Fig. 7.1
The previous surgical design for mandibular sagittal-splitting ostectomy: Ostectomy is done on the mandibular angle and body area
Authors want to correct misunderstandings related to sagittal resection of the mandible in previous literature. Authors also want to devise a safe and effective sagittal mandibular resection method, for effective mandibular reduction.
Patient Assessment and Consultation
Among the ordinary preoperative evaluation of the patients, the degree of protrusion of the mandible, in frontal view is important. First, amount of masseter muscle hypertrophy, and amount of the subcutaneous fat should be evaluated by the physical examination at initial consultation. Using the PA cephalogram and 3D CT, the degree of protrusion or flaring of the mandible angle is evaluated. Shape and convexity of the body should be examined carefully. A panoramic view does not give a good information in terms of sagittal resection. Imagine the three dimensional shape of sagittal resection in your mind before the surgery.
Indication for sagittal resection of mandible is thick mandibular body especially around oblique line. However, in our institute, sagittal resection of mandible is usually combined with mandible contouring in ordinary mandible reduction patient. There is a group of patients who does not get good effect from sagittal resection, such as patient with thin mandible and scarce bucal fat.
Surgical Techniques
Our mandible reduction surgery was performed with both mandibular contouring and sagittal mandibular resection. The prominent mandible angle’s gonion and lower mandible body were removed by mandibular contouring. Then, the remaining most prominent part of the mandibular area was removed by sagittal mandibular resection by shaving the outer cortex, leaving the inferior alveolar nerve safe. Our sagittal mandibular resection focused on removing the thickest mandible body area (Fig. 7.2).
Fig. 7.2
Author’s design and actual resection. Author’s design for mandibular sagittal resection. Compare the area of resection with conventional description
Sagittal mandibular resection focused on removing the mandible body area. All patients were discharged 1 day after the operation without a suction drain. Most patients who underwent mandibular reduction were satisfied with their aesthetic results. There were no serious complications.
In the axial computed tomography view, there are two types of outer contour of the mandible. In the straight or outcurved type of the mandible (Fig. 7.4), the gonial area protrudes out. In this type of patients, the bigonial distance is the widest area (W2). However, in the incurved type of the mandible (Fig. 7.5), the posterior angle area tilts inwardly, and the most protruded area of the mandible is 1–2 cm anterior to the posterior border of the mandible (P2). Authors name this point as maximal ramus point (MRP) (Figs. 7.5 and 7.6). This area is the widest ramus area, and, in this type of patient, bi-ramus width (W2) is wider than bigonial distance (W3), representing the facial width.
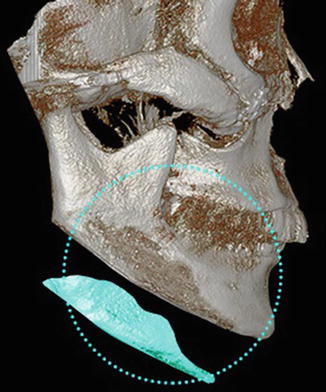
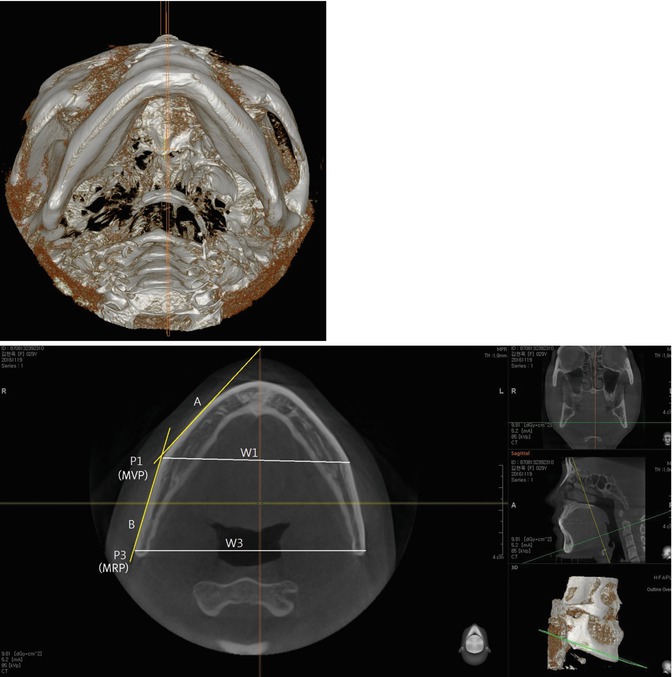
