11 Role of Dermatopathology in the Surgical Management of Skin Cancer The role of dermatopathology in the surgical management of cutaneous malignancy mirrors the role of pathology in the management of most cancers. The goal is to establish an accurate diagnosis, provide prognostic information, and determine the surgical margin status. Dermatopathology is somewhat unique in that many tumors are caught at very early stages; thus, these patients are typically expected to do well compared to patients with tumors occurring at visceral sites. Also unique is the variety of benign and malignant cutaneous neoplasms with a broad spectrum of histopathologic features and clinical behaviors. For example, there is no other type of benign human tumor which displays as great a spectrum in features as melanocytic nevi. Additionally, there is no other benign tumor, which can be as difficult to distinguish from its malignant counterpart as an atypical nevus from melanoma. This chapter is intended to highlight the particularities found in the most common types of cutaneous malignancies as they relate to the vital diagnostic, prognostic, and predictive information contained within the pathology report. The need for improved completeness in cancer pathology reporting to improve patient care has been recently recognized. In response to this need, pathology organizations have published recommended reporting protocols for various tumor types. Much of what is included in the pathology cancer reports generated in the United States is guided by the College of American Pathologists (CAP)-produced cancer Protocols, which reflect current updates to the American Joint Committee on Cancer (AJCC) Cancer Staging Manual and the most recent WHO tumor classification systems.1 The CAP cancer protocols serve as a resource for pathologists to aid in effective reporting of surgical pathology findings necessary to provide quality patient care, and can additionally include optional cancer biomarker reporting templates. Biomarker reporting templates establish reporting guidance for commonly ordered biomarkers (e.g., estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 in breast cancer) and improve consistency and completeness of results reporting. Currently, there are no such biomarker reporting templates for primary cutaneous neoplasms, yet this may change in the coming years. The American College of Surgeons Commission on Cancer (ACS CoC) has recognized the value of such protocols, and it has been mandated that pathologists at CoC-approved cancer programs include the scientifically validated or regularly used data elements of the protocols in their surgical pathology reports on cancer specimens, as of January 1, 2004. Basal cell carcinoma (BCC) derives its name from its resemblance to the basal layer keratinocytes of the epidermis. It is thought to originate from the lowest layers of the epidermis or the outer root sheath of the pilosebaceous unit. This carcinoma shares many features with follicular matrix epithelium, including their immunophenotypic-staining pattern. BCC is the most common cancer in humans,2 and yet the CAP does not include specific cancer reporting protocols for BCC, due to its overall excellent prognosis. That said, appropriate management is necessary to avoid local tissue destruction and tissue disfigurement while preserving cosmesis and function. To this aim, pathologic parameters in the biopsy specimen can help determine the potential for subclinical extension beyond a clinically defined border, and thus are commented on. The pathologic risk factors which define high-risk versus low-risk primary BCC relate to tumor size, depth of invasion, histologic tumor subtype, perineural invasion, and vascular invasion (very rarely seen, but unfavorable if present). Studies have shown that the gross size of tumor impacts the risk for depth of invasion, subclinical extension, and recurrence-free survival, with ≥ 2 cm appearing to confer increased risk to trunk and extremity lesions; ≥ 6 mm for face, genitalia, hands/feet; and ≥ 10 mm for all other anatomic locations.3 The histologic tumor subtype of BCC is a predictor of risk of recurrence and metastasis. Indeed, studies list the strongest predictors for recurrence to be aggressive histologic tumor type, along with positive excision margins.4 While there are many types of BCC recognized, most can be grouped as nonaggressive, aggressive, or indifferent ( Fig. 11.1 (a) BCC, nodular. (b) BCC, superficial, multifocal. The vast majority of BCCs do not require immunohistochemical (IHC) staining for diagnosis. In rare BCCs, such as the so-called trichoepitheliomatous types ( BCC is typically thought to be a continuously growing tumor; yet, reports of “skip” lesions still exist, especially with regard to