Introduction
With the ongoing rise of obesity in the United States a greater emphasis is placed on the importance of weight loss, diet, and exercise. A weight loss of more than 50 lb is classified as massive weight loss, and it can cause significant disfigurement and irregularities. Breasts are significantly affected by these changes. The loss of parenchymal volume combined with skin redundancy and loss of elasticity leads to a flattened, deflated, and ptotic breast appearance. Furthermore, the skin redundancy produces a roll of skin and fat on the lateral border of the breast that extends onto the chest wall. This lateral roll blurs the lateral curve of the breast and often forms one continuous roll of soft tissue, greatly affecting the aesthetics of the breast.
The Pittsburgh Rating Scale is a validated measure introduced in 2005 by our group to classify contour deformities after massive weight loss. This scale helps especially in the breast where the commonly used breast ptosis scales fall short because they are not sufficiently descriptive of the unique breast changes associated with massive weight loss. The scale ranges from 0 to 3:0 includes normal breasts that do not require operative management; 1 includes grade I or II ptosis, or severe macromastia, and it benefits from traditional mastopexy, reduction, or augmentation techniques; 2 includes grade III ptosis, or moderate volume loss, or constricted breast, and it benefits from traditional mastopexy with or without augmentation; and 3 includes severe lateral roll and/or severe volume depletion with loose skin and flattened breast shape, and it benefits from parenchymal reshaping