Rosacea
Eric F. Bernstein
Ryan B. Thorpe
Kevin Schomacker
Jason D. Bloom
Emil A. Tanghetti
Jayant D. Bhawalkar
BACKGROUND
Rosacea is a chronic inflammatory condition comprising facial flushing, telangiectasias, and inflammatory papules and pustules1 estimated to affect 16 million Americans.2 Rosacea is generally distributed on the convexities of the central face and is classified into 4 main subtypes: erythematotelangiectatic rosacea, papulopustular rosacea, phymatous rosacea, and ocular rosacea.3 Although the exact pathomechanisms of rosacea are unknown, substantial recent advances in research support a multifactorial disease process, including roles for a dysregulated immune system, microbial overgrowth, aberrant neurovascular signaling, ultraviolet (UV) radiation exposure, reactive oxygen species, and genetic susceptibility.1,4
The prevalence of rosacea ranges from 1% to 22%,5 likely because of the methods utilized to gather epidemiologic data. For example, using a photograph database of 2,933 women volunteers from 4 international cities (Los Angeles, Akita, Rome, and London), researchers reported prevalence rates of rosacea in 9.6% of all races and 16% in white women,2 whereas retrospective database studies in the United States have reported far lower prevalence rates of 1.34%6 to 2.1%.7 In a recent community-based study aimed to support the notion that the true community prevalence of rosacea is underestimated by database, clinic-based studies, or survey studies, 11% of community members showed signs of rosacea when under direct observation.8 Furthermore,
when specifically using the classification system of the American National Rosacea Society Expert Committee, researchers in Estonia reported a prevalence rate of 22%, again suggesting that rosacea is more common than previously thought.9
when specifically using the classification system of the American National Rosacea Society Expert Committee, researchers in Estonia reported a prevalence rate of 22%, again suggesting that rosacea is more common than previously thought.9
Rosacea is more common in females, except for phymatous rosacea, which is more common in men.10 Communications on the prevalence of ocular rosacea ranges widely from 6% to 58% owing to the potential for high false-positive reports and the need to update the diagnostic criteria for ocular rosacea.5 Since the 1960s, however, ocular involvement has been reported to be in 50% of patients with rosacea.11 The most prevalent form of rosacea is the erythematotelangiectatic subtype. For example, of 168 Korean patients with rosacea, 96.4% were diagnosed with the erythematotelangiectatic subtype, 50.6% had the papulopustular subtype, 14.3% had ocular rosacea, and only 4.8% demonstrated phymatous changes. The mean age at diagnosis in this group of patients was 47.8 years12 Similarly, in a group of patients from Sweden, 81% had erythematotelangiectatic rosacea and 19% had papulopustular rosacea.13 Rosacea is more common in lighter skinned individuals and has not been found in all communities. For example, in a study comparing dermatologic diseases in the United Kingdom with a clinic in Kumasi, Ghana, no cases of rosacea were found in Ghana.14
Several environmental factors are associated with worse disease, including age, lifetime UV radiation exposure, body mass index, smoking, alcohol, cardiovascular comorbidity, and skin cancer comorbidity.15
PRESENTATION
Patients present with a complaint of redness, broken capillaries, poor complexion, or acneiform breakouts. The exacerbations of redness or papules typically occur following sun exposure or wine consumption, but these may occur following any of a number of triggers. In many cases, the patient is unaware of the underlying triggers.