superficial BCC. For the purposes of surgical and pathologic margins, however, BCCs can be considered a continuously growing tumor. Current practice guidelines from the National Comprehensive Cancer Network suggest a 4-mm lateral clinical margin for BCCs ≤ 2 cm diameter treated with elliptical excision, based on studies which showed a 98% histologic cure rate in this setting.10 This may not always be desirable given the cosmetically and functionally sensitive location. As such, Mohs’ micrographic surgery or surgical excision with complete, circumferential, peripheral, and deep margin assessment (CCPDMA) or “slow Mohs” is often undertaken.11 Some studies suggest that traditional paraffin-fixed serial cross-sectioning (bread loafing) techniques can miss positive surgical margins in up to 56% of cases.12 In addition, although the pathology report will include the positivity or negativity of the surgical margins, the distance of the margin to tumor may or may not be reported. Margins can only be partially examined in shave “saucerization” and punch biopsy specimens, and thus are typically not discussed. In rare circumstances in which surgical treatment is not feasible for BCC, systemic therapy has become available. Options include vismodegib (BMS-833923), saridegib (IPI-926), and sonidegib/erismodegib (LDE225), which target the activating mutations in the hedgehog signaling pathway that are known to drive BCCs.13 Cutaneous squamous cell carcinoma (cSCC) is the second most common skin cancer, and is formed from the keratinizing cells of the epidermis. SCC is typically classified as high risk or low risk depending on the risk for local recurrence and metastasis. The tumor size and anatomic location criteria for risk stratification are identical to those used for BCC. CAP requires reporting of invasive squamous cell carcinomas greater than 2 cm in greatest dimension (which are automatically a minimum of pT2 pathologic tumor stage) to be performed in a templated manner,1 due to the doubled risk for local recurrence and tripled risk for metastasis in this setting.14 The templated pathologic report should contain all histopathologic parameters associated with a worse prognosis, defined as high-risk features by the AJCC-7 staging criteria. These include tumor size and site (greatest dimension: > 2 cm; ear or non–hair-bearing lip), histologic grade (poor or undifferentiated), maximum tumor thickness (> 2 mm), anatomic level (Clark IV or V), and perineural or vascular involvement (present).14,15 The caliber and location of the involved nerve is prognostically relevant. Local recurrence is more likely if the involved nerve is located in the subcutis or muscle and when the caliber exceeds 0.2 mm. Fig. 11.2 (a) BCC, micronodular. (b) BCC, infiltrative (low power). (c) BCC, infiltrative (high power). (d) BCC, morpheaform. (e) BCC, trichoepitheliomatous (alternative). While various subtypes of squamous cell carcinoma are recognized, including acantholytic ( Maximum tumor thickness (Breslow’s thickness) is measured with a calibrated ocular micrometer, which is a glass disk that fits in the microscope eyepiece. It has a ruled scale used to measure the size of magnified objects. The physical length of the marks on the scale varies depending on the degree of magnification. Breslow’s tumor thickness is measured from the granular layer of the epidermis, or the base of the ulcer in ulcerated lesions, to the deepest extent of tumor. Increasing Breslow’s thickness is associated with increased risk, as is increasing Clark’s level of invasion ( Often, tumors with high-risk features are treated with Mohs micrographic surgery or resection with CCPDMA. Tumors with perineural invasion especially benefit from intraoperative margin control and possibly adjuvant radiation therapy. The size of the involved nerve should be included in the pathology report, as diameter 0.1-mm or greater increases risk of recurrence and metastasis.16 Fig. 11.6 (a) Cutaneous squamous cell carcinoma (cSCC), sarcomatoid, spindle cell (H&E low power). (b) cSCC, sarcomatoid, epithelioid (high power). Incomplete removal of primary cSCC makes subsequent therapies much less likely to succeed.17 If a lesion is removed by elliptical excision, the surgical specimen should be oriented and bread-loafed sections submitted at 2- to 3-mm intervals with marginal involvement reported. The best clear indicator of a positive margin is tumor with either ink or cautery artifact on it ( Sentinel lymph node biopsy (SLNBx) is considered in patients with high-risk cSCC and clinically negative lymph nodes because approximately 12% of these nodes will be positive.18,19 Sentinel and regional lymph node detection of cSCC is usually possible using hematoxylin and eosin (H&E) stains alone, due to the significantly different morphology of this carcinoma compared to normal lymph node constituents ( Although malignant melanoma (MM) is much less common than BCC and cSCC, no other diagnosis lends itself to as much difficulty, subjectivity, and lack of agreement among dermatopathologists.22,23,24,25,26 This may be due to the large degree of histologic overlap of melanoma with various benign mimickers, and due to the limited spectrum of cytologic atypia in melanomas compared to other malignancies. For instance, superficial spreading (
