2Facial Subunit Reconstructive Principles and General Considerations
Abstract
Adhering to fundamental principles of surgical reconstruction and understanding tissue biomechanics are the keys to reliable reconstruction outcomes after Mohs micrographic surgery. Disregarding these fundamental principles leads to inconsistent outcomes or noticeable scars. This chapter will review guiding principles for facial reconstruction.
Keywords: reconstruction, design principles, tissue biomechanics, systematic wound assessment, flap, facial reconstruction
Capsule Summary and Pearls
This chapter will review fundamental principles of facial reconstruction design, tissue biomechanics, anatomy, and selection of reconstruction options.
•Fundamental principles of reconstructive design:
–To preserve and restore free margins and contour.
–To hide scars in cosmetic subunit junctions and relaxed skin tension lines.
–To optimize skin color and texture match.
•Fundamental principles of tissue biomechanics:
–Reconstructions to repair central facial defects favor tissue movement from lateral to medial locations.
–Reconstructions to repair lateral facial defects favor tissue movement from inferior to superior locations.
–Linear closures and sliding flaps have the greatest tension at the primary defect.
–Transposition and interpolation flaps transfer the greatest tension away from the primary defect to the tissue donor site.
–Ideal undermining planes vary with the anatomic location of the face and affect blood supply to flaps.
•Fundamental principles of anatomy:
–Blood supply to the face comes from both the external and internal carotid systems. Incorporating vessels into flap pedicles can improve blood supply and flap survival.
–The superficial musculoaponeurotic system (SMAS) protects the branches of the facial nerve.
•Fundamental principles to assess facial wounds and to select an ideal reconstruction:
–Define the missing anatomic layers in a defect and replace them with similar tissue whenever possible.
–Preserving free margins and contour is the top priority. Hiding scars in cosmetic subunit junction lines and relaxed skin tension lines and matching color and texture are secondary priorities.
–If wound edges can be approximated without tension or distortion of anatomy, linear closure or sliding flaps are usually possible.
–If approximating wound edges has high tension or distorts anatomy, transposition and interpolation flaps or skin grafts may be necessary.
2.1 Design Principles of Facial Reconstruction
2.1.1 Overview
We observe faces as we do highways: we disregard the expected; we notice the unexpected. Just as we ignore the characteristics of the highway until painted lines are altered or we encounter bumps or holes, we do not pay attention to facial scars unless they surprise us with unexpected lines or contours. The surgeon’s job is to leave scars that blend into the background and restore the expected contours of the face. In descending order of importance, the fundamental principles of reconstructive design are to preserve and restore free margins and contour, to hide scars in cosmetic subunit junctions and relaxed skin tension lines (RSTLs), and to optimize color and texture match with imported tissue.
2.1.2 Free Margins
The eyelids, distal nose, lips, and helical rim are “free margins” because they are unsupported on one side. These structures define our appearance, as demonstrated by the prominence of free margins in a facial sketch (Fig. 2.1). Preserving and restoring the free margins of the eyelids, the distal nose, the lips, and helical rim is a top priority during reconstructive surgery. Tension from reconstructive surgery or subsequent contraction from resulting scars can change the position of these delicate structures and create noticeable changes in contour and symmetry (Fig. 2.2). Strategies to preserve free margin position include orienting tension vectors parallel to free margins, transferring tension to tissue reservoirs remote from free margins,1 and tacking tissue to immobile deep structures so that dermal sutures near free margins are tension free.
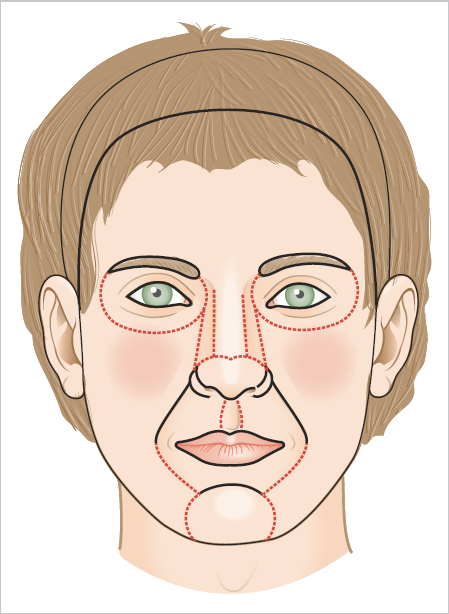
Fig. 2.1 Cosmetic subunits and free margins of the face.

