12Perioperative Management and Wound Care
Abstract
Structured perioperative management and wound care is essential to successful surgical outcomes during Mohs micrographic surgery (MMS). At the authors’ institution, these structured protocols focusing on perioperative antibiotics, anticoagulation, conscious sedation/analgesia, and implantable cardioverter-defibrillators (ICD)/implantable devices are closely followed to ensure patient safety. A discussion of these protocols in a step-wise fashion with a review of the current literature is included in the following chapter to help the dermatologic surgeon use evidence-based medicine to support their decision-making process. Furthermore, an in-depth focus is provided on the management of dressings based on the following closure or procedural types: second intention wound healing, porcine xenografts, biologic dressings, dermabrasion, primary closure, postflap care, and postgraft care. These step-by-step dressing recommendations will help to provide a framework on the management of wounds following MMS. Even in the most skilled dermatologic surgeon’s hands, complications can arise including hematoma, infection, and postprocedural pain. A brief discussion on these postoperative complications with management recommendations is included.
Keywords: Antibiotic prophylaxis, anticoagulants, conscious sedation/analgesia, pacemakers/defibrillators, postdermabrasion care, postprimary closure care, postflap care, postgraft care, hematoma, infection, pain management
Capsule Summary and Pearls
•Highlight preoperative and postoperative considerations during Mohs micrographic surgery.
•Management of perioperative antibiotics, anticoagulation, conscious sedation/analgesia, and ICD/implantable devices.
•Management of dressings based on closure type.
–Second intention/granulation.
–Dermabrasion.
–Porcine xenografts and biologic dressings.
–Primary closure.
–Postflap care.
–Postgraft care.
•Approach to postoperative complications including hematoma and infection.
•Postoperative pain management.
12.1 Preoperative Considerations
12.1.1 Antibiotic Prophylaxis
Antibiotic prophylaxis, utilized to prevent surgical site infection (SSI), infective endocarditis (IE), and hematogenous total joint infection, is an important consideration in Mohs micrographic surgery (MMS). The low rates of SSI, hematogenous total joint infection, and IE seen with MMS have led to guidelines that recommend against the routine use of prophylactic antibiotics. Despite the 2007 guidelines from the American Heart Association on the prevention of IE,1 the 2008 Journal of the Academy of Dermatology (JAAD) advisory statement on prophylactic antibiotics in dermatologic surgery,2 and the clinical practice guideline from the American Academy of Orthopaedic Surgeons-American Dental Association,3 studies show that antibiotics are used more than are recommended, which translates to an increased risk of adverse side effects and antimicrobial resistance.4 According to the JAAD advisory statement, the ultimate decision on the use of prophylactic antibiotics should be tailored to each individual patient’s clinical scenario; however, the following four factors should be considered2:
1.Skin condition (infected vs. noninfected).
2.Anatomic site (high risk vs. low risk of SSI).
3.Type of procedure.
4.High-risk cardiac conditions or high risk of prosthetic joint infection.
Bacteremia, the predisposing factor for IE and hematogenous total joint infection, can occur via two ways in dermatologic surgery. Bacteria can be introduced intravascularly during a perforating procedure or can spread into the vasculature from an infected surgical site. Perforating dermatologic procedures are defined by invasion or immediate destruction of the epidermis or mucosa and include MMS, excision, biopsy, ablative laser, incision and drainage, and electrodessication and curettage. Nonperforating procedures include cryotherapy and nonablative laser. Pooled studies have shown a low rate of bacteremia of 1.9% during dermatologic procedures on clinically noninfected, eroded, or intact skin.2 This low risk of bacteremia is comparable to the rate of bacteremia during daily activities and therefore argues in favor of reduced routine utilization of prophylactic antibiotics.1,2 Cutaneous infection has been attributed as the likely cause of cases of IE and as many as 50% of late onset hematogenous total joint infections, highlighting the importance of assessing the risk for SSI and prompt, aggressive treatment of cutaneous infection, especially in patients with high-risk features for IE and prosthetic joint infection.2 Procedures involving infected skin should be postponed until the infection has been treated. If surgery on infected skin is necessary, the patient should be covered by empiric antibiotics.
In addition to minimizing the risk of bacteremia to prevent IE and prosthetic joint infection, antibiotic prophylaxis should also be utilized for areas and cases in which an SSI may result in adverse outcomes, such as graft or flap failure on the nasal tip resulting in poor cosmesis. Antibiotic prophylaxis should also be considered in prolonged procedures as studies have demonstrated an increased infection rate in this setting.5
We will discuss the indications for prophylactic antibiotics in MMS and provide recommendations on antibiotic selection and administration.