11.1 Introduction
11.2 Basal Cell Carcinoma
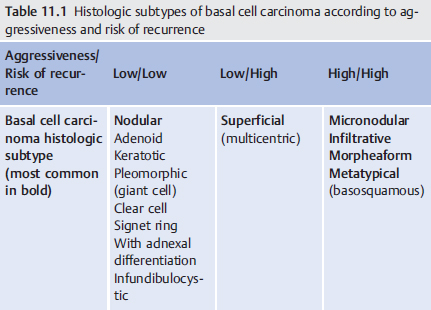
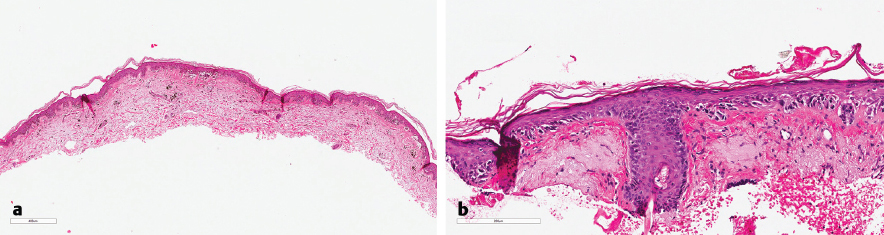
![]() Table 11.1), and often there are mixed types within one tumor. Nodular (
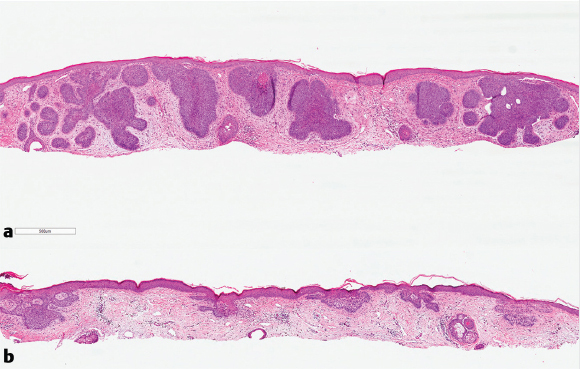
Table 11.1), and often there are mixed types within one tumor. Nodular (![]() Fig. 11.1a) and superficial (
Fig. 11.1a) and superficial (![]() Fig. 11.1b) BCCs are common forms falling into the nonaggressive category. Nodular BCC grows in large dermal tumor nodules, often with connection to the overlying epidermis. Within these nodules, cells can form into trabeculae or pseudoglandular spaces. The perimeter of tumor nodules shows nuclear palisading and often retraction artifact from the surrounding myxoid stroma by a cleft-like space. Superficial BCCs are multifocal in nature and hang off the epidermis. For this reason, they show a higher rate of local recurrence compared to nodular subtype alone. Infundibulocystic BCC is the most indolent variant of BCC, and some argue it may not be a real carcinoma, thus referring to it as “basaloid follicular hamartoma.” Micronodular (
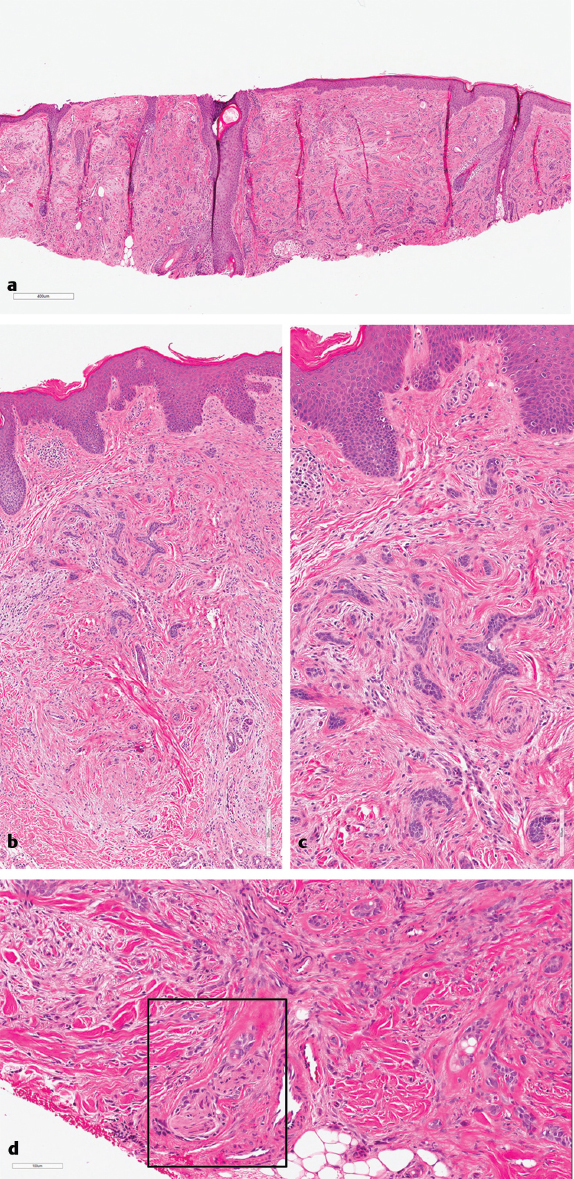
Fig. 11.1b) BCCs are common forms falling into the nonaggressive category. Nodular BCC grows in large dermal tumor nodules, often with connection to the overlying epidermis. Within these nodules, cells can form into trabeculae or pseudoglandular spaces. The perimeter of tumor nodules shows nuclear palisading and often retraction artifact from the surrounding myxoid stroma by a cleft-like space. Superficial BCCs are multifocal in nature and hang off the epidermis. For this reason, they show a higher rate of local recurrence compared to nodular subtype alone. Infundibulocystic BCC is the most indolent variant of BCC, and some argue it may not be a real carcinoma, thus referring to it as “basaloid follicular hamartoma.” Micronodular (![]() Fig. 11.2a), infiltrative (
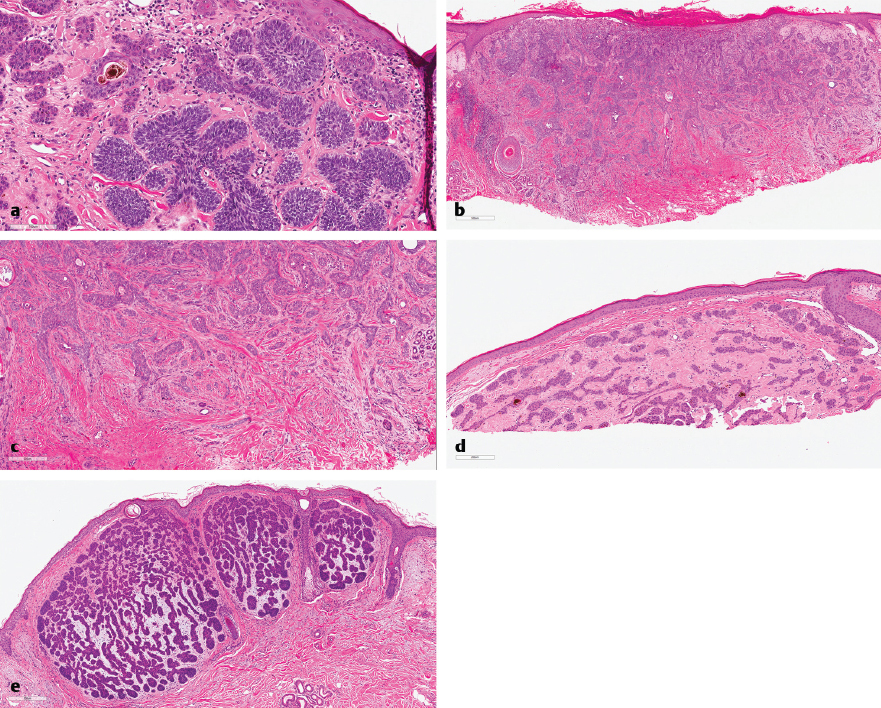
Fig. 11.2a), infiltrative (![]() Fig. 11.2b, c), and morpheaform (
Fig. 11.2b, c), and morpheaform (![]() Fig. 11.2d) subtypes of BCC are associated with a higher incidence of positive margins and thus tumor recurrence.5,6 For this reason, BCC subtyping is important information to be included in the pathology report. The micronodular pattern shows small tumor nodules (< 0.15 mm) and lacks circumscription. Micronodular BCC (
Fig. 11.2d) subtypes of BCC are associated with a higher incidence of positive margins and thus tumor recurrence.5,6 For this reason, BCC subtyping is important information to be included in the pathology report. The micronodular pattern shows small tumor nodules (< 0.15 mm) and lacks circumscription. Micronodular BCC (![]() Fig. 11.2e) usually shows at least focal retraction artifact, stromal mucin, increased mitosis, and a lack of papillary mesenchymal bodies, as distinguishing factors from trichoepitheliomas (
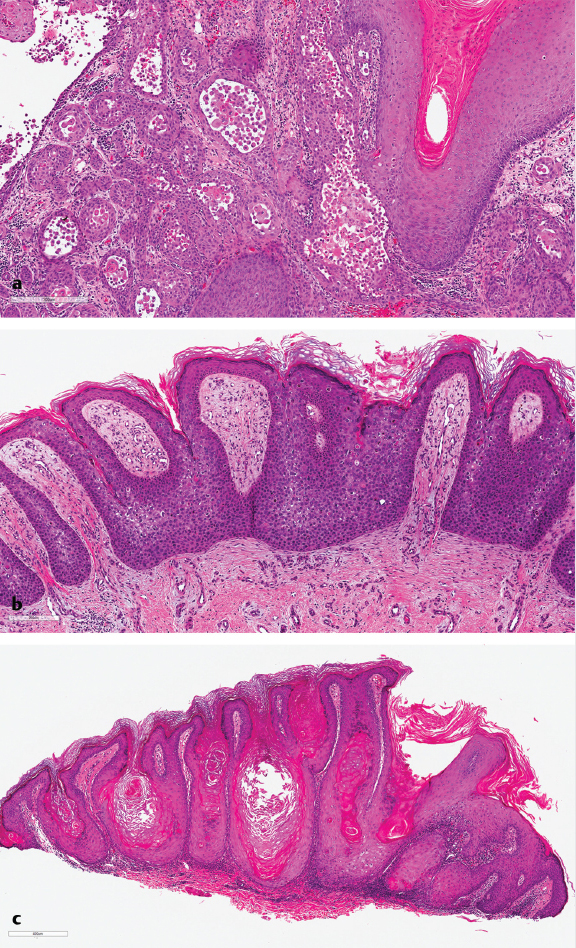
Fig. 11.2e) usually shows at least focal retraction artifact, stromal mucin, increased mitosis, and a lack of papillary mesenchymal bodies, as distinguishing factors from trichoepitheliomas (![]() Fig. 11.3a–c). Infiltrative BCCs show thin, linear basaloid tumor strands growing in an infiltrative pattern. When the same type of growth becomes even more spiked and associated with a densely sclerotic stroma, tumors are called morpheaform BCC. Perineural invasion is another important pathologic prognostic feature in BCC, and BCC tumors with this feature (
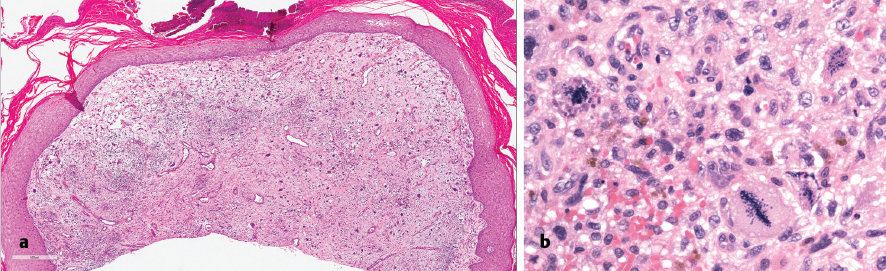
Fig. 11.3a–c). Infiltrative BCCs show thin, linear basaloid tumor strands growing in an infiltrative pattern. When the same type of growth becomes even more spiked and associated with a densely sclerotic stroma, tumors are called morpheaform BCC. Perineural invasion is another important pathologic prognostic feature in BCC, and BCC tumors with this feature (![]() Fig. 11.3d) have higher rates of recurrence and morbidity. While studies on treatment protocols in this setting are relatively limited, Mohs surgery appears to confer better outcome, and adjuvant radiotherapy may be considered.7
Fig. 11.3d) have higher rates of recurrence and morbidity. While studies on treatment protocols in this setting are relatively limited, Mohs surgery appears to confer better outcome, and adjuvant radiotherapy may be considered.7
