Introduction
Capsular contracture has for decades been the most common complication associated with aesthetic and reconstructive breast surgery. Although the exact mechanism or cause is still unclear, many causes have been implicated, the most feasible include hypertrophic scarring, the infectious theory, or potentially both. The hypertrophic theory implicates that either blood or seroma fluid surrounding a breast implant induces the capsular contracture, and the role of a myofibroblast in this process has been implicated by some. The infectious theory has the most supporting evidence and has become the predominant theory, implicating low-level bacterial contamination and the formation of a biofilm around the breast prosthesis, either introduced at the time of implantation or seeding of the implant space from a transient bacteremia. The exact cause is most likely multifactorial. The significance of this pathologic process cannot be overstated because capsular contracture has consistently been the leading indication for revision after placement of breast implants, ranging from 15%–30%, and accounts for nearly 50,000 reoperations annually.
The management of an established capsular contracture may include some non-surgical efforts, but failure to resolve the contracture will generally necessitate surgical intervention. There are many proposed approaches to management, but the best data support implant exchange and new pocket creation as significant to reducing recurrence. The management of the capsule may include a capsulotomy, a total capsulectomy, a near-total or partial capsulectomy, a pocket exchange from subglandular to submuscular, creation of a neosubpectoral pocket, or even implant removal with or without a capsulectomy. The use of acellular dermal matrix (ADM) in treatment of established or recalcitrant capsular contracture has been associated with some of the lowest rates of recurrence.
In this chapter the authors will describe their preferred approaches of a capsulectomy with or without pocket exchange, a neosubpectoral pocket with collapse of the capsule below the new implant, and the selective use of ADM.
Indications and Contraindications
Capsular contracture is a clinical diagnosis made on symptoms and physical examination. Early capsular contractures by definition occur in the first year. It has been thought that most capsular contractures occur in the first year, but long-term breast implant data confirm that capsular contracture based on multiple causes, including seeding from a distant site or silicone leak, may develop any time after breast implant placement. Capsular contractures have classically been graded by the Baker classification ( Table 11.1 ).
| Grade I | Breast is soft and looks natural |
| Grade II | Breast is slightly firm but looks normal |
| Grade III | Breast feels and looks firm |
| Grace IV | Breast is hard, is painful, and looks abnormal |
Surgical intervention is usually reserved for Baker grade III and IV capsular contractures, because these are characterized by visible deformation of the augmentation result and potentially discomfort and pain.
When treating an early capsular contracture as it is evolving, appropriate non-surgical management may be appropriate. This may include manual displacement and massage, oral consumption of a leukotriene inhibitor (Singulair) and/or vitamin E, and the use of external ultrasound therapy. Once a contracture is well-established, this non-surgical approach is less effective.
Surgical intervention is best if performed after the capsular contracture has stabilized. Intervening during the evolution of a capsular contracture is ill-advised, because the inflammatory process makes surgical intervention more challenging and there is a greater risk of recurrence. If possible, surgical intervention is performed when the capsular contracture has stabilized for 3 months. If the breast deformity and associated pain preclude delay, intervention may proceed earlier but potentially may be more challenging secondary to the inflammatory process
Preoperative Evaluation and Special Considerations
The approach to treatment of the capsular contracture is determined by a host of influencing factors. It is first important to recognize the duration of symptoms and the natural history of the evolving capsular contracture. Efforts to manage it non-operatively and determining when it is necessary and optimal to proceed with surgical correction will provide the best chance for success.
The approach to correction is multifactorial, but generally begins with the decision whether to retain the capsule or to remove it. When retaining the capsule, a capsulotomy has been successfully used by many surgeons but with a rather high recurrence rate. If the infectious theory is thought to be the culprit in development of the capsular contracture, it is worrisome to leave the contaminated capsule in place. Another approach when leaving the capsule would be to create a neosubpectoral pocket, effectively creating a fresh new pocket and isolating the implant from the potentially contaminated capsule. More commonly, a total capsulectomy is performed to remove the entire capsule or a partial capsulectomy in some selected cases in which removing the entire capsule was deemed too challenging or dangerous, especially with removal of adherent capsule from the underlying chest wall.