DIAGNOSIS
Clinical Diagnosis
Rosacea is diagnosed by the presence of one or more of the following primary features: flushing (transient erythema), nontransient erythema, papules and pustules, and telangiectasias. Secondary features of rosacea include burning, stinging, erythematous plaques, dry skin, edema, ocular manifestations, or phymatous changes and may occur independently or in combination with the primary features of rosacea.3,16
Histopathology
Rosacea is usually a clinical diagnosis, but occasionally biopsy is needed to differentiate between rosacea and other dermatoses. Histologic examination of erythrotelangiectatic rosacea demonstrates dilated capillaries in the upper dermis and a mild perivascular chronic lymphohistiocytic infiltrate. Biopsy of papulopustular rosacea demonstrates a perifollicular and perivascular mixed infiltrate with lymphocytes, plasma cells, and neutrophils. In phymatous rosacea, marked sebaceous hyperplasia is seen along with dermal hyaluronic acid and fibrotic stroma.1
Subtypes
In 2002 the National Rosacea Society Expert Committee detailed the clinical presentations of each rosacea subtype, and in 2004, a grading system was released to improve patient outcomes, communication among physicians, and the efficacy of research.3,17
Erythematotelangiectatic Rosacea
Erythematotelangiectatic rosacea is characterized by facial flushing often with persistent central facial erythema. Although not required for diagnosis, telangiectasias, central facial edema, stinging or burning sensations, and roughness or scaling are frequently seen.3 This subtype may occasionally mimic facial contact dermatitis, photosensitivity, or the “butterfly rash” of lupus erythematosus.16 Prolonged episodes of flushing with sweating, flushing not limited to the face, and flushing accompanied with systemic symptoms such as diarrhea, wheezing, headaches, palpitations, or weakness demand further investigation to rule out other causes of flushing (eg, mastocytosis, pheochromocytoma, or carcinoid syndrome).16
Papulopustular Rosacea
Papulopustular rosacea presents with transient papules or pustules in addition to the persistent central facial erythema seen in erythematotelangiectatic rosacea. The papules and pustules of this subtype of rosacea
may resemble acne vulgaris, except that comedones are absent. Stinging and burning sensations are also frequently reported, and the papules and pustules may occur periorificially (perioral, perinasal, or periocular).3 A recent cross-sectional study of 135 patients concluded that only a small portion of patients progress from one subtype to another. Of patients with erythematotelangiectatic rosacea, in spite of a mean duration of rosacea of 21 years, 69% never fulfilled the criteria for papulopustular rosacea; however, of those who did have papulopustular rosacea, 66% developed erythematotelangiectatic rosacea before papulopustular rosacea.18
may resemble acne vulgaris, except that comedones are absent. Stinging and burning sensations are also frequently reported, and the papules and pustules may occur periorificially (perioral, perinasal, or periocular).3 A recent cross-sectional study of 135 patients concluded that only a small portion of patients progress from one subtype to another. Of patients with erythematotelangiectatic rosacea, in spite of a mean duration of rosacea of 21 years, 69% never fulfilled the criteria for papulopustular rosacea; however, of those who did have papulopustular rosacea, 66% developed erythematotelangiectatic rosacea before papulopustular rosacea.18
Phymatous Rosacea
Phymatous rosacea is characterized by bulbous thickening of the skin with irregular surface nodularity and facial enlargement. Chronic edema in addition to connective tissue and sebaceous gland hypertrophy is also present.19 This subtype may be seen after, or in combination with, either of the aforementioned rosacea subtypes.3 Epidemiological researchers report that, although 80% of patients with erythematotelangiectatic rosacea never meet criteria for phymatous rosacea, of the 20% who did have phymatous rosacea, only 8% developed phymatous rosacea without first having erythematotelangiectatic rosacea.18 Phymatous rosacea can affect multiple areas of the face, including the nose (rhinophyma), chin (gnathophyma), forehead (metophyma), cheeks, eyelids (blepharophyma), or ears (otophyma).19 Unlike all other forms of rosacea, phymatous rosacea is much more common in men, reportedly up to 20 times more common, than in women.20 Although phymatous rosacea is frequently referred to as “end-stage rosacea,” it can happen independently of any other features of rosacea.16
Ocular Rosacea
Ocular rosacea, seen in 35% to 50% of patients,10,18 is defined by the National Rosacea Society as eyes having one or more of the following signs and symptoms: foreign body sensation, burning or stinging sensations, watery or bloodshot appearance, dryness, itching, light sensitivity, blurred vision, telangiectasias of the conjunctiva and lid margin, or lid and periocular erythema.3 Chalazions and hordeola are common signs of rosacea-related ocular disease, and blepharitis, conjunctivitis, and irregularity of the eyelid margin have all been reported findings.3 Corneal complications, such as punctate keratitis, corneal infiltrates or ulcers, or marginal keratitis can each result in decreased visual acuity.3 Ocular rosacea may precede, follow, or occur independently of skin changes.16
Periorificial/Perioral Dermatitis
Often considered a variant of rosacea, perioral dermatitis presents with minute papulopustules in the perioral, perinasal, and periorbital regions, often accompanied by erythema and telangiectasia.