Prevention of Infective Endocarditis
According to the 2008 JAAD advisory statement on antibiotic prophylaxis in dermatologic surgery, antibiotic prophylaxis is recommended in three circumstances to prevent IE and nonvalvular cardiovascular device-related infection:
1.Procedures on infected skin.
2.Any breach of the oral mucosa in the setting of high-risk cardiac conditions.
3.For sites that are at a high risk for SSI.2
High-risk cardiac conditions as defined by the American Heart Association Guidelines are outlined in Table 12.1,1,2 and surgical sites or techniques with a high risk of SSI are shown in Table 12.2.2,6,7
Table 12.1 High-risk cardiac conditions that warrant prophylactic antibiotics in perforating dermatologic surgery involving the oral mucosa or infected skin
History of infective endocarditis Prosthetic valve or prosthetic material for valve repair Cardiac transplant patients with valvulopathy Unrepaired cyanotic CHD First 6 months following repaired CHD with prosthetic material or device Residual defects in repaired CHD at site or adjacent to site of prosthetic patch or device Abbreviation: CHD, congenital heart disease. |
Based on the American Heart Association Guidelines on Prevention of Infective Endocarditis and Wright et al.2,8 |
Table 12.2 High-risk locations and techniques for surgical site infection that warrant prophylactic antibiotics in dermatologic surgery
Groin Lower leg Widespread inflammatory dermatosis Nasal flaps Skin grafts Wedge excision of the lip or ear Prolonged procedure, multiple sites |
Based on Wright et al, Dixon et al, and Maragh and Brown.2,6,7 |
Devices and prosthetics that do not warrant antibiotic prophylaxis include: pacemakers, defibrillators, peripheral vascular stents, coronary artery stents, central nervous system shunts, breast implants, and penile prostheses.2
Prevention of Hematogenous Total Joint Infection
Based on guidelines from the American Dental Association and American Academy of Orthopaedic Surgeons, the American Heart Association, and the 2008 JAAD advisory statement on antibiotic prophylaxis in dermatologic surgery, antibiotic prophylaxis should be used in the following three instances to prevent hematogenous total joint infection:
1.Procedures that breach the oral mucosa in high-risk orthopaedic patients as defined in Table 12.3.2,3
2.When the procedure involves infected skin.
3.With a technique or for area at high risk for SSI (Table 12.2).2,6,7
Guidelines do not recommend antibiotic prophylaxis in dermatologic surgeries on nonmucosal or noninfected skin, or locations or techniques that are not at a high risk for SSI. Orthopaedic pins, plates, or screws do not warrant prophylactic antibiotics.1–3
Table 12.3 High-risk features in patients with prosthetic joints that warrant prophylactic antibiotics to prevent prosthetic joint infection in dermatologic surgery
Within 2 years of joint replacement History of prior prosthetic joint infection Immunosuppression due to medication, radiation, inflammatory disease Type 1 diabetes Hemophilia HIV/AIDs Malignancy Malnourished state |
Based on Wright et al, American Dental Association and American Academy of Orthopaedic Surgeons guidelines on prevention of prosthetic joint infection.2,3 |
Surgical Site Infection
SSI is defined as postoperative infection at the operative site. Table 12.2 shows procedure locations and techniques which have been found to have a high risk for SSI and therefore warrant prophylactic antibiotics to prevent potential local complications and bacteremia from infection.2,6,7 These sites are thought to be at high risk for SSI due to increased microbial burden.9 These high-risk locations were determined from large studies that evaluated reported overall cutaneous surgical infection rates, which generally range from 0.7 to 8.7% of cases.7,8,9–,10,11,12-13 A prospective study by Maragh and Brown found an overall low rate of SSI of 0.7% for Mohs surgery.7 Of these infections, a large percentage occurred on the nose. The ear has also been found to have a high infection rate.14 Studies have shown that SSIs were more likely in patients with immunosuppression, diabetes, widespread inflammatory disease due to colonization with Staphylococcus aureus, hematoma formation, in malignant vs. benign lesions, procedures in the groin or lower extremity, and flap or graft reconstruction.2,10,12,13 In the editor’s experience, in the case of lower extremity SSI or threatened dehiscence, it may be useful to use a tetracycline-based antibiotic-like doxycycline, along with wound care and compression.15
It is believed that endogenous flora are responsible for the majority of SSIs.16 Colonization with S. aureus and the increasing incidence of methicillin-resistant Staphylococcus aureus (MRSA) are a known cause of SSI.17 Evaluation for S. aureus nasal carriage can help to predict those at an increased risk for postoperative wound infection. Approximately 37% of the population is a carrier of S. aureus.18 While the anterior nares are easily accessible and are typically the highest colonized site, extranasal reservoirs include the pharynx, axilla, and groin.16 Studies showed that carriers of S. aureus who underwent topical decolonization including topical mupirocin and chlorhexidine gluconate wash for 5 days had fewer SSIs when compared with patients who received perioperative antibiotics or no treatment.16,18 In the setting of an overall low infection rate, the individual practitioner will have to determine whether the preoperative testing and treatment of S. aureus are cost effective and feasible given the time and labor involved.