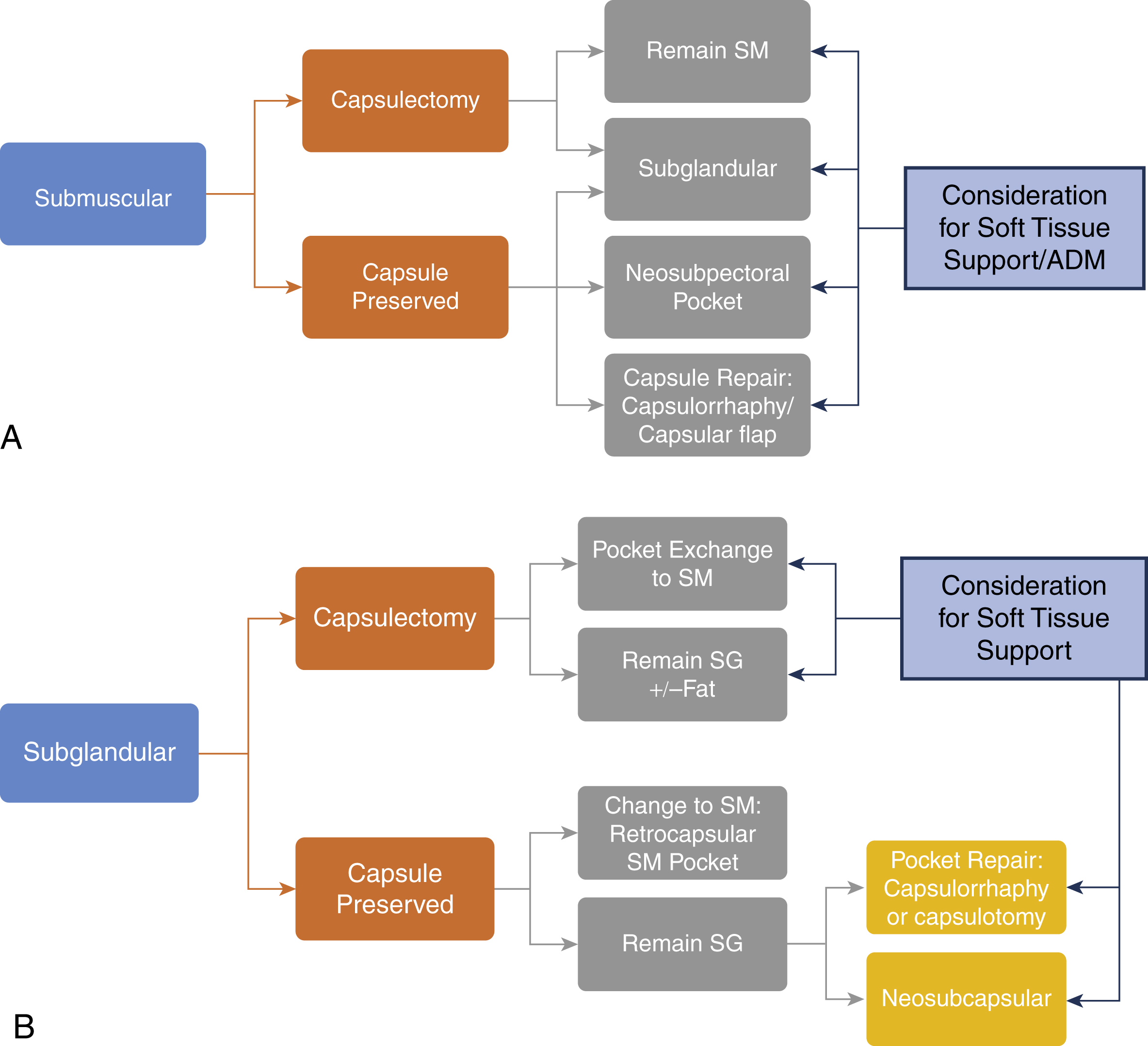
Additionally, it is important to determine pocket placement for the new breast implant. When subglandular, a pocket exchange to a submuscular pocket is commonly performed to create a new pocket. The submuscular pocket is associated with lower capsular contracture rates, provides often much needed additional soft tissue coverage over the implant, and creates a pocket with potentially less bioburden from overlying breast tissue. For all secondary breast cases, we developed an algorithm to guide our pocket decisions for these difficult cases ( Fig. 11.1A, B ).