Differential Diagnosis
Autoimmune photosensitivity disorders (lupus erythematosus, dermatomyositis, etc.)
Flushing syndromes (carcinoid, pheochromocytoma, etc.)
Photodermatitis (polymorphous light eruption, photoallergic contact dermatitis)
Seborrheic dermatitis
Acne vulgaris
Actinic dermatitis
Photoaging
Contact dermatitis
Demodex folliculitis
PATHOGENESIS
Although the pathogenesis remains to be fully elucidated, leading proposed mechanisms include dysregulation of the innate immune system, vascular changes, reactive oxygen species, UV radiation, and microbial overgrowth.4 It is the interplay between these factors that likely underpins the clinical manifestations of rosacea.
Immune System Dysregulation
Several elements of the innate immune system are abnormally regulated in rosacea. Yamasaki et al. discovered that cathelicidin (LL-37), an antimicrobial peptide of the innate immune system,21,22 is both abnormally increased and in an abnormal form in rosacea skin. Also increased is kallikrein 5, the primary serine protease responsible for processing cathelicidin into active form. Investigators have shown that increased cathelicidin and serine protease activity result in increased skin inflammation in mice.4 Cathelicidin is also associated with other characteristic features of rosacea such as vasodilation and vascular proliferation.23 Cathelicidin is
induced by vitamin D, which is known to be activated by UV light, an established agitator of the disease.1 Toll-like receptor 2 (TLR2), a microbial pattern recognition receptor is also induced by vitamin D; blocking the TLR2 receptor inhibits cathelicidin production.24 Mast cells, immune cells of granulocytic heritage, are also found in increased numbers in the dermis of rosacea and happen to be one of the primary sources of cathelicidin. In one study, mice depleted of their mast cell stores did not develop rosacea-like features when injected with cathelicidin, whereas wild-type mice preloaded with mast cell stabilizers displayed increased levels of rosacea-like features as well as high amounts of chymase, tryptase, and matrix metalloproteinase-9 when injected with cathelicidin.22 Scientific explorations regarding the dysregulated immune system demonstrated in rosacea are ongoing.
induced by vitamin D, which is known to be activated by UV light, an established agitator of the disease.1 Toll-like receptor 2 (TLR2), a microbial pattern recognition receptor is also induced by vitamin D; blocking the TLR2 receptor inhibits cathelicidin production.24 Mast cells, immune cells of granulocytic heritage, are also found in increased numbers in the dermis of rosacea and happen to be one of the primary sources of cathelicidin. In one study, mice depleted of their mast cell stores did not develop rosacea-like features when injected with cathelicidin, whereas wild-type mice preloaded with mast cell stabilizers displayed increased levels of rosacea-like features as well as high amounts of chymase, tryptase, and matrix metalloproteinase-9 when injected with cathelicidin.22 Scientific explorations regarding the dysregulated immune system demonstrated in rosacea are ongoing.
Vascular Changes
Increased vascularity has historically been thought to play a role not only in developing rosacea but also in many of the symptoms of rosacea. Supporting this supposition is the successful treatment of rosacea with the topical selective alpha-1 adrenergic receptor agonist, oxymetazoline.25 Moreover, lesional skin is marked by increased VEGF, CD31, and D2-40 compared with non-lesional skin, further advancing increased vascularity as a contributing factor to rosacea.26 In addition, increased skin blood flow has been demonstrated in papulopustular rosacea skin but not in erythematotelangiectatic rosacea.27 Undoubtedly, laser therapy is uniquely positioned to target vascular contributions to the pathogenesis of rosacea.