Prophylactic antibiotics can be delivered pre-, intra-, and postoperatively; however, it is ideal to have the antibiotic present in the bloodstream at the procedure site prior to incision as it is believed that antibiotics delivered preoperatively are more effective as they are incorporated into the wound, which does not occur with postoperative administration.5
Topical antibiotics have been studied for the prevention of SSI, given the ability to deliver high levels of drug directly to the operative site while avoiding the adverse effects of systemic antibiotics. Their ointment base also provides a moist wound environment, which promotes healing. Studies have shown no statistically significant difference in SSI with the use of petrolatum compared to topical antibiotics.19,20,21 Topical antibiotics are also associated with adverse effects including contact dermatitis, anaphylaxis, and drug reactions. In addition, their use adds an unnecessary cost and promotes antimicrobial resistance.19–21 Therefore, the use of petrolatum is recommended on postoperative dermatologic wounds.
Perioperative Antibiotic Prophylaxis Summary
The guidelines discussed above have been summarized into a chart adapted from Mayo Clinic’s Division of Dermatologic Surgery (Fig. 12.1).2,22 Ultimately the decision regarding the use of antimicrobial prophylaxis should be individualized, weighing the risks and benefits of antibiotic use specific to each patient’s clinical scenario.
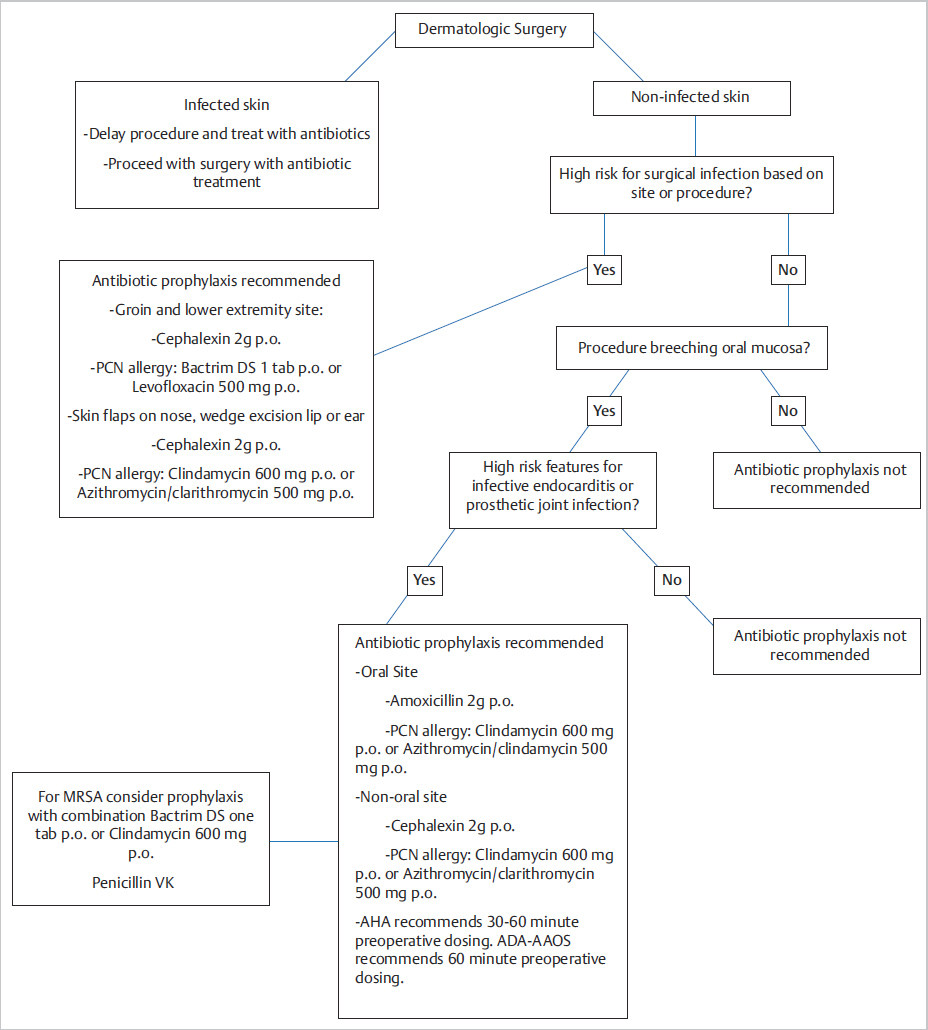
Fig. 12.1 Approach to antibiotic prophylaxis. Consider a longer duration of antibiotic treatment (7–10 days) in addition to the preoperative dose in high-risk situations. Based on Wright et al.2
12.1.2 Anticoagulants
Patients undergoing MMS often have medical comorbidities that necessitate the use of antithrombotics. Antithrombotics are divided into two classes, anticoagulants, which inhibit thrombin generation and fibrin formation, and antiplatelets, which block platelet activation and aggregation.23 Knowledge of these agents is important as many patients undergoing MMS are on one or multiple antithrombotic agents concomitantly and novel anticoagulants are continually being developed. Given an estimated 46% of patients undergoing cutaneous surgery are on at least one anticoagulant or antiplatelet agent, the proper perioperative management of these medications is critical to prevent adverse outcomes and even death.24
The decision of whether to stop antithrombotic agents in the perioperative period requires assessment of the risk benefit ratio of developing potential thrombotic events such as stroke, myocardial infarction, and pulmonary embolism, while minimizing intra- and postoperative hemorrhage. Blinded observers of cutaneous surgeries demonstrated that visual inspection of intraoperative oozing was not predictive of antithrombotic status.25 Studies evaluating perioperative antithrombotic use in cutaneous surgery have shown only minor bleeding complications when antithrombotics were continued, while many cases of thrombotic events were reported with antithrombotic cessation, even for a short duration.23,26–26 In addition to the complications arising from antithrombotic cessation, the blood work and testing required upon medication reinitiation adds additional cost.29
Brief interruption of antithrombotic therapy, typically 3 to 14 days prior to surgery depending on the agent, is a common method to attempt to balance potential perioperative bleeding and thrombotic events. In a study by Otley et al, only 1.6% of patients who underwent MMS or excision while on warfarin or platelet inhibitors developed severe complications.30 This was comparable to that seen in the control group who were not on antithrombotics.30 In addition, those who had their antithrombotic held perioperatively did not experience a statistically significant reduction in the rate of severe complications.30 Several other studies found similar results with antithrombotic continuation and did not see a significant increase in complications such as hematoma formation with associated necrosis, dehiscence, or infection.29,31,32,33,43