Fig. 2.2 Patient with lateral ectropion of the left eye due to contracted scar tissue from prior repair. Malposition of the free margin causes conspicuous changes in appearance.
2.1.3 Contour
Contour determines how light reflects off our faces. Concavities (alar groove, medial canthus, philtrum) cast shadows; convexities (zygoma, tip of nose) reflect shiny light; and planar surfaces (cheek, forehead) reflect a subtle, even light. Unnatural contours on the face are noticeable because they interrupt the expected play of light. Too much volume (e.g., thick forehead flap on the nasal tip), too little volume (e.g., a skin graft in a deep defect), or failure to recreate natural contours (e.g., flaps that ablate the alar groove) will draw attention to these aberrations in facial contour (Fig. 2.3a–c). A top priority of reconstructive surgery is to recreate natural contours by filling wounds with tissue of similar surface area and thickness.

2.1.4 Cosmetic Subunit Junction Lines
Cosmetic subunit junction lines create natural shadows and reflections at transition zones between facial structures (Fig. 2.1).2,3 In complex cosmetic subunits such as the nose, further subdivisions are evident between the tip, dorsum, sidewalls, alae, and soft triangles.4 For example, the alar groove separates the ala and nasal sidewall. Around the mouth, the vermilion cutaneous junction divides the shiny red vermilion from the hair-bearing skin of the cutaneous lip. The nasolabial fold separates the lip from the cheek. Intentionally placing scars in cosmetic subunit boundaries camouflages them within natural shadows and reflections (Fig. 2.4). Wounds near the boundaries of cosmetic subunits may be expanded to hide scars in the junction lines (Fig. 2.5, Fig. 2.6).

Fig. 2.4 (a) This defect resides along the cosmetic subunit junction lines that separate the cheek from the nose and mouth. (b) Appearance immediately after a linear repair that falls within the nasofacial sulcus and nasolabial fold. (c) Weeks after surgery, the pink scar is less conspicuous because it falls in the cosmetic subunit junction lines where a viewer expects to see lines or shadows.

Fig. 2.5 (a) Tension from a local flap for this nasal tip defect risked distortion of the free margins. (b) The defect was expanded to the boundaries of the nasal tip subunit and repaired with a full-thickness skin graft. (c) The scars along the cosmetic subunit boundaries are inconspicuous and the free margins and contour are restored.

2.1.5 Relaxed Skin Tension Lines
RSTLs correspond to the wrinkles that form with animation of the underlying muscles of facial expression. RSTLs run perpendicular to the direction of the underlying muscle fibers. For example, contraction of the vertically oriented frontalis muscle fibers creates horizontal rhytids on the forehead and contractions of the circumferential orbicularis oculi and orbicularis oris muscles form rhytids that radiate perpendicularly from the free margins of eyelids and lips, respectively (Fig. 2.7). As we age, these lines become more visible even without animation of facial muscles. Scars are less noticeable and have less tension when they align with RSTLs. However, placing scars in RSTLs should not violate higher priority reconstruction principles. For example, if a horizontal closure on the forehead would cause asymmetric lift of the eyebrow, it is better to perform a vertical closure that crosses RSTLs but preserves brow position.

Fig. 2.7 (a, b)Periorbital and perioral lines.
2.1.6 Color and Texture
Mismatches in color and texture can make scars noticeable, a common outcome with skin grafts (Fig. 2.3b, Fig. 2.8). Linear closures and local flaps are preferred, because they recruit adjacent skin of similar color and texture. Mismatches in the density of hair and sebaceous glands can still occur with local flaps (Fig. 2.9), especially if terminal hairs are transposed to areas normally containing vellus hairs. Replacement of specialty skin, such as the vermilion lip or eyelid margin, may not be possible. When it is impossible to avoid color and texture mismatches, conforming to higher priority reconstruction principles (free margins, contour, cosmetic subunit junction lines, RSTLs) often makes these differences acceptable (Fig. 2.9).
