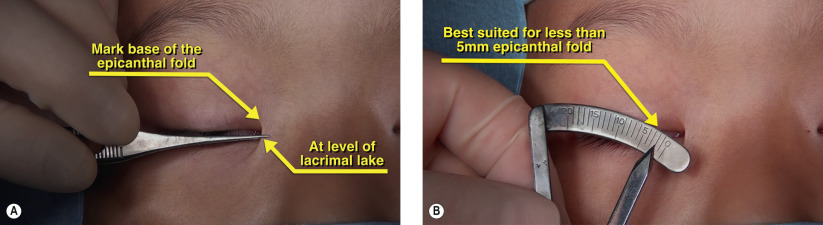
| Cosmetically displeasing epicanthal fold less than 5 mm |
| In combination with ptosis surgery, double upper eyelid crease formation or epiblepharon repair |
| Desire for concurrent double eyelid surgery |
| History of prior hypertrophic scarring of skin or keloid formation after incisional surgery |
| Type of epicanthal fold present |
| No excess upper eyelid dermatochalasis or eyelid ptosis present |
| Discussion of complications related to scar formation and visibility of incision lines |
Introduction
The presence of an epicanthal fold with the absence of a supratarsal fold (double upper eyelid) is a common finding in the Asian patient. In patients without a prominent epicanthal fold, creation of a double eyelid ( Chapters 4 and 5 ) can create an aesthetically pleasing outcome. However, if a prominent epicanthal fold is not concurrently addressed during double eyelid surgery, the resulting outcome may appear suboptimal due to the apparent shortening of the horizontal palpebral fissure and widened intercanthal distance.
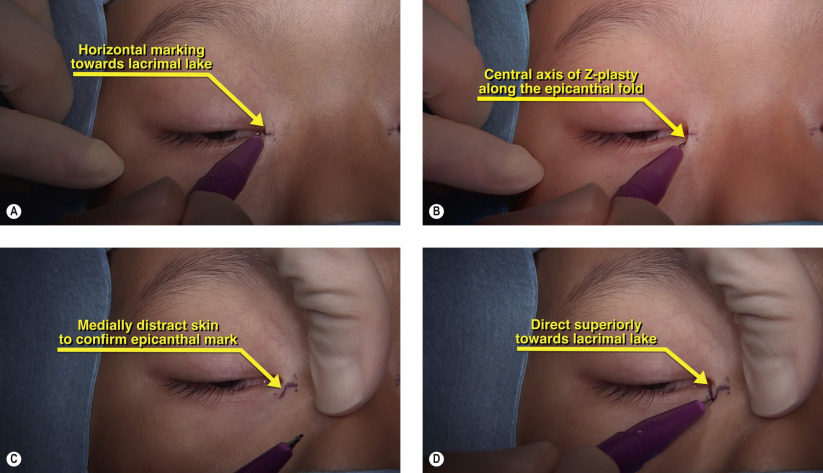
The classic technique to address epicanthal folds is Mustardé’s technique, as covered in Chapter 8 . Mustardé’s epicanthoplasty involves larger incisions and can more powerfully reduce congenitally anomalous epicanthal folds but may cause more visible scarring in the medial canthal region. The root Z-epicanthoplasty, has the benefit of smaller incisions, which are created with minimal wound tension and can be an excellent cosmetic adjunct during double eyelid surgery. The root Z-epicanthoplasty differs from the classic Z-plasty flap in that the angles of the Z are not equivalent. To allow for rearrangement of these flaps, judicious undermining is performed with conservative debulking of the subcutaneous fibrofatty tissues and orbicularis muscle fibers which constitute the epicanthal fold.
Surgical Technique