Although some studies have demonstrated an increase in severe hemorrhagic complications in patients taking warfarin or clopidogrel, these complications were non-life-threatening.35,36,37 As expected, those taking more than one antithrombotic agent are at an increased risk of postoperative bleeding.38 Cutaneous surgery is often postponed when an international normalized ratio (INR), typically checked within 24 hours of surgery for patients on warfarin, is greater than 3.5. If the INR is supratherapeutic, then the dermatologic surgeon should have a discussion with the patient regarding the trends of his/her INR in order to determine the need for close follow-up with the patient’s primary care provider.
Consideration has been given to the use of unfractionated heparin as a bridge during the temporary interruption of anticoagulant therapy in order to shorten the duration of thromboembolic risk. No reduction in hemorrhagic complications was seen with this approach. Instead, this led to hospitalizations and increased blood work.33 The low-molecular-weight heparins have a more predictable biologic response when compared to unfractionated heparin and therefore do not require laboratory monitoring; however, their safety during cutaneous surgery has not been well characterized.39
Chang et al also studied patients undergoing cutaneous surgery who were taking the novel oral anticoagulants (nOAC) Rivaroxaban and Dabigatran and found no severe hemorrhagic complications in patients on these agents.40 Novel anticoagulants have been reported to have an increased risk of postoperative hemorrhagic complications compared to all other anticoagulants combined; however, these complications were mild in severity.24 Therefore, despite a possible increased risk for postoperative bleeding, it is recommended that patients be maintained on their nOAC when undergoing MMS. A recent study reviewing a complication rate at one institution suggested that perioperatively interrupting nOAC may be safe and efficacious. They also briefly reviewed nondermatologic literature and guidelines, where a similar interruption to nOAC was recommended.41
In addition to a review of antithrombotics, attention should be given to the use of supplements, such as vitamin E and fish oil, which can possess intrinsic anticoagulant properties and may increase blood pressure, thereby contributing to bleeding.40,42 Given that evidence-based studies regarding the management of these supplements are lacking, the decision regarding their perioperative use is at the discretion of the individual provider.27
Discontinuation of antithrombotics can be associated with patient discomfort in the case of nonsteroidal anti-inflammatory drugs (NSAIDs) utilized for pain. In these cases, acetaminophen, in the appropriate clinical context, may be substituted for pain control. At the authors’ institution, we currently advise against using NSAIDs during the first 72 hours, given the increased risk of postprocedural bleeding in comparison to that of acetaminophen. Given that there is newer emerging evidence to suggest that better pain control is achieved when adding NSAIDs to acetaminophen in the postoperative period, the dermatologic surgeon must consider the utility of adding NSAIDs in the postprocedural period at the theoretical risk of increasing bleeding on a case-by-case basis.