![]() Fig. 11.2e), or clear cell types, IHC staining may be required. BCC stains in a pattern similar to the follicular infundibulum and will be positive for both high- and low-molecular-weight cytokeratins, BerEP4, Bcl-2 (diffuse), and Ki-67 (20–40% proliferative index), and will show exclusion of CK20 + Merkel’s cells.8 A recent study by Nedved et al revealed that while there is only fair concordance between dermatopathologists with regard to specific BCC typing, there is substantial agreement when tumors were reclassified into a two-tiered system of high- and low-risk phenotypes.9 As such, BCCs often do not require a second pathologic opinion.
Fig. 11.2e), or clear cell types, IHC staining may be required. BCC stains in a pattern similar to the follicular infundibulum and will be positive for both high- and low-molecular-weight cytokeratins, BerEP4, Bcl-2 (diffuse), and Ki-67 (20–40% proliferative index), and will show exclusion of CK20 + Merkel’s cells.8 A recent study by Nedved et al revealed that while there is only fair concordance between dermatopathologists with regard to specific BCC typing, there is substantial agreement when tumors were reclassified into a two-tiered system of high- and low-risk phenotypes.9 As such, BCCs often do not require a second pathologic opinion.
11.3 Squamous Cell Carcinoma
![]() Fig. 11.4a), Bowenoid (
Fig. 11.4a), Bowenoid (![]() Fig. 11.4b), and verrucous (
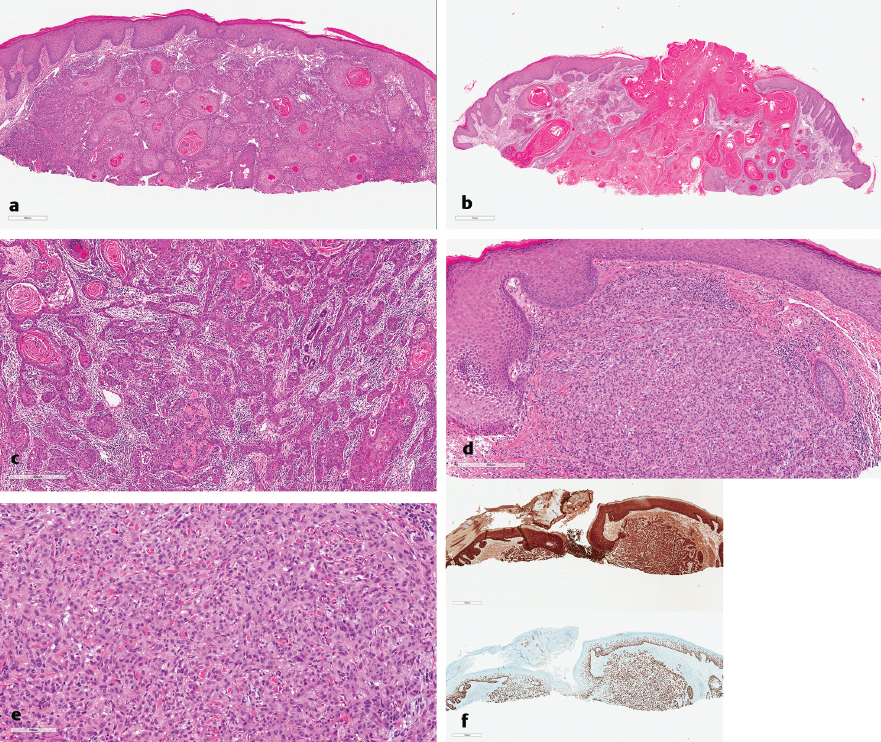
Fig. 11.4b), and verrucous (![]() Fig. 11.4c), such typing is not necessary to include (though often incorporated) in the reporting template. The histologic grade, rather, is the required information because decreasing levels of differentiation are associated with increasing risk of recurrence. Well-differentiated cSCC will closely resemble normal epithelium, but often shows an irregular border of invasive islands with a desmoplastic host response, paradoxical maturation with descent into the dermis, and subtle nuclear atypia (
Fig. 11.4c), such typing is not necessary to include (though often incorporated) in the reporting template. The histologic grade, rather, is the required information because decreasing levels of differentiation are associated with increasing risk of recurrence. Well-differentiated cSCC will closely resemble normal epithelium, but often shows an irregular border of invasive islands with a desmoplastic host response, paradoxical maturation with descent into the dermis, and subtle nuclear atypia (![]() Fig. 11.5a). Keratoacanthomas (
Fig. 11.5a). Keratoacanthomas (![]() Fig. 11.5b) appear to represent a unique form of invasive, well-differentiated squamous cell carcinoma that will often involute on its own, possibly due to the relatively increased expression of apoptotic genes.16 As such, well-differentiated SCC and keratoacanthomas perform the best clinically. Moderately differentiated cases show less obvious squamous features (
Fig. 11.5b) appear to represent a unique form of invasive, well-differentiated squamous cell carcinoma that will often involute on its own, possibly due to the relatively increased expression of apoptotic genes.16 As such, well-differentiated SCC and keratoacanthomas perform the best clinically. Moderately differentiated cases show less obvious squamous features (![]() Fig. 11.5c). Poorly differentiated (
Fig. 11.5c). Poorly differentiated (![]() Fig. 11.5d, e) squamous cell carcinoma, which may require IHC staining for confirmation (
Fig. 11.5d, e) squamous cell carcinoma, which may require IHC staining for confirmation (![]() Fig. 11.5f), and undifferentiated, sarcomatoid (
Fig. 11.5f), and undifferentiated, sarcomatoid (![]() Fig. 11.6a-BSCC) squamous cell carcinoma, which requires clinical correlation, a precursor lesion, or focal IHC staining positivity by definition, have increased risk for recurrence. As such, both poor and de-differentiation are histologic features which upstage a patient from a pT1 to a pT2 tumor.14
Fig. 11.6a-BSCC) squamous cell carcinoma, which requires clinical correlation, a precursor lesion, or focal IHC staining positivity by definition, have increased risk for recurrence. As such, both poor and de-differentiation are histologic features which upstage a patient from a pT1 to a pT2 tumor.14
![]() Table 11.2). Perineural invasion is more common in larger tumors (
Table 11.2). Perineural invasion is more common in larger tumors (![]() Fig. 11.7a), as is lymphovascular invasion.
Fig. 11.7a), as is lymphovascular invasion.
![]() Fig. 11.7b). If positive margins are found after initial excision, then Mohs micrographic surgery or resection with CCPDMA is typically indicated, especially if graft placement is necessary. Measurement of distance to the margin is not required information, but is often reported.