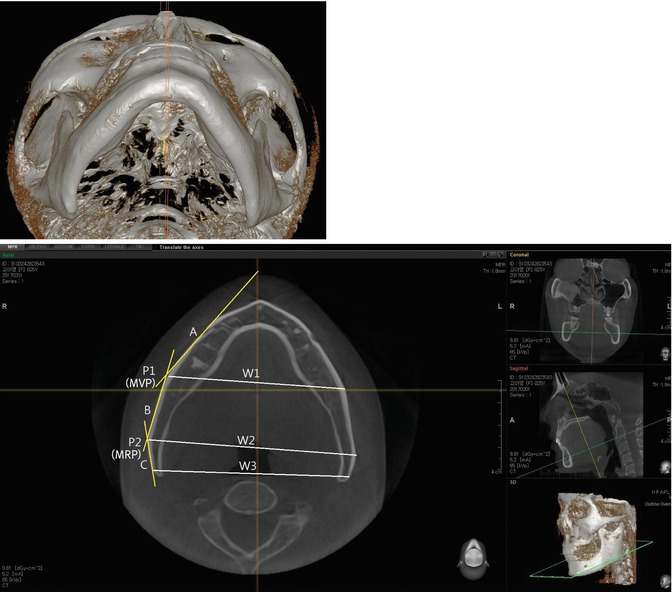
Fig. 7.3
Our surgical outcome for mandibular sagittal resection combined with mandible contouring: the sagittal resection focuses on removing the abundant mandible body area
Fig. 7.4
The mandible of staight or outcurved type. (Upper) Three-dimensional submento-vertex view of the mandible. (Lower) Axial view. The gonial area is the most protruded area, and the bigonial distance is the widest (W3)
Fig. 7.5
The mandible of incurved type. (Upper) Three-dimensional submento-vertex view of the mandible. (Lower) Axial view. The posterior ramus tilts inward. The maximum ramus point is the most protruded area, and the bi-ramus (W2) distance is the widest area comparing bigonial distance (W3)
Regarding the mandibular body when viewed on computed tomography, the widest point is the intersection of the surface line of the mandibular body (A) and ramus (B) (Figs. 7.3, 7.4 and 7.5). This point (P1) is usually the thickest area, the average thickness of which is 17.8 mm, while that at the posterior angle area was 6.4 mm. This point is named as the maximum body point (MBP).
Three lines, two points, and three widths are used to describe the shape of the mandible on computed tomography (Figs. 7.4, 7.5 and 7.6). The line on the mandibular body surface is the body surface line (A), and the one on the ramus surface is the ramus surface line (B). In incurved type of the mandible, there is the third line in the posterior ramus, named as posterior ramus surface line (C). The maximal body point is marked by the widest and usually the thickest point on computed tomography and the intersection of the body surface line and ramus surface line (P1). The maximal ramus point is described as the intersection of the ramus surface line and posterior ramus surface line in the submento-vertex view (P2).
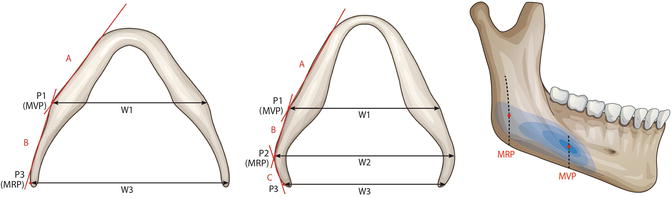
Fig. 7.6
Schematic presentation of the shape of the mandible in axial view. (Left) Straight or outcurved type. (Center) Incurved type. Body surface line (A), ramus surface line (B), and posterior ramus surface line (C) are marked. Compare which part of the mandible represents the facial width: bigonial distance (W3) in straight or outcurved type while bi-ramus distance (W2) in incurved type (Right) MRP and MBP in the actual mandible surface
Two points are important clinically in sagittal resection of the mandible. The maximal ramus point is the widest point in the mandible and should be resected to reduce the width of the face. In incurved type, even after contouring ostectomy, the width of the face does not change at all, resulting in patient’s dissatisfaction. In this case, sagittal resection of the mandible to reduce this maximal ramus point accomplishes a good reduction of facial width, resulting in satisfactory slimming effect. The maximum body point of the mandible is usually the thickest area in the body of the mandible. Maximal resection is possible during the sagittal resection. It is also the widest area in the body of the mandible, and appropriate reduction of this area is critical in shaping the slim and attractive jawline.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