As a result of numerous studies which demonstrate potential life-threatening thrombotic events with discontinuation of antithrombotics and the relative lack of major complications with antithrombotic continuation during cutaneous surgery, we strongly recommend that cutaneous surgeons maintain patients on their current antithrombotics, which is the practice at the authors’ institution. If taken for preventative purposes, aspirin and aspirin-containing products can be discontinued 7 to 10 days before surgery.23,29,43
It is important to recognize that certain techniques predispose a patient to a higher risk of bleeding. In comparison to linear closures, flaps and full-thickness skin grafts have a higher hemorrhagic complication rate even when factors including age, sex, postoperative size, and anticoagulation status are controlled. Extensive undermining is thought to account for the increased bleeding and hematoma formation.24 Therefore, use of plication sutures and other techniques to minimize cutting tissue should be considered. To prevent postoperative bleeding, emphasis should be placed on careful intraoperative hemostasis, the application of proper pressure dressings, patient education on minimizing physical activity in the postoperative period, and management of postoperative bleeding.
Recent guideline updates in 2017 from the American Academy of Cardiology have suggested holding direct oral anticoagulants (DOACs), such as apixaban, dabigatran, and rivaroxaban, 24 hours prior to procedures with low risks of bleeding.44 Siscos et al performed a retrospective chart review over a 4-year time period at a single center where they found that among their 750 Mohs micrographic surgery procedures, 1 patient experienced a transient ischemic attack (TIA) and 2 patients experienced a hematoma and minor bleeding in the 30-day postoperative period when holding their DOACs for surgery.45 The DOACs were held 24 hours prior to their Mohs micrographic surgery and resumed 1 day after surgery with only three minor complications.45 Randomized controlled trials and further studies are needed to determine the appropriateness of holding DOACs in the perioperative period for Mohs micrographic surgery.
12.1.3 Conscious Sedation/Analgesia
Conscious Sedation
Given that the majority of MMS cases are performed on the face with a case length typically exceeding 2 hours, dermatologic surgeons are faced with the challenge of reducing patients’ anxiety. The advantage of local anesthesia becomes increasingly evident with the number of comorbidities for the typical patient undergoing MMS. At the authors’ institution, the administration of oral midazolam as an anxiolytic and sedative has helped maintain the focus on patient-centered care during surgery without the distraction of an overly anxious patient. Midazolam, a benzodiazepine, acts on the benzodiazepine receptor located on the postsynaptic GABA neurons of the central nervous system.46 The focused targeting of the GABA-A receptors in the central nervous system has allowed for numerous providers across specialties to use this medication as a tool for anxiolysis, antegrade amnesia, and light sedation.47 In comparison to diazepam, midazolam has a quicker onset of action and a shorter half-life.48 In a meta-analysis from nine trials involving 587 patients, only 58 of the 296 patients who received midazolam could recall the procedure while 140 of 291 patients who received diazepam had recollection of the procedure (RR 0.45, 95% CI 0.30–0.66).49 The onset of action for midazolam is typically 10 to 20 minutes with a peak effect at 30 to 60 minutes after administration.46 Although hepatic and renal disease may impede excretion of the medication leading to increased sedation, the half-life is typically 3 hours. Midazolam has often been utilized by gastroenterologists as an anxiolytic during flexible sigmoidoscopies; however, it does not reduce actual pain. As was seen by Kuganeswaran et al, in comparison to placebo, patients’ anxiety, and perceived comfort was significantly lower with 7.5-mg midazolam PO thought to be due to the amnestic effect of benzodiazepines.50 There are limited randomized controlled studies on MMS using oral midazolam; however, Beer et al51 in a randomized, double-blind prospective study during facial procedures under local anesthesia compared the patient reduction in anxiety when administered clonidine, midazolam, morphine, or placebo.48 Although a small sample size of 150 patients were in the study, midazolam and clonidine were found to reduce anxiety during facial plastic procedures performed under local anesthesia.48 The patients treated with midazolam had increased risk of respiratory depression.48 In Otley et al, they found during 11 episodes of conscious sedation while treating 8 pediatric patients undergoing excision or pulsed dye laser (PDL) therapy that the combination of oral benzodiazepine with inhaled nitrous oxide (35–50%) with oxygen via nasal cannula resulted in an adequate level of sedation while performing the procedures.52 As was mentioned in their study, minimal side effects of nausea were experienced; however, the use of conscious sedation must be performed in a closely monitored procedural setting with practitioners who are certified with basic and advanced cardiopulmonary life support, access to a crash cart, and training in case respiratory or cardiac depression occurs.52 During our cases we do not routinely use nitrous oxide, given that the adult population responds well to monotherapy with midazolam to ease their anxiety. The advantage of oral midazolam with or without inhaled nitrous oxide is the swift ease of onset and lack of needing intravenous access.