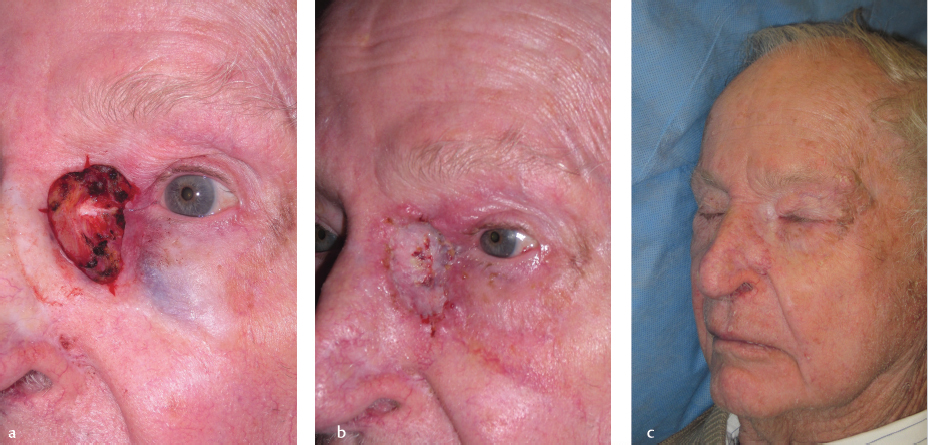
Fig. 2.8 (a) Large defect of the left medial canthus. (b) Healing skin graft. (c) While there is good anatomical position of the eyelids, there is noticeable mismatch in color of the graft in comparison to the surrounding skin.
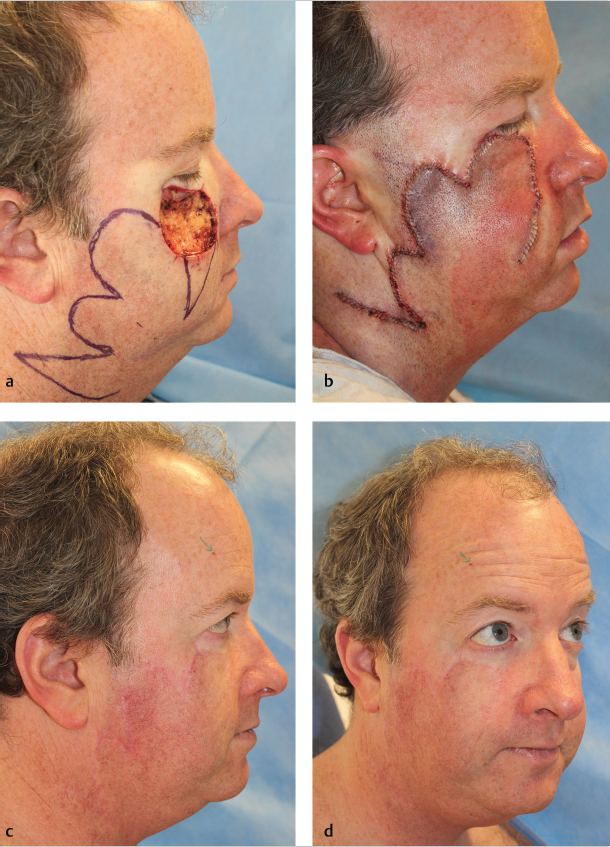
Fig. 2.9 (a) Large Mohs defect on the right infraorbital cheek. (b) Trilobed flap sutured in place. (c,d) Well-healed flap with excellent restoration of contour and no pull on the ipsilateral lower lid. While incision lines are fine, note that the flap is more conspicuous given terminal hair follicles were transposed to an area of normally vellus hair–bearing skin.
2.2 Principles of Tissue Biomechanics
2.2.1 Overview
2.2.2 Preferred Vectors to Move Facial Tissue
The direction in which a skin flap slides toward the defect is called the primary tissue motion, and the countermovement of the surrounding tissue to meet the flap is considered secondary tissue motion. Facial skin moves along preferred vectors (Fig. 2.10).
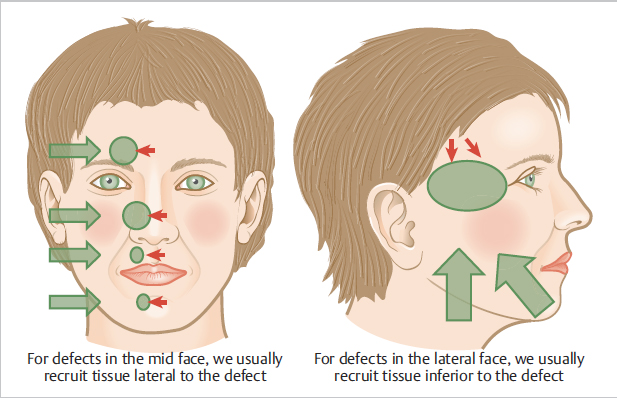
To repair defects of the lateral face (lateral forehead, temples, lateral cheek), the primary tissue motion occurs along a superior or superolateral vector that moves skin from the neck and jowl to more superior locations on the face. The superior vector has minimal impact on the contours of the central face. In general, facial reconstructions are most successful when the primary tissue motion follows these vectors.