Fig. 11.7b). If positive margins are found after initial excision, then Mohs micrographic surgery or resection with CCPDMA is typically indicated, especially if graft placement is necessary. Measurement of distance to the margin is not required information, but is often reported.
![]() Fig. 11.7c). The size, number, and site (ipsilateral or bilateral) of lymph node involvement is associated with clinical outcome, with meta-static deposit size the most important factor.20,21 As such, these are required components of the templated pathology report.
Fig. 11.7c). The size, number, and site (ipsilateral or bilateral) of lymph node involvement is associated with clinical outcome, with meta-static deposit size the most important factor.20,21 As such, these are required components of the templated pathology report.
11.4 Malignant Melanoma
![]() Fig. 11.8a), nevoid (
Fig. 11.8a), nevoid (![]() Fig. 11.8b, c), and Spitzoid (
Fig. 11.8b, c), and Spitzoid (![]() Fig. 11.8d, e) melanomas can show histopathologic overlap with dysplastic nevi (
Fig. 11.8d, e) melanomas can show histopathologic overlap with dysplastic nevi (![]() Fig. 11.9a) or recurrent nevi (
Fig. 11.9a) or recurrent nevi (![]() Fig. 11.9b-d) and Spitz nevi (
Fig. 11.9b-d) and Spitz nevi (![]() Fig. 11.9e), respectively.21 Meanwhile, the so-called atypical Spitz tumor/nevus is a diagnosis that often requires ancillary testing for confirmation due to the lack of consistent distinguishing histologic features from melanoma. Farmer et al illustrated that within a panel of eight expert pathologists, diagnostic discordance between two or more panel members was observed in 38% of melanocytic lesions.25 The experimental design and premise of this study has been questioned by some who insist that the majority of cases can be accurately classified; and that descriptive reporting on the uncertain malignant potential of particular lesions is in fact permissible.27 Contemporary studies done by Niebling et al at the Melanoma Institute Australia (MIA) on 5,011 MIA and non–MIA-matched reports on the same primary melanomas found significant changes in the diagnosis, AJCC-T classification, and treatment recommendations after pathology review by melanoma pathologists, with moderate concordance demonstrated for various tumor staging parameters. Because of this, the recommendation that pathology review be considered for all patients attending specialist melanoma treatment centers has been made.28,29 Needless to say, it is important to trust the dermatopathologist diagnosing melanocytic lesions. Likewise, it is important that pathology reports of at least borderline melanocytic lesions document key diagnostic criteria (microscopic features) on which the diagnosis was based, and describe any areas of uncertainty.
Fig. 11.9e), respectively.21 Meanwhile, the so-called atypical Spitz tumor/nevus is a diagnosis that often requires ancillary testing for confirmation due to the lack of consistent distinguishing histologic features from melanoma. Farmer et al illustrated that within a panel of eight expert pathologists, diagnostic discordance between two or more panel members was observed in 38% of melanocytic lesions.25 The experimental design and premise of this study has been questioned by some who insist that the majority of cases can be accurately classified; and that descriptive reporting on the uncertain malignant potential of particular lesions is in fact permissible.27 Contemporary studies done by Niebling et al at the Melanoma Institute Australia (MIA) on 5,011 MIA and non–MIA-matched reports on the same primary melanomas found significant changes in the diagnosis, AJCC-T classification, and treatment recommendations after pathology review by melanoma pathologists, with moderate concordance demonstrated for various tumor staging parameters. Because of this, the recommendation that pathology review be considered for all patients attending specialist melanoma treatment centers has been made.28,29 Needless to say, it is important to trust the dermatopathologist diagnosing melanocytic lesions. Likewise, it is important that pathology reports of at least borderline melanocytic lesions document key diagnostic criteria (microscopic features) on which the diagnosis was based, and describe any areas of uncertainty.
Clark’s level | cSCC risk of recurrence and metastases | |
I | Tumor confined to the epidermis (in situ) | Low |
II | Tumor invasion into the papillary dermis | |
III | Tumor at the junction of the papillary and reticular dermis | |
IV | Tumor invasion into the reticular dermis | High |
V | Tumor invasion into the subcutaneous fat | |
Abbreviation: cSCC, cutaneous squamous cell carcinoma.