Finally, preoperative planning must include a decision on the management of the breast implant. Although some surgeons have approached the management of capsular contractures with keeping the same implants in place, there are good data to support improved outcomes with implant exchange. However, it is understandable that there may be no need to change the implant if one is simply performing a capsulotomy for treatment. We think that isolating the implant from the old capsule, creating a new pocket, and exchanging the implant during the revisional procedure are all hallmarks for success in treatment of established capsular contractures. Smooth and textured devices have been used successfully and are often a personal preference. The more cohesive smooth or textured fifth-generation devices with optimal fill can provide improved stability in the upper pole compared to the less cohesive implants. Textured implants are often used in our practice because of the reduced capsular contracture rates (especially in the subglandular pocket) and the positional control and reduced soft tissue stretch the implant provides in what is often an unstable pocket, especially after a capsulectomy ( Box 11.1 ).
- •
Textured implants
- •
Cohesive implants
- •
Shaped implants
- •
Silicone compared with saline implants
- •
Lower profile implants
- •
Smaller implants
- •
Tight, firm breast skin
Surgical Technique
Relevant Surgical Anatomy
When approaching any revision breast surgery, such as the treatment of capsular contracture, additional changes have often occurred to the breast. There is often additional soft tissue thinning and atrophy associated with the implant and tight capsular contracture. This is often more profound with a long history of implantation, increased duration of untreated capsular contracture, subglandular implant placement, and presence of oversized implants. The breast has a rich blood supply from multiple sources, including the internal mammary artery perforators, the lateral thoracic arteries, and the thoracoacromial, anterolateral, and anteromedial intercostal perforators. Previous breast procedures could alter the blood supply, including the location of the augmentation scars, biopsy scars, alterations secondary to a previous mastopexy, and the breast implant pocket location. If a concomitant mastopexy is performed at the time of capsular contracture treatment, an understanding of the remaining blood supply is even more imperative to prevent devascularization and nipple loss.
Preoperative Markings
With the patient in the upright position, the midline and the current inframammary folds (IMFs) are marked. In capsular contracture, the IMFs are often elevated with the contracted implant. In unilateral capsular contracture, the new IMF position on the side of the capsular contracture should be marked at the same level as the opposite unaffected side. If bilateral capsular contractures exist, IMF placement should be based on a biodimensional approach determined by the implant selected. Although many techniques exist, we determine IMF position in cases in which IMF position needs to be altered based on a formula that uses implant dimensions of projection and height. It is important to take the measurement of the IMF at rest and on stretch. The stretch measurement for determining the ideal IMF position is as follows :
IdealNippletofoldDistance=12implantprojection+12implantheightUndermaximalstretch
A line is then drawn vertically 1.5 cm from the midline, marking the extent of dissection medially. This provides a 3-cm intermammary space to avoid overdissection and medial implant displacement postoperatively ( Fig. 11.2 ).

Intraoperative Markings
Once the patient is under anesthesia and has been prepped for the operative procedure, all markings are confirmed and retraced if necessary. The incision location is confirmed and marked for the appropriate distance. The incision can be placed through the scar used in the primary case if inframammary or periareolar. If the original incision was periareolar and an inframammary scar is selected, the new incision is placed at the planned IMF position.
Details of the Procedure
Capsulectomy (Total or Subtotal)
Total and subtotal capsulectomies are considered the gold standard treatment of a capsular contracture and are the most common techniques employed by the authors. A capsulectomy can be performed on subglandular or submuscular capsular contractures.
The capsulectomy is typically performed under general anesthesia. The operative field is injected with 50 cc per side of local anesthetic of 0.25% lidocaine, 0.125% Marcaine, and 1:400,000 epinephrine ( Table 11.2 ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


