9Chin Reconstruction
Abstract
The chin is a midline cosmetic subunit in which cutaneous malignancies are common. Mohs micrographic surgery provides the highest cure rates and smallest defects after extirpation of these lesions. Preoperative assessment of the patient’s normal anatomy is an important part of surgical planning. Delineation of any pronounced landmarks helps with designing reconstruction. Further, understanding resting skin tension lines along the convex chin can help the surgeon fashion a repair that is cosmetically pleasing. The baseline anatomy of the patient and suspected cosmetic outcomes should be discussed with the patient as much as possible. Curvilinear primary closures are a mainstay for reconstruction. For defects spanning a large portion of the chin, advancement and rotation flaps are excellent options and likely the most commonly used flaps. While larger defects may require transposition flaps harvested from adjacent submental neck or the skin of the jaw, care should be taken to take note of typical locations of the marginal mandibular nerve. Taking care to use sufficient undermining, release from the mentalis muscle near the wound edge and appropriate eversion of the wound edge will result in the best outcomes.
Keywords: chin, mental crease, labiomental crease, mental nerve block, marginal mandibular nerve
Capsule Summary and Pearls
•Delineate the labiomental crease and any mental cleft that is present prior to infiltration of local anesthetic.
•Assess thickness and mobility of the skin prior to infiltration of local anesthetic.
•Align linear closures to fit the convex contour of the chin when it is pronounced.
•Elongate Burow’s triangles to account for a pronounced convex chin. This may include extending the removal of a standing cone to the submental neck.
•Avoid crossing the labiomental crease with suture lines to avoid upward displacement of the vermilion.
•With deeper defects, avoid crossing the mandible to prevent tethering of the scar to the underlying menton.
•Rich muscular anatomy and anastomosing blood supply allow for durable flaps if undermined in the appropriate plane on the chin.
•The marginal mandibular branch of the facial nerve lies lateral to the chin and should be avoided for larger reconstructions utilizing this tissue reservoir.
9.1 Relevant Anatomy
The chin is formed by a projection in the anterior-most portion of the mandible. It is bordered by the labiomental crease superiorly and the inferior extension of the nasolabial folds (or marionette lines) laterally (Fig. 9.1). The nasolabial folds generally become more obvious in older patients with more pronounced skin laxity. The lack of significant nasolabial folds or marionette lines in younger patients makes the lateral borders of the chin more ambiguous. The inferior border of the chin is defined by the inferior border of the anterior mandible. The chin has a variably, but generally dense fibrous subcutaneous tissue mass with insertions of the mentalis muscle, which originates from the medial portion of the mandible at the lateral incisors. This muscle wrinkles the skin of the chin and helps protrude the lower lip. Other muscles in this area include the inferior portion of the orbicularis oris superiorly, the depressor anguli oris, and the depressor labii inferioris laterally. The inferior border of the chin includes the medial insertions of the platysma muscle.
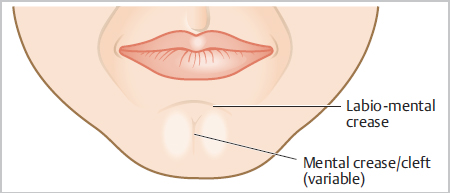
Fig. 9.1 Basic surface anatomy of the chin.
Resting skin tension lines follow a generally curvilinear or sickle-shaped course curving laterally along the rounded convex axis of the protruding mental prominence. The most obvious line of the lower face is often the labiomental crease, which should be identified prior to infiltration of local anesthetic. This line is of utmost importance in designing repairs of the chin. A natural surface anatomy feature of importance is the mental cleft, when present. This too should be identified with markings prior to infiltration of anesthetic. When linear closures and scars cross this line, an obvious and lasting deformity generally ensues, pushing the lower vermilion border upward and obliterating the labiomental crease. The lateral borders include a variable nasolabial fold or marionette line.
Danger zones of the chin include the inferior labial arteries superiorly and the marginal mandibular nerve at the most lateral portion. These are unlikely to be encountered on the chin proper. It is also important to note that the labiomental crease is the inferior border of the lower cutaneous lip, which has variable thickness. The oral cavity can lie less than 1 cm from the skin at this point. When considering repairs for the chin, the lateral tissue reservoirs do contain the marginal mandibular nerve, and thus it should be identified by surface landmarks during design of reconstruction. On the chin proper, one may encounter the V3 branch of the trigeminal nerve (mental nerve), which provides sensory innervation to the chin and lower lip. The presence of this nerve root offers and easy solution to anesthesia via regional block of this area and can be utilized for patient comfort.
9.2 Aesthetic Subunits and Defects
Aesthetic subunits and defects are shown in detail in Fig. 9.2, Fig. 9.3, Fig. 9.4, Fig. 9.5, Fig. 9.6, Fig. 9.7.