Given the known risk of respiratory depression with benzodiazepine use, a strict protocol is followed during all MMS cases performed at the authors’ institution. Following rooming of the patient, review of the patient’s preoperative questionnaire, and vital signs, the Mohs surgeon assesses the possible need for anxiolysis. If the patient meets criterion for midazolam, the surgeon confirms the dosage with the nurse (typical starting dose ranges from 5 to 10 mg). Factors taken into account to decide on an appropriate starting dose include: history of pulmonary disease (i.e., COPD), sleep apnea, supplemental oxygen dependence, renal and hepatic disease given excretion of the medication, age of patient, low body weight, fall risk, and medication list. In these high-risk patients, a lower dose by half or one-third is safer and may require longer onset of action than higher doses. If a patient does not have a family member or friend present on the day of surgery, midazolam will not be administered for patient safety. Given that the risk of respiratory depression and level of sedation are increased if the patient is also on opioid-based medications, we typically do not administer benzodiazepines in this case. Although unlikely in light sedation if ventilation was compromised, the benefit of midazolam and other benzodiazepines is that flumazenil may be administered to improve spontaneous ventilation. If hypoxia does occur, it is recommended based on the guidelines to (1) encourage the patient to take deep breaths, (2) start the patient on supplemental oxygen, (3) administer positive pressure ventilation, and (4) observe the patient following reversal with flumazenil.53
The baseline vital signs are obtained including blood pressure, pulse, and oxygen saturation. Patients either have a nurse or a family member in the room while the tissue is processing to ensure that the patient is never unattended. Repeat vital signs are obtained after every dose administration and prior to discharge from the clinic. The Richmond Agitation-Sedation Score (RASS) is calculated by the nurse prior to departure with a goal of 0 to −1. All providers and nurses are trained and certified in basic and advanced cardiac lift support and have access to a crash cart in the clinic. Patients are advised to not drive, operate heavy machinery, or take any sedating medications or alcohol for at least 24 hours to reduce the risk of central nervous or respiratory depression. In our experience, midazolam is a useful tool for eyelid or large central facial cases.
Analgesia
Adequate control of a patient’s discomfort during and after surgery is considered a high priority during MMS. As part of the preoperative questionnaire given to patients on the day of surgery, the presence of pre-existing pain and the patient’s postprocedural pain threshold are reviewed. If the patient highlights that they have pre-existing pain or a low pain threshold, this is further addressed in depth with the nurse and surgeon. During the informed consent, the provider discusses with the patient that we recommend acetaminophen for postprocedural pain for the first 48 to 72 hours. As is standard for the majority of Mohs surgeons, we infiltrate the marked surgical site in the superficial subcutaneous tissue with a 30-gauge syringe with lidocaine 1% with epinephrine (1:200,000). Pertinent guidelines for the use of local anesthetics in dermatologic surgery are summarized in Table 12.4.52 The nurse pays special care to not go through the clinically evident tumor to avoid floaters during tissue removal. Following removal of the first and every subsequent stage, the nurse provides additional local anesthesia with subcutaneous infiltration of lidocaine 1%, bupivacaine 0.25%, and epinephrine (1:200,000) in a 2-mL syringe to allow for better pain control during tissue processing. Benzodiazepines increase the seizure threshold and allow large doses of lidocaine to be given safely without toxicity symptoms. The extended time period over which the local is administered between Mohs layers and before reconstruction also reduces toxicity risks. Cardiac monitoring should also be provided with large doses of bupivacaine. For very large cases such as dermatofibroma sarcoma protuberans or melanoma excisions, we often utilize tumescent anesthesia based on the components as seen in Table 12.5. As recommended ways to reduce pain during tumescent administration, inject slowly and injecting room-temperature or slightly warmed solution is helpful. Furthermore, buffering the acidic solution with bicarbonate also reduces the burning sensation experienced during administration.53
Table 12.4 Pertinent extracted recommendations based on AAD guidelines for Mohs micrographic surgery
Local anesthesia type | Maximum amount to use (adult) |
Lidocaine without epinephrine Lidocaine with epinephrine Tumescent anesthesia Multistage procedure such as MMS | 4.5 mg/kg 7 mg/kg 55 mg/kg Do not exceed 500-mg lidocaine |
Abbreviation: MMS, Mohs micrographic surgery. Based on Kouba et al.52 | |
Table 12.5 Formula of tumescent we use for larger cases such as DFSP or deeper tumors
Ingredient in tumescent mixture | Quantity in tumescent mixture |
1% Lidocaine Epinephrine Sodium bicarbonate Normal saline (0.9%) | 1,000 mg 1 mg 12.5 mEq 1,000 mL |
Abbreviation: DFSP, dermatofibrosarcoma protuberans. | |
Following the procedure, based on the presence of large facial flaps or surgical defects in which the patient has a low pain threshold, a typical prescription given to patients is tramadol 50-mg tablets one to two tablets every 6 hours with a total number of six pills. Based on the increasing misuse and dependence on opiate-based narcotic pain medications, we do not routinely prescribe alternative controlled substances which are beyond the scope of this chapter. Patients are provided the call number for the resident and surgical fellow on call in case pain is not controlled following normal business hours.