Ultraviolet Radiation and Reactive Oxygen Species
UV exposure contributes to rosacea in a variety of mechanisms. Specifically, UV radiation increases reactive oxygen species in the skin,1 and UVB radiation and hydrogen peroxide are potent inducers of vascular endothelial growth factor28 and are known to amplify the kallikrein 5/cathelicidin cascade through TLR2 signaling.1 With regard to rosacea, reactive oxygen species are reported to alter matrix metalloproteinases, enhance inflammatory reactions, and degenerate cutaneous collagens. In fact, many treatments of rosacea may work by decreasing reactive oxygen species.21
Genetic Contributions
Although no specific gene or set of genes has been identified as causing rosacea, the suspected genetic component was supported by a 2015 study of 275 twin pairs. Employing the National Rosacea Society grading system17 and the well-accepted ACE statistical model, the genetic contribution to rosacea pathogenesis was calculated to be 46%.15 With time, genetic susceptibility genes will only become more defined and may relate to the immune system.
Microbial Overgrowth
Although this theory is not universally accepted, overgrowth of various microbes accused in the pathogenesis of rosacea may work in combination with the factors described above to result in rosacea. Supporting this theory, investigators have shown that the density of Demodex mites in the skin of patients with rosacea is higher than in normal controls (10.8 mites/cm2 vs 0.7 mites/cm2, respectively).29 It is important to note, however, that Demodex mites are normal colonizers of human skin, as the main food sources for these mites in all phases of development are epidermal cells and sebum components. This explains why the mites are found on areas of skin particularly rich in sebaceous glands, such as the nose, cheeks, forehead, and chin.30 Reports of normal rates of colonization of Demodex folliculorum and Demodex brevis, the 2 main species of mites on human skin, range from 20% to 80% in people unaffected by rosacea, with increased colonization rates as people age.
Facial itching in the absence of erythema is correlated with mite density, and antigens from bacteria found within Demodex can stimulate lymphocyte proliferation.31 Accordingly, some suggest that the pathogenesis of rosacea is due more to the bacteria living within the mite than the mite itself. For example, Bacillus oleronius, a bacteria found in Demodex in a symbiotic relationship, produces proteins more capable of stimulating blood mononuclear cell proliferation in patients with rosacea (16 of 22) than in control patients (5 of 17).32 Other investigators suggest that the mites may play a more active role by mechanically blocking hair follicles, secreting digestive enzymes, and/or triggering reactions of the immune system.30 Antibiotics used to treat rosacea may in part be effective because of activity against the bacteria. This is suggested by data showing that antibiotics useful in some patients, such as tetracyclines, do not have any activity against Demodex but are lethal to
the B oleronius. Chitin from Demodex, however, has been postulated to increase TLR2 expression. In fact, chitin-induced effects were largely not seen in one study in which TLR2 receptors were blocked.33
the B oleronius. Chitin from Demodex, however, has been postulated to increase TLR2 expression. In fact, chitin-induced effects were largely not seen in one study in which TLR2 receptors were blocked.33
Demodex mites and B oleronius are not the only microbes implicated in rosacea. Staphylococcus epidermidis has also garnered some attention ever since researchers reported that pustules in papulopustular rosacea grew pure S epidermidis, whereas control cultures from unaffected areas on the same faces did not.34 Others have shown that the S epidermidis isolated from patients with rosacea exhibited different protein excretions at different amounts at different temperatures compared with controls. In addition, S. epidermidis from patients with rosacea is consistently beta-hemolytic compared with the nonhemolytic strains found on control subjects.35 Similar to the suggested mechanisms of the other microbes discussed earlier, S epidermidis also secretes molecules that increase defensins through TLR2 signaling.36
As can be derived from the earlier discussion, the pathogenesis of rosacea is complex and unsolved, but most agree that recent research indicates that the innate immune system, UV radiation, vascular changes, genetics, and microbial overgrowth may all play a role in the pathogenesis of rosacea and that it is the collaboration among these systems that results in the signs and symptoms of rosacea.
TREATMENT OF ROSACEA
The 4 phenotypic expressions of rosacea may be the result of distinctive pathogenic factors and, subsequently, respond to equally distinctive therapeutic methods.37 Algorithm 9.2.1 outlines treatment for the various subtypes of rosacea.