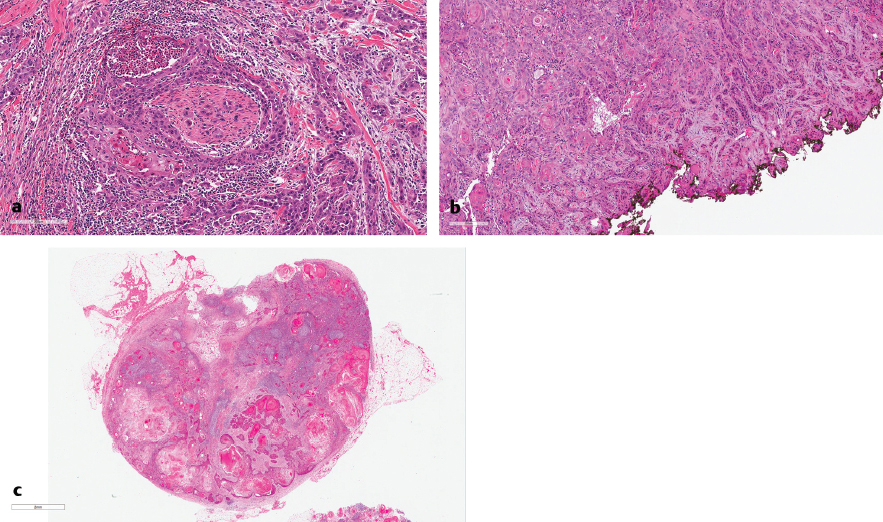
Fig. 11.7 (a) Cutaneous squamous cell carcinoma (cSCC), perineural invasion. (b) cSCC, positive inked margin. (c) cSCC, lymph node metastasis.
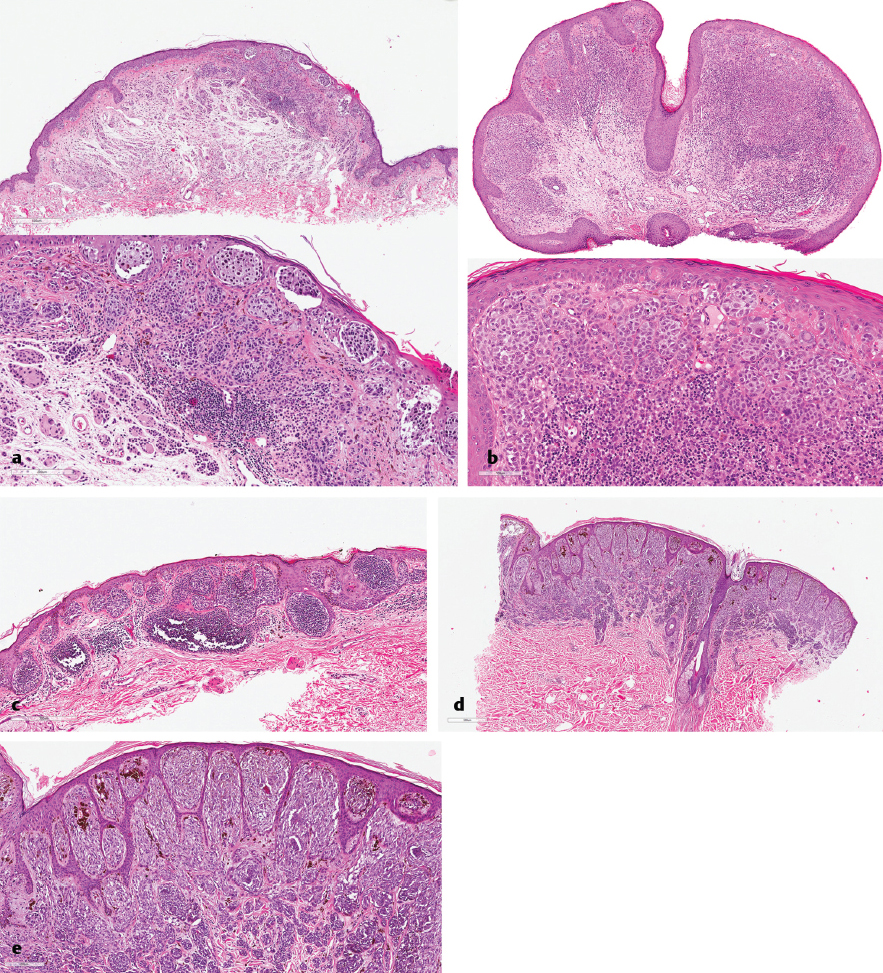
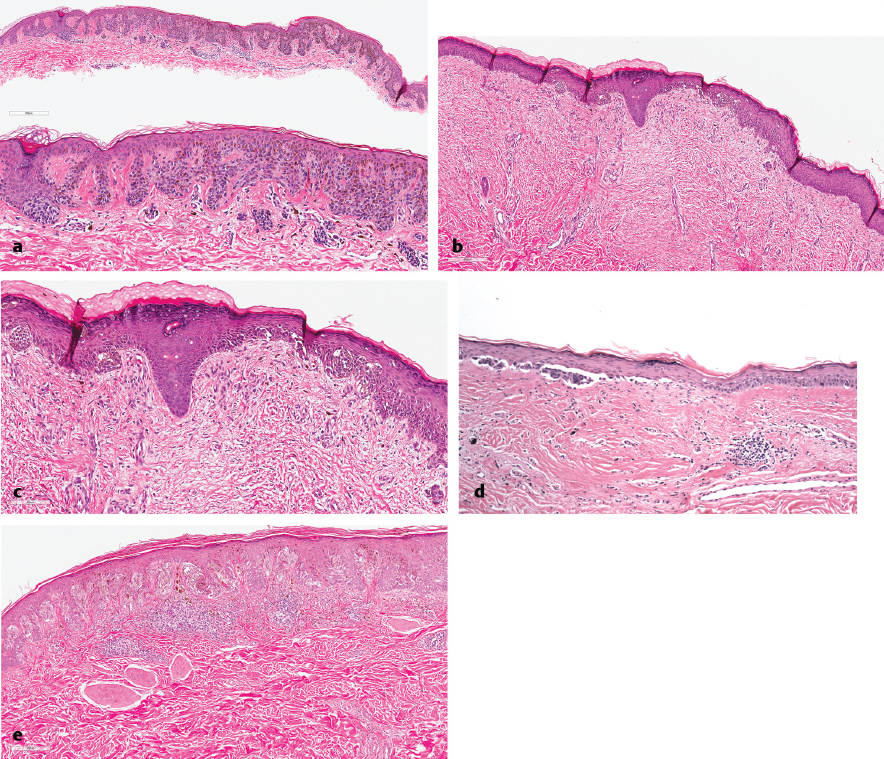
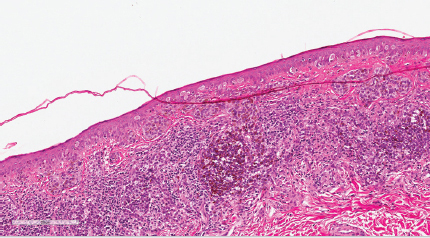
Fig. 11.10 Melanoma, superficial spreading with pagetoid spread.
Clinical information can be crucially important in the diagnosis of melanoma. Older patient age, increased signs of solar damage, and large lesional diameter (> 6 mm) will immediately alter the perspective through which a biopsy is reviewed. Numerous criteria are considered, both in number and severity, in the assessment for malignancy. In general, melanomas tend to show many forms of asymmetry. These include asymmetry of low power silhouette, lateral border cell distribution, cytologic features, pigmentation, inflammatory host response, and nesting architecture. Consumption of the epidermis (![]() Fig. 11.8e) and pagetoid spread of melanocytes (
Fig. 11.8e) and pagetoid spread of melanocytes (![]() Fig. 11.10) are emblematic clues to melanoma.30
Fig. 11.10) are emblematic clues to melanoma.30
Owing to the diagnostic difficulty sometimes associated with melanoma and its capacity to spread relatively early in evolution, it is our practice that all melanomas diagnosed by outside pathologists be reviewed by pathologists within our institution prior to definitive treatment at our institution. For those surgeons treating patients in the community, it is likely not practical to have every melanoma reviewed by an outside pathologist. However, there are certain red flags that surgeons can be aware of which should reflexively lead to a second pathologist’s opinion (![]() Table 11.3). When a second opinion is sought, it should often be from a dermatopathology group at a tertiary-care center who more regularly diagnose melanomas, and who has access to ancillary diagnostic tests which can aid in the differential diagnosis.
Table 11.3). When a second opinion is sought, it should often be from a dermatopathology group at a tertiary-care center who more regularly diagnose melanomas, and who has access to ancillary diagnostic tests which can aid in the differential diagnosis.
Table 11.3 Common scenarios for requesting a second opinion in the diagnosis of melanocytic lesions
Lesions with overlapping or ambiguous histopathologic features | Dysplastic nevi Spitzoid lesions |
Obscuring histopathologic features | Inflammation Regression Melanocytic lesions arising in association with a previous biopsy |
Unusual clinical features | Young age, unusual location |
11.4.1 Diagnostic Aids in Melanoma
Comparative Genomic Hybridization
Ancillary tests that assist in distinguishing potentially lethal melanomas from benign melanocytic nevi with atypical histopathologic features are available. The arguably most robust ancillary method that has emerged over the past decade is cytogenetic analysis. Based on the pioneering work by Bastian and colleagues, melanomas were found to commonly carry chromosomal copy number changes, while these are absent or rare in nevi. The preferred cytogenetic method is comparative genomic hybridization (CGH), because it tests all chromosomes. CGH determines DNA copy number by the competitive hybridization of two differentially labeled DNA populations (tumor DNA and normal control DNA) hybridized to a substrate (representing the genome). The ratio of the two differentially labeled signals is used to determine increases and decreases in copy number of tumoral DNA at a given genomic coordinate. Multiple studies have shown semi-characteristic chromosomal gains and losses in melanomas that were not seen in nevi.31,32 Isolated 11p gains were seen in Spitz nevi and not melanomas.32 Higher resolution array-based CGH studies have allowed for the identification of recurrent genetic abnormalities more common in unique types of melanomas arising in various contexts (![]() Table 11.4).33
Table 11.4).33
Fluorescence In Situ Hybridization
Multiprobe fluorescence in situ hybridization (FISH) assays, which were based on existing CGH data, have been tested in their ability to discriminate melanomas and nevi. Of the various combinations tested, those probes to loci 6p25 (RREB1), 6p23 (MYB), CEP6 (Centromere 6, for discrimination of aneuploidy and polyploidy), and 11q13 (CCND1) proved to have the highest sensitivity and specificity (![]() Fig. 11.11 and
Fig. 11.11 and ![]() Table 11.5).34 This probe set shows a range of reported sensitivities and specificities depending on the diagnostic problem and particular study (
Table 11.5).34 This probe set shows a range of reported sensitivities and specificities depending on the diagnostic problem and particular study (![]() Table 11.635). Multiple studies using the same four-probe FISH set have reported diagnostic utility for distinguishing melanoma from nevi,36,37,38 and particular utility in various diagnostically difficult circumstances (
Table 11.635). Multiple studies using the same four-probe FISH set have reported diagnostic utility for distinguishing melanoma from nevi,36,37,38 and particular utility in various diagnostically difficult circumstances (![]() Table 11.6). Of note, pigmented spindle cell nevi-like39 and desmoplastic melanoma40 have reduced FISH sensitivity (73 and 47%, respectively). Homozygous loss of 9p21 (CDKN2A) and gains in 8q24 (MYC) are additional FISH parameters for the diagnosis of cutaneous melanoma. When such probes are used in combination with the previously mentioned four probes, the sensitivity and specificity of the test is improved to 94 and 98%, respectively, in unambiguous lesions.41,42,43,44,45 Additional studies will be needed to determine the sensitivity and specificity in ambiguous lesions. Due to the possibility of false-negative or false-positive cytogenetic test results, CGH and, in particular, FISH data need to be carefully correlated with clinical and histopathologic findings. A diagnosis should not solely be based on cytogenetic results.
Table 11.6). Of note, pigmented spindle cell nevi-like39 and desmoplastic melanoma40 have reduced FISH sensitivity (73 and 47%, respectively). Homozygous loss of 9p21 (CDKN2A) and gains in 8q24 (MYC) are additional FISH parameters for the diagnosis of cutaneous melanoma. When such probes are used in combination with the previously mentioned four probes, the sensitivity and specificity of the test is improved to 94 and 98%, respectively, in unambiguous lesions.41,42,43,44,45 Additional studies will be needed to determine the sensitivity and specificity in ambiguous lesions. Due to the possibility of false-negative or false-positive cytogenetic test results, CGH and, in particular, FISH data need to be carefully correlated with clinical and histopathologic findings. A diagnosis should not solely be based on cytogenetic results.