techniques with dermal suspension and consideration of auto-augmentation. Aside from the breast shape, patients who have had massive weight loss also have the characteristic of nipple medialization. This is important to recognize to ensure the nipple–areola complex (NAC) is moved laterally along a true breast meridian.
This chapter highlights the anatomic changes observed in the breast after massive weight loss and provides an overview of the preoperative evaluation, surgical management, and postoperative care to achieve an aesthetically pleasing result.
Indications and Contraindications
Breast reshaping with mastopexy or other techniques is indicated in patients who have lost a massive amount of weight with ptosis, loss of upper pole fullness, and medialization of the NAC. The type of breast reshaping procedure depends on the Pittsburgh Rating Scale and certain clinical criteria. Patients with mild breast deformities should be considered for traditional mastopexy techniques, including short scar approaches. However, dermal suspension and parenchymal reshaping with selective auto-augmentation is indicated in patients with the following conditions:
- •
Grade III breast ptosis
- •
Parenchymal volume loss with flattening of the breast against the chest wall
- •
Inelastic and redundant skin envelope
- •
Medialization of the NAC
- •
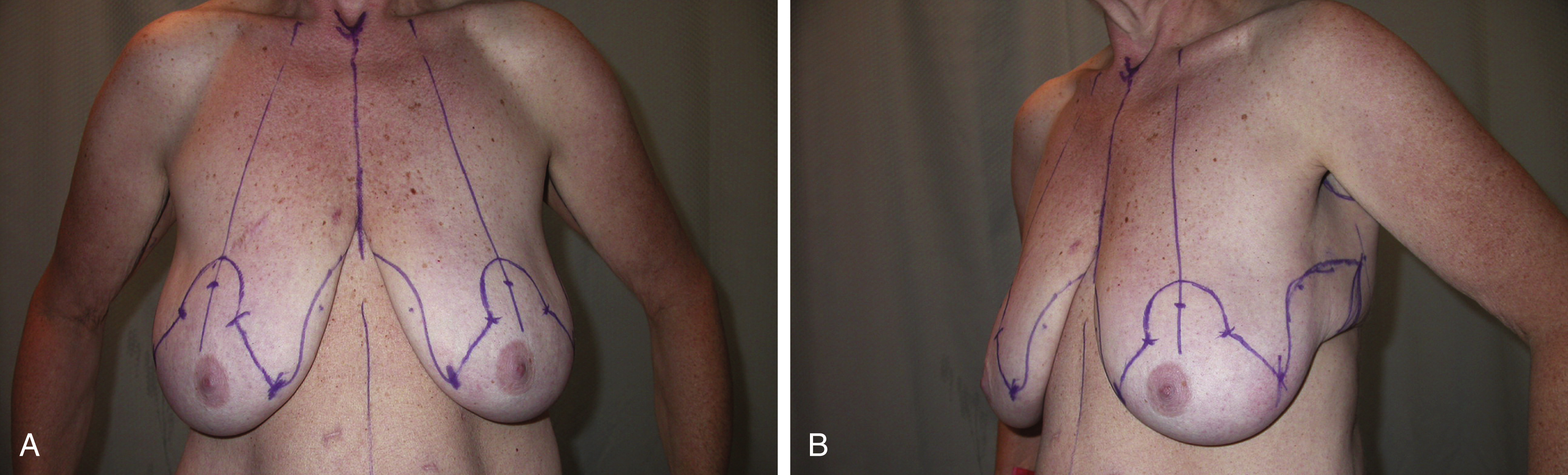
Roll of skin and fat on the lateral border of the breast that extends onto the chest wall (see Fig. 21.1A–C )
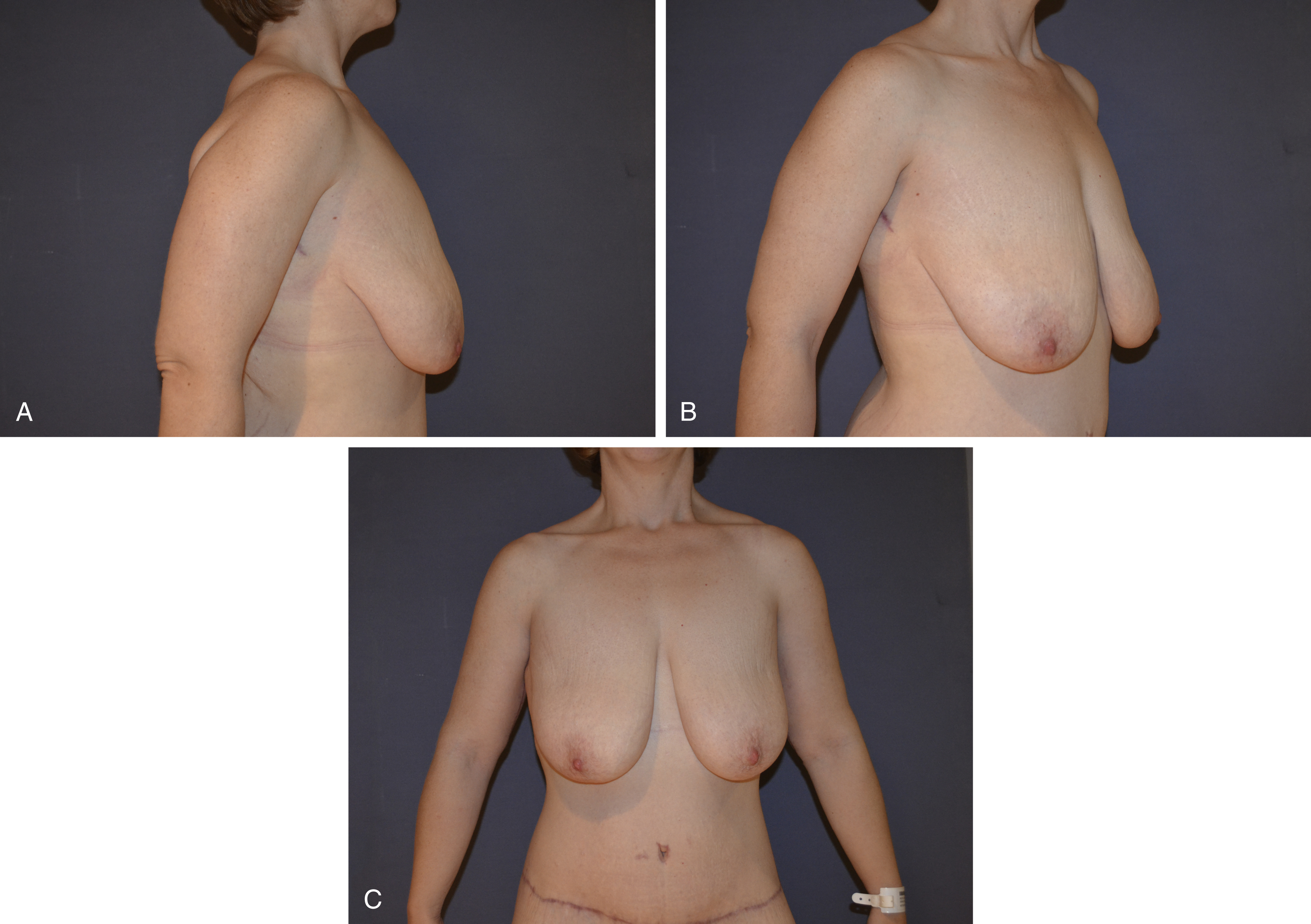
Fig. 21.1
(A–C) Typical candidate for dermal suspension and parenchymal reshaping with selective auto-augmentation technique.
