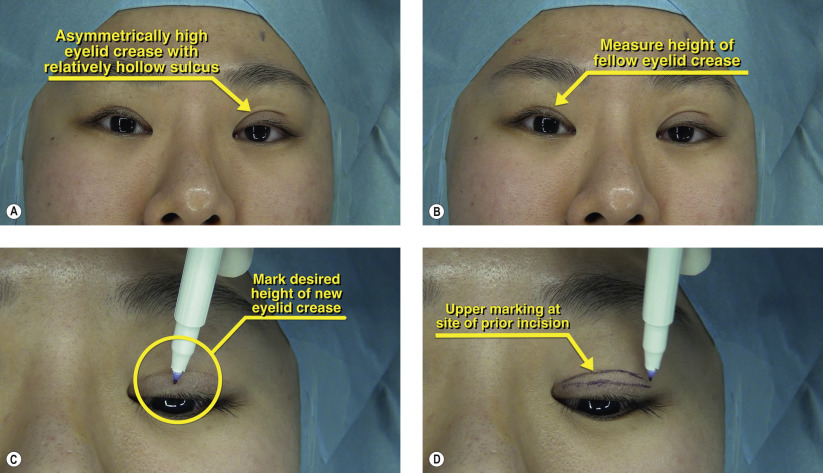
| Eyelid crease asymmetry |
| High placement of surgical eyelid crease |
| Hollowing of superior sulcus |
| History of prior surgery to create eyelid crease |
| Amount of skin reserve above existing crease |
| Presence or absence of upper eyelid fat |
| Presence of co-existing ptosis |
| Shape and height of current and desired crease |
Introduction
Revision of a high, asymmetric Asian upper eyelid crease is a challenging surgical problem. There are multiple etiologies including a high skin crease incision, excessive removal of orbital fat, damage to the levator, improper placement of crease formation sutures, and iatrogenic surgical trauma. Prior to undertaking surgical revision, the patient’s expectations should be kept low and the need for subsequent surgeries must be discussed. Alternative treatments, such as upper eyelid hyaluronic acid fillers, can be discussed if revision surgery is not an option.
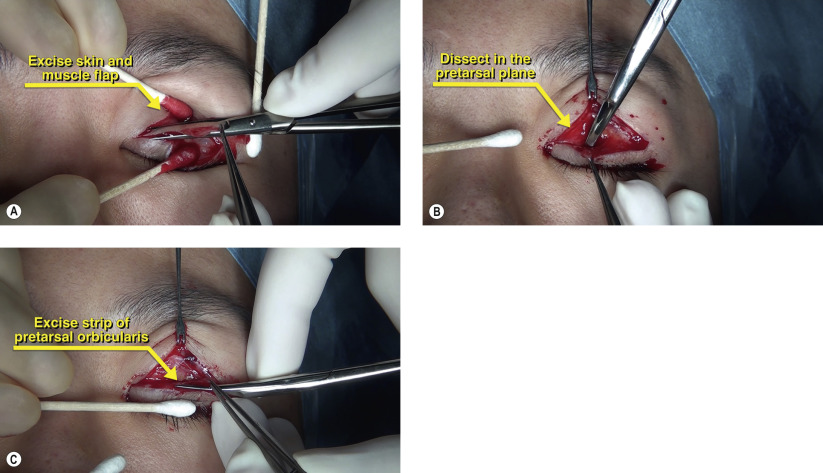
The general principles of crease lowering are to excise an ellipse of skin and orbicularis to the desired level of the new crease and then inferior advancement of a preaponeurotic fat pedicle as a buffer to prevent multiple crease formation followed by placement of crease formation sutures.
Surgical Technique