Medical
Avoid Triggers
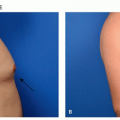
The main symptoms of rosacea, flushing and blushing, result from the accumulation of extra blood vessels that occur following chronic sun exposure, superimposed upon a genetic predisposition to develop telangiectasias from the sun.13,14,15,38,39 Rosacea can affect from 2.7%38 to 10%14 of individuals depending on the population being studied, sampling ability, and criteria for diagnosing rosacea, and as stated earlier those percentages can vary widely. A brilliant twin study conducted at a convention of twins in the northeast United States determined that a genetic predisposition to develop rosacea accounted for approximately half of the likelihood to develop rosacea, whereas greater sun exposure accounted for the other half.15 Other factors, such as surgery in an affected area, or smoking, which causes free-radical stress in a fashion similar to sun exposure, can also contribute to the development of unwanted blood vessels. In addition, esthetic treatments such as hyaluronic acid fillers also cause telangiectasias in treatment areas, owing to stimulation of extracellular matrix production, including unwanted blood vessels. Topical treatments, such as tretinoin can also induce telangiectasias, perhaps by stimulation of extracellular matrix or by increasing sensitivity to the sun. However, as is immediately obvious when looking at the distribution of erythema in sun-exposed facial skin, the sun is by far the biggest culprit in the development of linear telangiectasias and diffuse erythema that characterize rosacea (Figure 9.2.1). The typical areas of involvement are the cheeks, chin, nose, and central forehead, with sparing of areas shaded by the brow, chin, or hair.
Sun Protection
Sunscreen. Regardless of the subtype, daily broadspectrum sunscreen use and sun avoidance behaviors are essential to rosacea management.37 The 4 big touch points for every patient presenting for laser treatment of rosacea should be: (1) sunscreen applied to all exposed sites (face, neck, chest, and hands) daily, rain or shine; (2) UV-blocking window film for every patient’s car; and (3) hats to shield the forehead and obviate the need for sunscreen on the forehead, which can sweat into the eyes hurting compliance; and (4) brown sunglasses to block the shorter visible wavelength protecting the eye and the periocular skin. The advice most often ignored is the need to apply UV-blocking window film to the patients’ cars, presumably because of the perception that little UV reaches within a car, the perception that being hot correlates with UV exposure, as well as the cost and inconvenience of having the film applied. The fact that many people have significant asymmetry of their facial veins, with the left or right side predominating, tells us that UV exposure through window glass is clinically significant and that we spend far too much of our time “outside” actually in the car (Figure 9.2.1). It is critical to have a list of businesses
that apply window film in the area of one’s patientreferral geographic area and a knowledge of the state-by-state laws governing window film application in one’s area and to emphasize that UV-blocking window films is clear, thus enabling equal or even better night vision due to cutting glare. Auto glass typically transmits from 71% to 79% of UV radiation, predominantly blocking in the UVB portion of the solar spectrum.40 Although UVA typically is less damaging to our skin, chronic UVA exposure results in significant photodamage, as evidenced by the predominance of photodamage on the side of the face and arm on which drivers or passengers typically sit.41 This
is best illustrated when comparing countries where the driver and passengers sit on opposite sides of the car.41 UV-blocking window film can reduce transmission of UV by 99.6% or more, while reducing the biological effect of solar-simulating radiation by 93%.40 Experience teaches that patients not following this advice often return for a single laser treatment on the driver’s side, if they are the primary driver, or the passenger’s side if they are primarily the passenger.
that apply window film in the area of one’s patientreferral geographic area and a knowledge of the state-by-state laws governing window film application in one’s area and to emphasize that UV-blocking window films is clear, thus enabling equal or even better night vision due to cutting glare. Auto glass typically transmits from 71% to 79% of UV radiation, predominantly blocking in the UVB portion of the solar spectrum.40 Although UVA typically is less damaging to our skin, chronic UVA exposure results in significant photodamage, as evidenced by the predominance of photodamage on the side of the face and arm on which drivers or passengers typically sit.41 This
is best illustrated when comparing countries where the driver and passengers sit on opposite sides of the car.41 UV-blocking window film can reduce transmission of UV by 99.6% or more, while reducing the biological effect of solar-simulating radiation by 93%.40 Experience teaches that patients not following this advice often return for a single laser treatment on the driver’s side, if they are the primary driver, or the passenger’s side if they are primarily the passenger.
