Hidradenitis Suppurativa
Julia M. Kasprzak
David C. Reid
I. BACKGROUND
Hidradenitis suppurativa (HS) is chronic, recurrent, scarring, inflammatory skin condition that involves the apocrine glands of intertriginous areas (Figs. 20-1 and 20-2). It has been estimated to affect 1% to 4% of the population. Most investigators do not report racial differences in incidence of this disease, but it has been established that women are more affected than men (3:1 ratio). The pathogenesis of HS remains unclear; however, follicular plugging, ductal rupture, and secondary inflammation are speculated to play a role. Additionally, genetic, mechanical, and hormonal processes are hypothesized to influence the disease.
II. CLINICAL PRESENTATION
HS has a mean age of onset of 22 years, and the disease course lasts an average of 19 years. Patients present with tender, inflamed nodules, sinus tracts, and abscesses in intertriginous areas. Lesions may drain material that is serosanguinous, purulent, or a mixture of the two, and drainage may be malodorous. Clinical course of HS is variable, with some patients having an intermittent, mild chronic course, and others suffering from persistent, severe disease. Severity of HS is classified by Hurley stages (Table 20-1).
A thorough history and review of systems is important to determine the patient’s genetic predisposition and risk for associated conditions. Approximately one-third of patients report a positive family history of HS, and families with autosomal dominant inheritance have been reported. Synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome, Crohn disease, follicular occlusion tetrad, and pyoderma gangrenosum are all associated with HS (Table 20-2). In addition, there are rare reports of squamous cell carcinoma arising in chronic HS lesions.
HS often causes significant morbidity for patients. They may have difficulty with mobility due to pain, drainage from the lesions may require use of diapers, and the lesions often become intensely malodorous. These factors can cause the patient to become depressed, isolated, or even suicidal. It is important to screen for depression and talk to patients about their quality of life at regular intervals.
III. WORKUP
The diagnosis of HS is usually made on clinical findings alone. However, a short list of differential diagnosis should be considered (Table 20-3). The Second International HS Research Symposium created the following diagnostic criteria (all three criteria must be met):
1. Typical lesions—nodules, abscesses, draining sinus, and bridged scars
2. Location—axillae, groin, genitals, perineal, perianal, buttocks, and infra- and intermammary regions
3. Chronic course and recurrences
Workup for associated diseases should be done on a case-by-case basis.
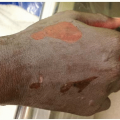
 Figure 20-1. Hidradenitis suppurativa. This patient has involvement of the inguinal areas, labia majora, and medial thighs. (From Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
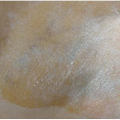
 Figure 20-2. Chronic hidradenitis suppurativa. This patient has involvement of the axilla with bandlike hypertrophic scars. Note the characteristic paired open comedones and the single furuncle-like. (From Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
TABLE 20-1 Hurley Stages | ||||
|---|---|---|---|---|
|