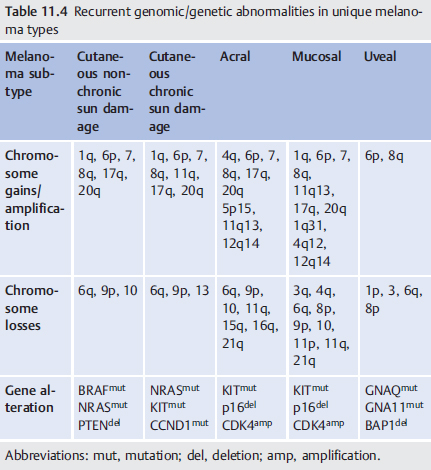
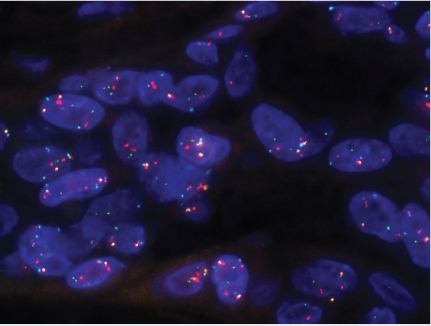
Fig. 11.11 Melanoma fluorescence in situ hybridization: Most cells show three red signals (6p), two green (11q), two cyan (CEP6), and one to two gold (6q).
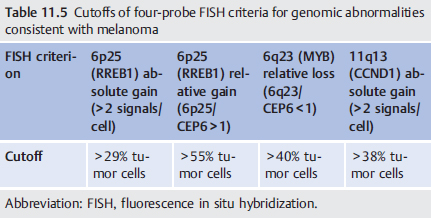
Table 11.6 Utility of FISH in the diagnosis of melanocytic lesions
Diagnostic problem | FISH sensitivity/specificity |
Nevus vs. Melanoma | 80–95%; 90–98% |
Histopathologically ambiguous melanocytic tumors | 43–100%; 50–80% |
Subcapsular nodal nevus vs. metastatic melanoma | |
Microstaging primary melanomas arising in precursor nevi | |
Primary nevus vs. nevus-like metastatic melanoma | |
Prognosis of melanoma |
Abbreviation: FISH, fluorescence in situ hybridization.
Myriad MyPath
In addition to FISH, gene expression microarray studies have attempted to distinguish primary cutaneous melanomas from various types of nevi. Myriad Genetics, Inc. has developed a 23-gene expression signature clinically validated to differentiate benign nevi from MM with a sensitivity of 89% and a specificity of 93%.46 The genes in this expression signature include those involved in immune function and those involved in cell differentiation and cell cycle. However, this test is currently of unproved value for ambiguous lesions, since the test has so far only been compared to consensus diagnoses of the diagnostically straightforward nevi and melanoma.
Immunohistochemical Stains in Melanoma
Although various investigators have at various times claimed that immunohistochemistry can aid in the distinction of nevus from melanoma, there are no robust data available, and we caution against using staining patterns, such as for HMB-45 and p16 for diagnosis.47 It is also questionable whether immunohistochemistry, such as for p16, has independent prognostic significance.48 The main value of immunohistochemistry is to verify the line of differentiation of amelanotic tumors, such as for the distinction of melanoma from sarcoma, and better visualization of melanocytes in the context of inflammation (e.g., lentigo maligna with lichenoid inflammatory reaction) or improved detection of small melanocyte deposits in the sentinel lymph node. More recently, immunohistochemistry has also become relevant for a quick assessment of mutation status, such as by using the antibody VE1 to detect the most common form of BRAF gene mutation—BRAFV600E.49
11.4.2 Histologic Subtypes of Melanoma
The common melanoma histologic subtypes, superficial spreading melanoma, nodular melanoma, and desmoplastic and lentigo maligna melanoma, show fairly good clinicopathologic and molecular concordance, but have no prognostic significance beyond that afforded by Breslow’s thickness. Their categorically discrepant clinical presentations and skewed molecular signatures are of interest, however, in so much as they may lead to variant algorithms for treatment when additional targeted therapies become available. This histologic subclassification also brings to light various clinical and histologic mimickers, and they are included below for interest.
Superficial Spreading Melanoma
MM is typically characterized by a proliferation of malignant melanocytes, which begins to grow horizontally along the dermal–epidermal junction and within the epidermis, as part of the radial growth phase, prior to entering the vertical growth phase characterized by progressively thicker dermal involvement. This relationship shows a broader intraepidermal component than dermal component. The most common of melanoma subtypes, these lesions are often characterized by pagetoid spread of melanocytes above the dermal–epidermal junction; irregularly shaped, sized, and placed melanocytic nests; and consumption of and clefting from the epidermis. Superficial spreading melanoma is typically found on intermittently sun-exposed areas as well as arising from pre-existing nevi. The main differential diagnosis is with dysplastic nevi; nevi of special sites such as scalp, breast, or genitals; traumatized nevi; or persistent/recurrent nevi. The most common genetic driver in superficial spreading melanomas is BRAF mutation, which appears to correlate with more epithelioid cytology in tumor cells and more pagetoid scatter of tumor cells.50,51,52
Superficial spreading melanoma will typically show mostly epithelioid cytomorphology. In banal nevi, melanocytes are often more epithelioid the younger the patient’s age is. Indeed, Spitz nevi, which occur mostly in children and young adults, are the most epithelioid of all nevi. Congenital nevi are typically very epithelioid superficially, often with patchy single cells in the epidermis. However, their overall architecture is very orderly with marked maturation upon descent into the dermis. Epithelioid cytomorphology in older individuals with background sun damage should cause pause and closer examination to exclude a nevoid melanoma.
Related posts:
 Mohs Micrographic Surgery’s Role in the Treatment of Skin Cancer
Mohs Micrographic Surgery’s Role in the Treatment of Skin Cancer
 Common Reconstructive Techniques after Facial Skin Cancer Excision
Common Reconstructive Techniques after Facial Skin Cancer Excision
 Clinical Detection of Skin Cancer
Clinical Detection of Skin Cancer
 Role of Radiotherapy in the Treatment of Skin Malignancies
Role of Radiotherapy in the Treatment of Skin Malignancies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