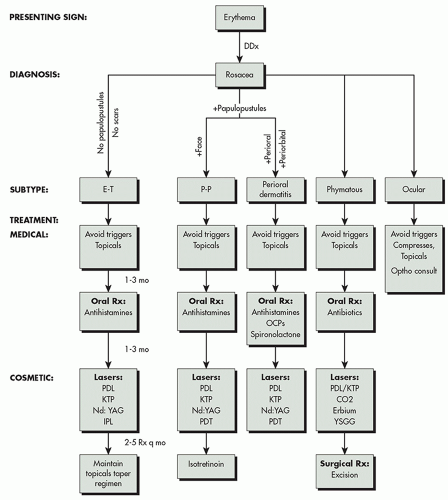 ALGORITHM 9.2.1 Treatment for the various subtypes of rosacea. CO2, carbon dioxide; E-T, erythematotelangiectatic; KTP, potassium titanyl phosphate; Nd:YAG, neodymium-doped yttrium aluminum garnet; PDL, pulsed dye laser; P-P, papulopustular; YSGG, yttrium, scandium, gallium, and garnet. (Courtesy of Macrene Alexiades, MD, PhD.) |
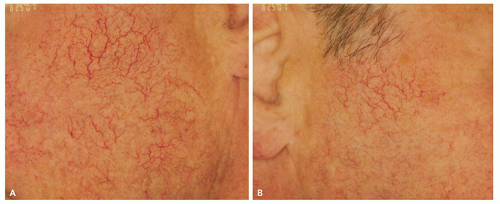 FIGURE 9.2.1 The driver’s side (A) and passenger’s side (B) of a patient who states he is the driver almost all the time he is in a car, showing many more telangiectasias on the driver’s side, thus illustrating the influence of sun exposure while in the car to the development of rosacea. (Reprinted with permission from Main Line Center for Laser Surgery.) |
Topical Therapy
Topical medications approved by the Food and Drug Administration for treating rosacea include metronidazole, sodium sulfacetamide and sulfur, azelaic acid, and ivermectin.37,42 Steroid-induced rosacea has responded to tacrolimus 0.075% ointment when combined with 595-nm laser therapy43 or avoiding other known aggravators, such as caffeine, spicy foods, alcohol, and hot fluids.44 With regard to the effectiveness of topical ivermectin, a recent phase III, investigator-blinded, randomized, parallel-group study found ivermectin 1% cream superior to metronidazole 0.75% cream with the percentage reduction of inflammatory lesions being 83% and 73.7%, respectively.45 In refractory oculocutaneous rosacea with proven Demodex folliculorum colonization, a single dose of oral ivermectin resulted in resolution.46 In another patient with refractory papulopustular rosacea the condition improved with oral ivermectin and topical permethrin 5% cream.47 Topical brimonidine, an α-2 adrenergic agonist, was more effective than vehicle at reducing the redness in patients with rosacea presumably by targeting blood vessels, and cyclosporine may be effective for ocular rosacea. Topical dapsone and other topical antibiotics, including clindamycin and erythromycin, are effective.
Oral Therapy
Older studies have long supported the use of oral tetracyclines, particularly doxycycline, for treating rosacea, and at least for some patients, azithromycin has been shown to be equivalent.48 Isotretinoin can be used in severe, recalcitrant cases.
Ocular rosacea can be treated with topical drops, eyelid hygiene, or metronidazole gel to the lid margins,16 as well as oral antibiotics such as the tetracyclines.
Cosmetic
Laser Therapy
Overview. Despite exhaustive topical and oral phar-macotherapy, for many patients the persistent visible vessels and erythema in rosacea are a major cosmetic concern and contribute to relapses.49 Laser therapy to treat rosacea targets blood vessels underlying the erythema of rosacea and also remodels and reorganizes dermal connective tissue and enhances the epidermal barrier.37 A diverse array of mechanisms has been suggested, including the stimulation of fibroblasts and
endothelial cells leading to cytokine, growth factor, and heat shock protein activation.37
endothelial cells leading to cytokine, growth factor, and heat shock protein activation.37
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