12.1.4 Implantable Devices
Pacemakers/Defibrillators
Prior to and throughout surgery, the provider must ensure adequate work-up and management of implanted devices including cardiac, deep brain stimulator, and cochlear implants to ensure that no harm comes to the patient or their device. Implantable cardioverter-defibrillators (ICD) are devices that have revolutionized medicine to terminate ventricular tachycardia (VT) and ventricular fibrillation (VF).54 Sustained VT and VF can lead to sudden cardiac death; thus, it is imperative that cauterization methods used during surgery do not interfere with the ICD function. A pacemaker can electrically stimulate or pace the heart with the newer models having the option to detect intrinsic cardiac activity.55 The indications of ICD/pacemaker placement is beyond the scope of this chapter; however, certain characteristics increase the risk for electromagnetic interference (EMI) as seen in Table 12.6.56
Table 12.6 Characteristics affecting electromagnetic interference (EMI) during dermatologic surgery
Proximity of electrosurgical device to implantable device Length of pulse delivery of electrosurgical device Lead placement (left-sided unipolar are at higher risk of sensing EMI) Noise protection algorithms ICD has increased sensitivity during pacing onset when there are absent sensed complexes in order to detect fine VF Patient’s level of dependence on pacemaker |
Abbreviations: EMI, electromagnetic interference; ICD, implantable cardioverter-defibrillators; VF, ventricular fibrillation. Based on Pinski SL, Trohman RG.56 |
Newer ICDs have protective fields in which nonphysiologic EMI leads to asynchronous pacing.55 Sustained asynchronous pacing has the increased risk of producing tachyarrhythmias.55 Similarly, newer cardiac devices have an insulated, sealed stainless steel or titanium case that reduces the distance between the electrodes.57 The guidelines by the Heart Rhythm Society (HRS) and the American Society of Anesthesiologists (ASA) recommend the following: patients who are pacemaker dependent with a pacemaker, patients with an ICD and pacemaker dependent, or patients with an ICD and not pacemaker dependent, use short electrosurgical bursts less than 5 seconds with magnet placement for procedures above the umbilicus and cardiac monitoring during the procedure.58 For nondependent patients with a pacemaker the magnet may not be required. Across dermatologic surgery there are various approaches to managing patients with ICDs and pacemakers. Per a survey administered to American College of Mohs Micrographic Surgery and Cutaneous Oncology (ACMMSCO) members, common practices of 166 members included using short bursts less than 5 seconds duration (71%), individual present with ACLS certification (68%), use of minimal power (61%), avoid use around device (57%), place grounding plate away from path of heart (37%), use bipolar forceps (19%), deactivate ICD (15%), and obtain a cardiac consultation (11%).59 Given the diverse responses, it becomes evident that there is no clear consensus among dermatologic surgeons. Common side effects from EMI during dermatologic surgery results include altered mental status, palpitations, syncope, and hemodynamic instability.59 Given the complexity and diversity of devices, the recommendation at our institution is to have the device interrogated either prior to or on the morning of surgery. Since 2000, when Mohs surgery orders are placed into our electronic medical record system, it automatically sends the pacemaker clinic (a part of the cardiovascular medicine division) notification that a device will need further investigation. Depending on the specifics of the device and the procedure, anatomic location and duration, the pacemaker clinic will make recommendations based on the telephone interrogation (or rarely in person) from their evaluation of the device. Continuous cardiac monitoring is performed by a registered nurse who is ACLS trained with appropriate postprocedural analysis of the device. Based on recommendations from the HRS and ASA, it is recommended that for elective procedures that the patient have had their pacemaker interrogated within the last 12 months and their ICD (if applicable) within the last 6 months.58 If in the unlikely event the EMI results in the need for defibrillation, it is advised to place the paddles 15 cm away from the device and place them in an anterior-posterior manner so that the electric field created with the shock is perpendicular to the leads of the implantable cardiac device.60