2.2.3 How Different Reconstructions Affect Location of Tension Relative to the Primary Defect
Primary closures and sliding flaps (i.e., advancement and rotation) recruit skin immediately adjacent to the wound and maintain greatest tension at the primary defect. When tension at the primary defect is too great for direct closure or if tension will distort anatomy, then transposition (e.g., rhombic, bilobed, and trilobed flaps) and interpolation flaps (e.g., paramedian forehead flap and nasolabial interpolation flap) or grafts may be necessary. These flaps transfer tension to a remote donor site so that tissue can be inset at the primary defect with minimal tension. Whether tension is at the primary defect or a remote donor site, all of these reconstruction options work best when the main tension falls along preferred vectors (lateral to medial in the mid-face and inferior to superior on the lateral face; Fig. 2.10).
2.2.4 Tissue Planes for Undermining and Elevating Flaps
Most local reconstructions of the face require undermining to mobilize tissue. Undermining releases either the skin edges or flap from underlying attachments to gain mobility.
The ideal surgical plane for facial undermining varies based on the location (Table 2.1). If the surgeon is working in an efficient surgical plane, flap elevation and undermining should occur with ease and minimal bleeding. Undue resistance or excessive bleeding while lifting tissue usually signifies an inefficient anatomic plane (e.g., most commonly splitting the subcutaneous fat, rather than working at the junction of the fat and fascia).
Table 2.1 Ideal surgical plane for facial undermining based on location
Anatomic location | Preferred anatomic plane | Comments/critical structures to consider |
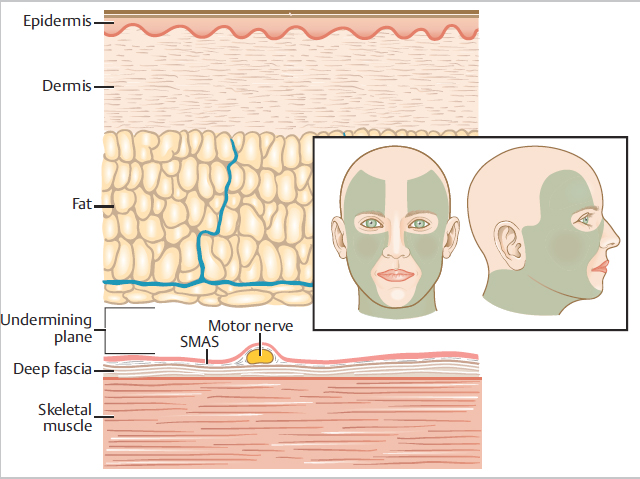
Lateral face and neck | Junction of the subcutaneous fat and superficial musculoaponeurotic system (SMAS) | The motor branches from the facial nerve always lie deep to the most superficial layer of SMAS.a Excision at the junction of the subcutaneous fat and SMAS will always protect the motor nerves. |
Central one-third of the face and scalp | At the junction of subcutaneous fat and SMAS or deep to the muscles of the SMAS (central face) or galea (on scalp) | Because the branches of the facial nerve have arborized before reaching the central one-third of the face, excision deep to the SMAS is less likely to cause motor deficits (e.g., excision of midline and paramedian frontalis muscle does not leave motor deficit on the forehead). On the midline nose, forehead, and scalp, undermining deep to the SMAS is frequently desirable. |
aIn areas where the muscles of facial expression are layered, for example, lip depressors and elevators, the motor nerves innervate the deepest muscles from their superficial surface. Abbreviation: SMAS, superficial musculoaponeurotic system. | ||
On the lateral face, the ideal plane to elevate flaps or undermine tissue is at the junction of the subcutaneous fat and fascia of the superficial musculoaponeurotic system (SMAS) (Fig. 2.11). This plane preserves the branches of the facial nerve, which lie deep to the SMAS. On the central face, excising deep to the muscles of facial expression/SMAS poses minimal risk for motor deficits. The most common surgical plane on the nose and central forehead is deep to the SMAS (Fig. 2.12). For smaller procedures in the central face, the surgeon may choose a surgical plane superficial to the SMAS, such as a small horizontal closure on the forehead or narrow linear closure on the cutaneous lip.