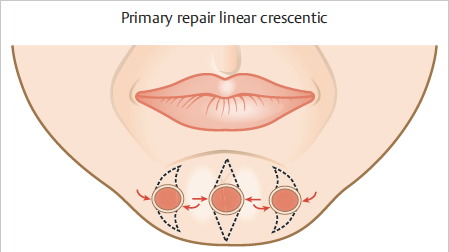
Fig. 9.2 Primary repair options. Midline defects with vertical closures. Lateral defects with curvilinear or crescentic closures.
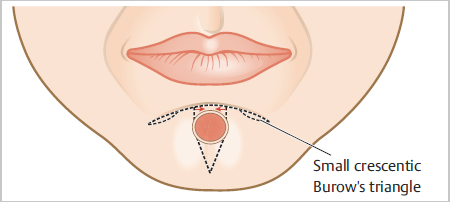
Fig. 9.3 O-T advancement flap. Note the small crescentic Burow’s triangles along the sliding edges of the flap to eliminate length discrepancy and bunching of the standing edge. Note the desire to place the horizontal line along the labiomental crease.
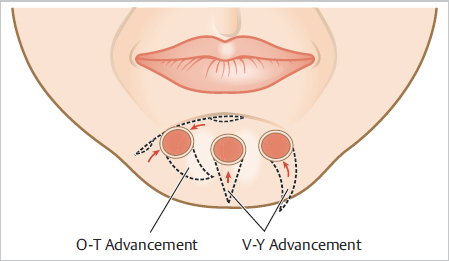
Fig. 9.4 V-Y advancement. Good option for midline defects and lateral defects. Note the curvilinear V used for the lateral defect designed toward midpoint of the chin. O-T advancement flap for defect lateral to midline.
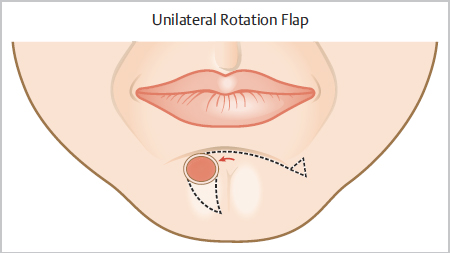
Fig. 9.5 Unilateral rotation flap. Note the arc extends along the labiomental crease and the standing cone is removed along the relaxed skin tension line of the lower lip or along the marionette line or from beneath the mandible if tissue is mobilized inferolateral to defect.
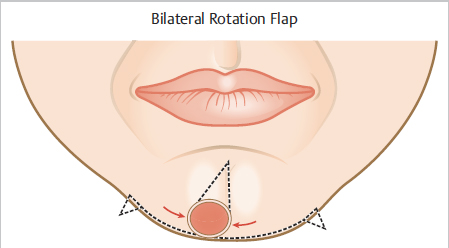
Fig. 9.6 Bilateral rotation flap. Standing cones removed from the area just inferior to the mandible at equal distances to maintain symmetry. This could also be considered an O-T advancement flap depending on the rotational or straight-line vector of tissue movement.
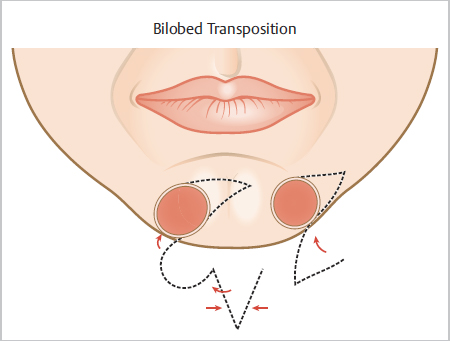
Fig. 9.7 Transposition flaps. Bilobed transposition offers the option of hiding secondary and tertiary defect scars on the submental area. A single lobe transposition can also be tailored to hide secondary defect scars in multiple locations below the mandible.
9.3 Reconstructive Options
9.3.1 Algorithm
•Primary (side-to-side) closure: Primary closures should not cross the labiomental crease if at all possible. Upward distortion of the lower lip can occur when the labiomental crease is crossed.
•Bilateral advancement flap (O-T): Note this may have a component of rotation due to the convex nature of the chin and curved mental crease (this is a “go-to” flap for the chin).
•V-Y advancement/island pedicle flap.
•When there is lack of enough tissue laxity for above repairs:
–Unilateral or bilateral rotation flap (bilateral is reserved for defects near the midline).
–Inferiorly and laterally based transposition flap/bilobed flap.
–Full-thickness skin graft.
9.3.2 Healing by secondary intention
The chin can heal very well when defects are shallow and broad. This may be suitable for all shallow defects but is most practical for defects that are too broad for primary closures and are shallow. If the defect is partial thickness and present in a man that normally grows a beard, it may be the preferred option for this location. If the defect includes subcutaneous fat, or obliterates follicular structures, a closure is likely the better option. Delayed repair after secondary intention healing can be a consideration for defects smaller than 1cm and no more than 3 to 5mm in depth. By allowing healing, the patient and clinician can assess the appearance and decide if closure is preferred. Facial hair preferences can change; thus, scar appearance on a clean-shaven face should be considered.
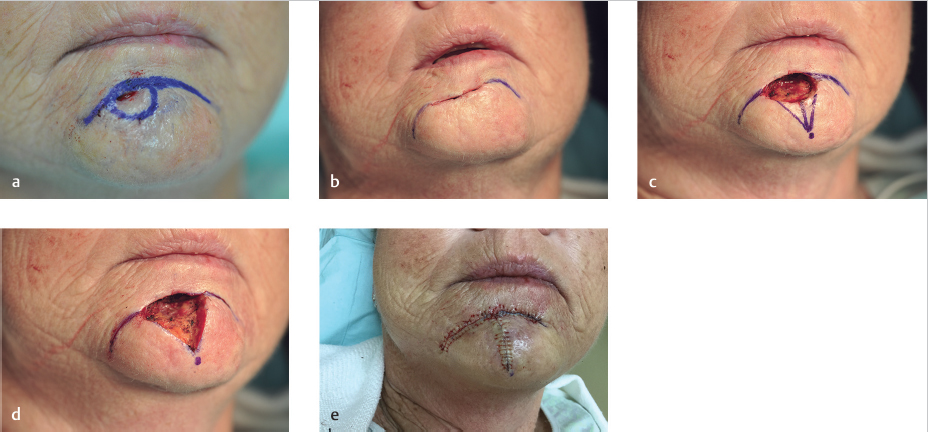
9.3.3 Primary closure
Primary closures on the chin are a mainstay for many Mohs defects. Midline or near-midline defects are common, and primary linear closures are common. Lateral defects will often appear better with a curvilinear design when oriented in a vertical fashion. This is best facilitated with the use of two concave lines on the medial side and a longer convex line on the lateral side (see Fig. 9.2). It is important to have the inner curve equal the length of the outer/broader curve by creating two concave lines on either end of the defect. Otherwise, the curve will have two skin edges of unequal length, leading to redundancy on the longer side. Undermining widely through the fibrous attachments of the mentalis muscle will facilitate movement of the edges of the defect and reduce tension on the wound. Insufficient undermining may result in a dimpled or depressed scar in this location due to the muscular attachments into the dermis.
Primary closures should not cross the labiomental crease. If a primary closure will require crossing this crease, it should be altered in some way. This will generally make an O-T flap the best option. Similarly, if the primary closure will cross the mandibular prominence inferiorly, it may result in tethering of the scar at this prominence. A bilateral advancement flap with inferior incisions along the mandibular border will provide less likelihood of tethering at the bony prominence, which can cause an unappealing visible difference from the frontal view.
Some defects may lend themselves to closure horizontally, or slightly angled. These are generally an exception to the rule that primary closures oriented vertically have a better long-term outcome. However, patients can have differing facial contours, laxity, and defects. As with any primary closure, it is sometimes advantageous to undermine the circular defect in all directions and assess where the natural skin tension vectors “want” to close the defect. Burow’s triangles should be long enough to account for the convexity of the chin. Otherwise, standing cone deformity is visible from many angles.
9.3.4 Bilateral Advancement (O-T flap)
The O-T flap (bilateral, single tangent flap) is a go-to flap for chin repairs (see Fig. 9.3, Fig. 9.8, and Fig. 9.9). Often, the convexity of the chin requires removal of longer dog-ears, and often, they will extend through the labiomental crease. Whenever the defect requires removal of a dog-ear that will cross the labiomental crease, the crease should be used as the line that defines the superior border (or the horizontal incision) for an O-T flap. This crossing arm of the “T” will often be curvilinear, following the crease. This at times will appear more consistent with a bilateral rotation flap. If a defect is closer to the inferior border of the chin, the O-T flap can be flipped so that the horizontal line of the T is along the inferior border of the mandible (see Fig. 9.6). The inferior dog-ear should ideally not cross the most inferior edge of the mandible. Crossing this prominence can lead to tethering of the scar to the bony prominence. A tethered appearance is not a certainty, and linear closures can often produce very acceptable outcomes. If a defect is sizable enough that an inferior dog-ear should cross onto the submental neck, and the superior dog-ear would cross the labiomental crease, one should consider a bilateral double tangent (O-H) flap. Horizontal lines can hide well within the labiomental crease and just under the chin on the submental neck. The O-T flap can be tailored to the site regardless of whether it is midline, or more laterally (see Fig. 9.4). The vertical arm of the T should be designed toward the central point of the chin, much like the spokes of a wheel radiating from the hub (chin midpoint) to the outer wheel (mental crease). When defects do not fall on midline, the dog-ear should follow the curvilinear shape of the relaxed skin tension lines on the chin. Again, this is generally a sickle shape curving laterally at the most convex point.