Five main types of electrosurgery are encountered in dermatologic surgery including electrodesiccation, electrofulguration, electrocoagulation, electrosection, and electrocautery. Electrodesiccation and electrofulguration are high frequency and low ampere methods to achieve hemostasis during surgery. Electrodesiccation involves direct contact with the electrode tip and the tissue whereas electrofulguration involves holding the electrode tip approximately 1 to 3 mm from the area being treated resulting in a visible spark. Advantages for these two methods of monoterminal electrosurgery include that the current is lower so there is both less tissue destruction and the patient acts as a ground. Contrastingly, electrocoagulation and electrosection have higher ampere and lower voltage resulting in increased tissue destruction and requiring the patient to be grounded. In order to reduce the likelihood of EMI, it is recommended to ground the patient to avoid having the device in the path. For example, if surgery were to be performed on the right arm, it would be recommended to ground the patient on the right lower extremity rather than the contralateral arm or leg. True electrocautery with a hot wire tip is not commonly used in dermatologic surgery, given the need for hemostasis for larger caliber vessels, but this method is less likely to cause interference, given that it uses thermal energy instead of electrical. Per a retrospective chart review at Mayo Clinic for the years 2001 to 2004, 173 patients with pacemakers and 13 with ICDs who underwent dermatologic surgery had no complications related to electrosurgery.61 Although the authors’ institution has the benefit of a pacemaker clinic allowing for pre- or postprocedural device interrogation, this study supports the use of bipolar cautery to reduce the risk of EMI during dermatologic surgery. Based on this study and general recommendations made by Dawes et al we recommend the following: (1) Ensure appropriate work-up investigation regarding the device type including if patient is pacemaker dependent. (2) Cardiac monitoring and O2 saturation during the procedure by ACLS trained provider and staff. (3) Use bipolar forceps if possible. (4) Use short bursts less than 5 seconds in duration. (5) Discuss if use of magnet is appropriate during use of electrocautery. (6) Place the grounding plate in an anatomic position to the electrocautery tip to limit the flow of current in the path of the device. (7) Have access to a crash cart. (8) Ensure that device is investigated postprocedurally and do not take off monitoring until device is restored to its original settings.61,62
Deep Brain Stimulators
With the aging patient population, deep brain stimulators are also increasingly encountered in patients undergoing MMS. Given that some of the main features of Parkinson’s disease include a resting tremor, muscular rigidity, and slower movements, a deep brain stimulator has helped to control the symptoms for patients who have Parkinson’s and other movement disorders.63 The deep brain stimulator is an implantable device with four electrodes implanted in the brain (specifically thalamus) and the neurostimulator located to the chest wall connected via a coiled wire. Settings are adjustable including the amplitude, width, and frequency of the pulse to reduce the motor symptoms in these neurologic conditions. Patients are able to turn the device on and off by using an external magnet to be placed over the neurostimulator implanted in the chest wall. Martinelli et al describe a case report of a patient with a deep brain stimulator for Parkinson’s undergoing MMS on the left ear for a squamous cell carcinoma in which no complications occurred with use of a battery-operated electrocautery device.64 Contrastingly, Weaver et al described a patient with a deep brain stimulator undergoing MMS for a basal cell carcinoma on the left cheek in which hemostasis was achieved with a hyfrecator (electrofulguration).65 With the use of the hyfrecator, the patient experienced the sensation of “electric shocks” on the ipsilateral arm and leg.65 Given the sensation, the surgeon switched to ophthalmic handheld battery-operated cautery which did not result in the symptoms that the patient had previously experienced with electrofulguration.65 Both of these case reports highlight the importance of screening for the presence of deep brain stimulators prior to surgery or use a magnet to turn the device off. If the underlying movement disorder would impede surgery with the device turned off, then the surgeon should consider using a battery handheld form of cautery that relies on thermal energy or bipolar forceps.
12.2 Postoperative Care
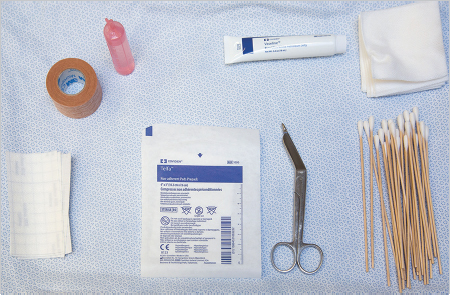
Following MMS, postoperative care varies based on the closure type. For all cases, photographs are obtained following the closure, and wound care is reviewed with the surgeon, nurse, and patient. As seen in Fig. 12.2, our standard tray to create a pressure dressing includes: normal saline, petrolatum jelly, cotton-tip-based application sticks, Telfa nonadherent dressing (Medtronic, Minneapolis, MN), 4 × 4 gauze, paper tape or Hypafix dressing (BSN Medical, Hamburg, Germany), and scissors. Patients are provided an educational pamphlet with the following instructions for daily wound care: