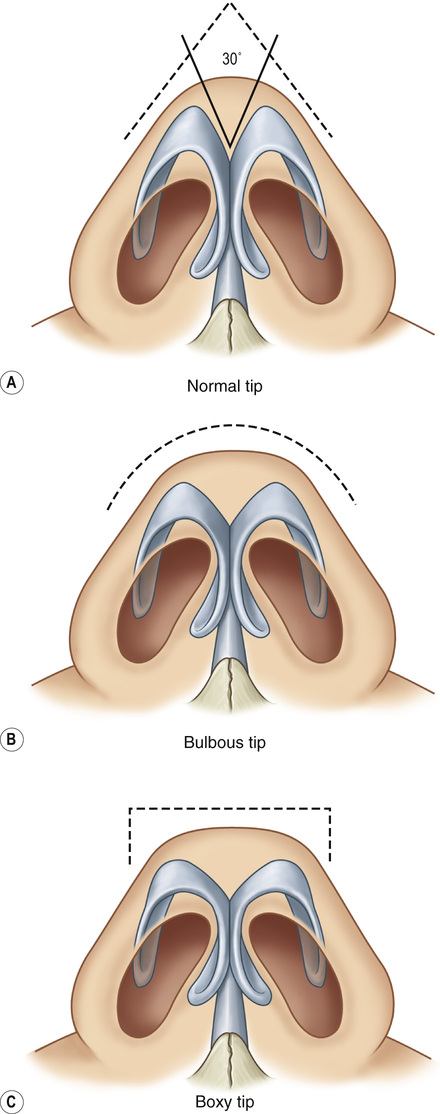
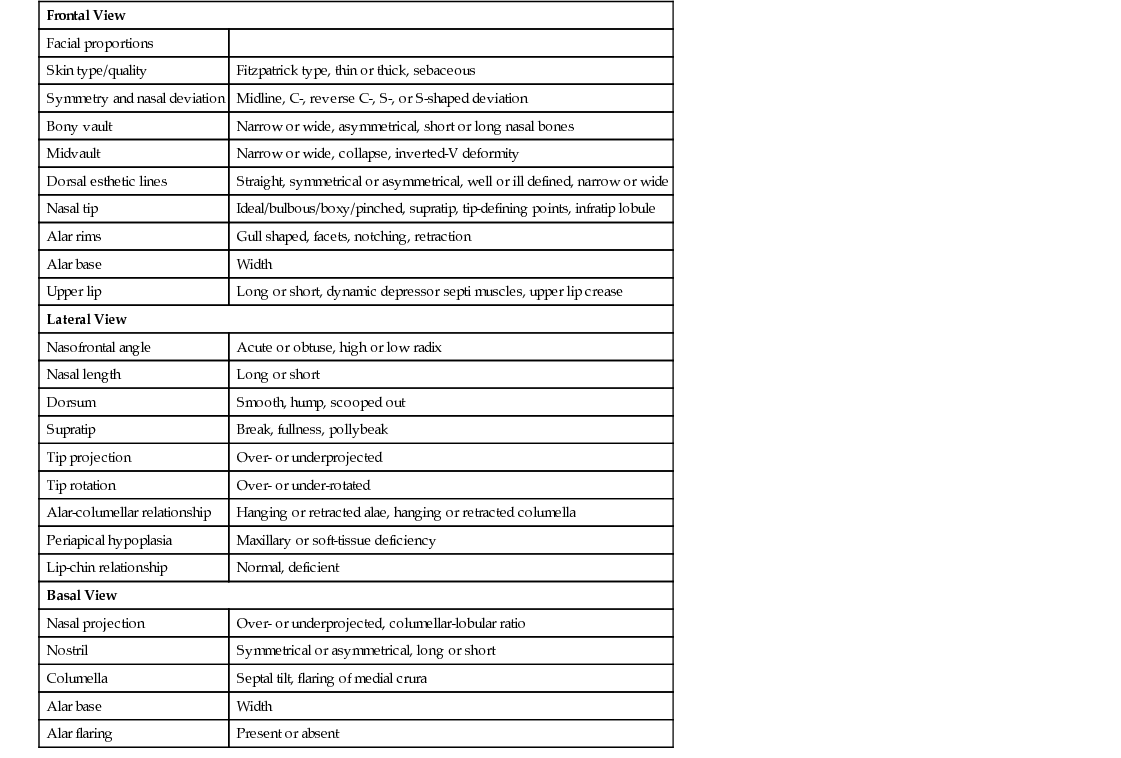
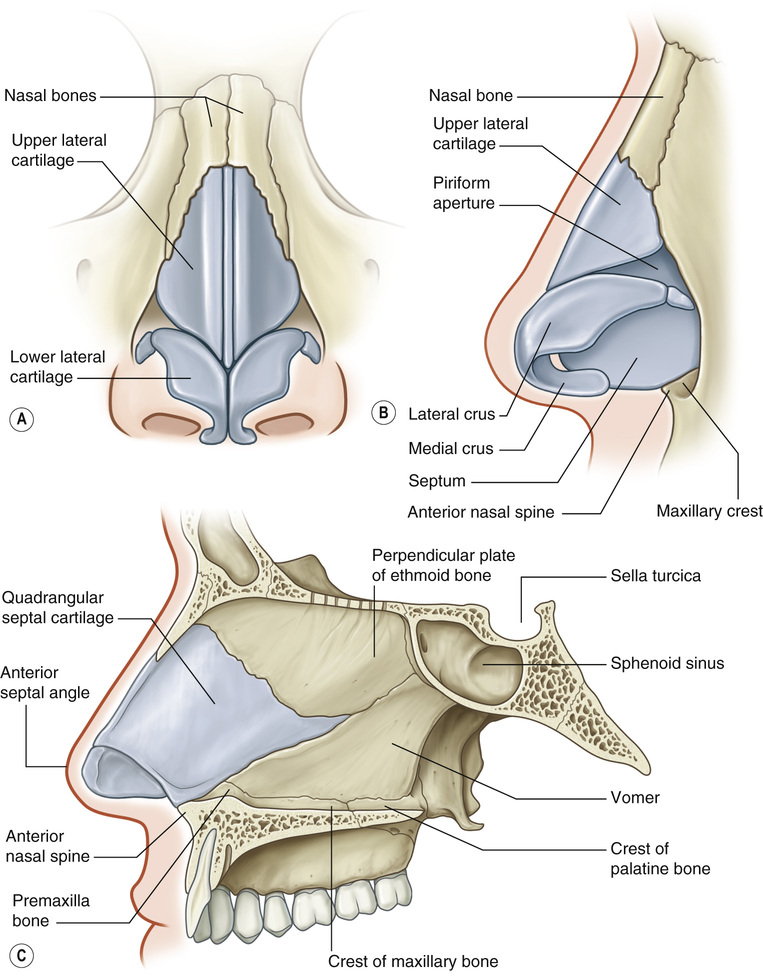
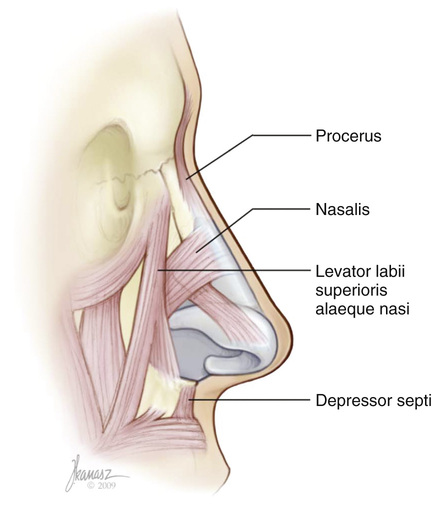
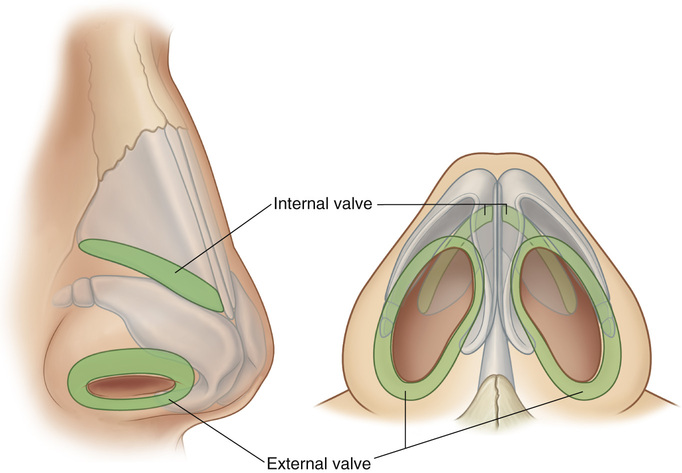
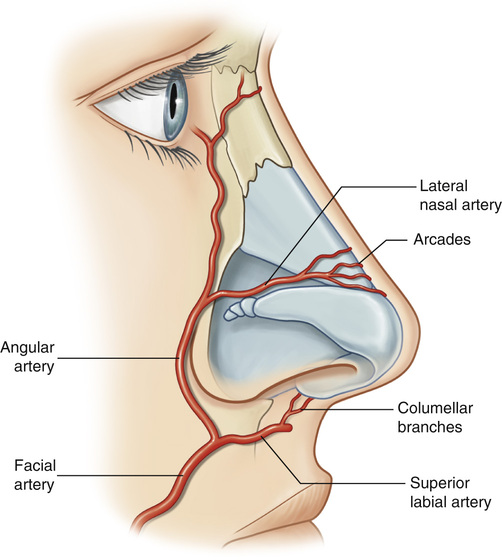
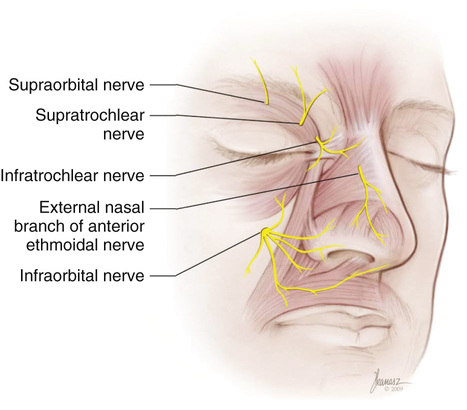
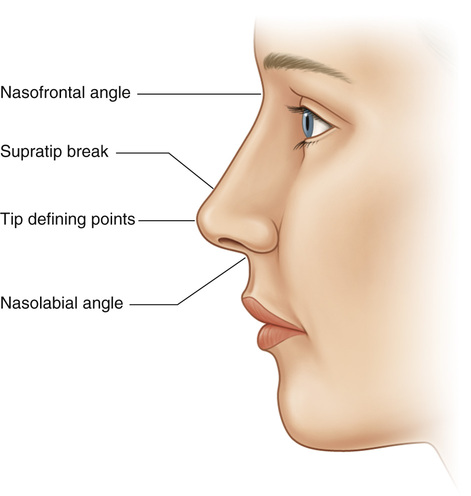
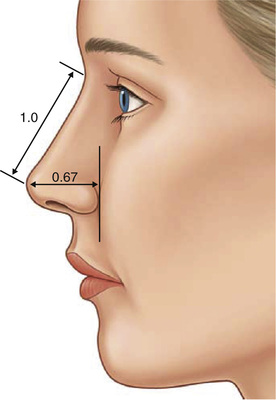
1. The nose is a system of two closely related layers. • Outer layer: Soft, elastic sleeve that slides over the semirigid inner framework • Inner layer: Semirigid framework ▪ Nasal lining: Mucosal inner layer (see Figure 27.1) 2. Muscles of the nose: Crucial to dynamic function of the nasal valve and airway • Facial paralysis (cranial nerve [CN] VII) can cause nasal airway obstruction on side of lesion • Depressor septi nasi: Depresses nasal tip (see Figure 27.2) 3. Nasal valves • INV (between septum and ULC): 10 to 15 degrees; if <10 = spreader grafts. ▪ Contributes the most to nasal air-flow resistance • External nasal valve (ENV; at genu of LLC and nares): Often from over-resection of LLC; treatment: Alar batten grafts (see Figure 27.3) 4. Vascular supply to the nose • Nasal tip: Columellar artery (superior labial a. → facial a. → external carotid a.), lateral nasal a. (angular a. → facial a. → external carotid a.) • Nasal sidewall, dorsum: Angular a. and lateral nasal a. ▪ The lateral nasal a. also perfuses the nasal tip during open rhinoplasty. • Posterior nasal septum: Sphenopalatine a. • Upper/central nasal septum: Posterior ethmoid a. (see Figure 27.4). 5. Sensory innervation of the nose • External branch of the anterior ethmoidal nerve: Nasal tip; vulnerable to damage during endonasal rhinoplasty procedures • Infraorbital nerve: Lower lateral half of the nose and columellar skin • Infratrochlear nerve: Cephalic portion of the nasal sidewalls and the skin overlying the radix • Supraorbital nerve also innervates the skin of the radix. • Supratrochlear nerve supplies sensation to the forehead skin. • The nose is made up of 9 esthetic subunits. • Conduit for oxygenated air to enter the lungs • Reservoir for warming and humidifying inspired air • Filters air and provides first-line immune defense against pathogens • The middle meatus marks the path of primary air flow within the nasal cavity. • Causes of obstruction include any abnormality that results in increased nasal resistance and decreased air flow (e.g., septal deviation, trauma, nasal valve collapse, turbinate hypertrophy, intranasal masses) ▪ INV incompetence and/or collapse thought to be the most common cause • In cases of rhinitis and turbinate hypertrophy, preoperative medical treatment is recommended. ▪ Viral rhinitis: Oral/topical decongestants 1. Nasofrontal angle: Males, 120 to 130 degrees; females, 115 to 125 degrees 2. Nasolabial angle: Males, 90 to 95 degrees; females, 100 to 105 degrees 3. Tip projection: Equal to base width; 2/3 length of nose (see Figure 27.7) 4. Base width: Equal to intercanthal distance 5. Angle of divergence refers to middle crura of LLC; the angle between R and L middle crus while looking at the nose from anterioposterior (AP) view. • Ideal angle: 30 to 60 degrees; >60 = boxy tip, <30 = narrow tip (see Figure 27.8) 6. The nostrils should have a teardrop configuration, with the diameter of the base slightly larger than the diameter of the apex. • The long axis of each nostril points in a slight medial direction (see Table 27.1). 3. The Asian nose is characterized by alar flare, a bulbous nasal tip, a short retracted columella (i.e., no columellar show), thick subcutaneous tissue, and a wide, flat nasal dorsum. • Asian rhinoplasty generally focuses on augmentation of the nasal dorsum with an alloplastic implant. ▪ Silicone implants are especially popular throughout Asia. • Caused by prominence of the caudal septum or convexity of the caudal margin of the medial crura • Treatment options: Resection of the caudal margin of the medial crura 5. Esthetic septorhinoplasty carries a high incidence of postoperative patient dissatisfaction. • Patient selection is critical. • Most common reasons for dissatisfaction ○ Patients with unrealistic expectations or excessive demands ○ Patients who are indecisive, immature, secretive, motivated by others, or unstable ○ Patients with body dysmorphic disorder (BDD) • Management of the dissatisfied patient: Frequent communication and follow-up 6. BDD • Affects 7% to 15% of all plastic surgery patients • Characterized by the degree of concern being much greater than the degree of deformity; patients are generally unaware that concerns are excessive. • Most patients with BDD are single (70% never married) and up to 50% have suicidal ideation. • Critical for planning, demonstration of results, and patient education • Lighting, patient positioning, and obtaining standard views are paramount for best photographic results. ▪ Standard views include frontal, oblique, lateral, basilar, cephalic, and smiling lateral
Rhinoplasty and Nasal Reconstruction
Anatomy of the Nose
Nasal Physiology
Ideal Nasal Analysis (see Figure 27.6)
Preoperative Considerations
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Rhinoplasty and Nasal Reconstruction
Chapter 27
 their nasal length.
their nasal length.