The only absolute contraindications for the use of dermal suspension and parenchymal reshaping with selective auto-augmentation includes active tobacco use, because extensive flap dissection is required with this technique and smoking can compromise the blood supply to the flaps. Relative contraindications for the use of dermal suspension and parenchymal reshaping with selective auto-augmentation include the following:
- •
Prior breast scars located in areas that may compromise perfusion of the undermined tissues.
- •
Inadequate parenchymal or lateral roll volume to mobilize and build a breast mound. In the case of significant asymmetry, the smaller breast is augmented using lateral chest wall tissue, or, if not possible, a reduction of the larger breast is performed to match the contralateral side.
- •
Active intertrigo.
- •
Diffuse fibrocystic disease.
- •
Body mass index (BMI) over 35.
Preoperative Evaluations and Special Considerations
Preoperative planning is crucial when performing body contouring in patients who have lost a massive amount of weight. A detailed history should be taken, including the type of bariatric surgery; time elapsed since the bariatric surgery; and the patient’s initial and current BMI, nutritional status, diet, medical or family history of venous thromboembolic event, and smoking status. The patient should be at goal weight (preferably with a BMI under 30) with no significant fluctuations (no more than a 5-lb change per month) for the prior 3 months. This weight stabilization usually occurs 12–18 months after bariatric surgery. Patients with a higher BMI should be referred back to the weight loss specialists to provide diet and exercise programs to optimize the patient’s BMI before surgery. Patients who are current users of tobacco products should be instructed to stop 1 month before and after surgery. Patients with a positive history of smoking are routinely tested with a cotinine urine test before surgery. A thorough physical examination of the breast should be conducted not only to determine the aesthetics but also to rule out the presence of masses and scars. Surgeons should assess skin quality, parenchymal volume, NAC position, and presence and size of a lateral roll of skin and fat.
The surgeon should determine whether the native breast parenchyma and lateral roll together will provide adequate volume for a breast reshaping procedure. Patients should be adequately assessed and should undergo medical clearance. Appropriate laboratory testing should be performed before surgery. Mammography is requested in accordance with the American Cancer Society guidelines. Patients should be asked to stop all medications that interfere with platelet function 2 weeks before surgery to avoid bleeding complications. Photographs of the breasts and trunk should be taken from a wide variety of angles. Photographs are helpful to plan the markings and the surgery and to critically assess the results postoperatively. Informed consent should be obtained discussing the procedure and complications. The postoperative care should be discussed to prepare the patient on what to expect in the postoperative period. The surgical plan, risks, and benefits are reviewed again on the day of surgery to address any outstanding patient concerns. Throughout the preoperative consultation, the plastic surgeon should gauge patient goals to ensure the expectations are realistic.
Several factors should be taken into account when deciding the most appropriate procedure for breast reshaping: severity of the breast deformities, desired breast size, and surgeon’s experience and comfort level.
The goals for breast reshaping in patients with massive weight loss are as follows:
- •
Use all available breast tissue and additional adjacent autologous tissue
- •
Reshape the breast skin envelope without relying on it for support
- •
Re-establish an appropriate NAC position
- •
Restore superior pole projection
- •
Eliminate the lateral skin and fat roll
The senior author has developed and refined a surgical technique to meet these goals. The principles are based on dermal suspension and parenchymal reshaping with selective auto-augmentation, which as mentioned earlier is used for breasts that score 2 or 3 on the Pittsburgh Rating Scale. In brief, an extended Wise pattern is used to encompass the lateral skin rolls necessary for volume augmentation. The de-epithelialized Wise pattern creates a broad dermal surface area, which is plicated to precisely contour the breast shape and is suspended to the periosteum of the chest wall. This is a safe and reproducible technique that yields a youthful breast shape in a very challenging population.
Surgical Techniques
Relevant Surgical Anatomy
Understanding the normal breast topography and blood supply are key to ensure optimal results and avoid complications. Breast skin receives blood supply from the subdermal plexus, which communicates with underlying deeper vessels supplying breast parenchyma through perforators. For this reason, skin flaps should be thick enough to avoid damaging the subdermal plexus. The breast parenchyma receives a rich blood supply from multiple arterial sources: internal mammary artery, lateral thoracic artery, intercostal perforators, thoracodorsal artery, and thoracoacromial artery. The central pedicle used in the technique described later relies on perforators of the internal mammary artery from the fifth or sixth intercostal space that comes through the pectoralis muscle into the parenchyma just medial to the breast meridian. The venous system accompanies the perforator. For this reason, the pedicle should be well designed and not undermined to prevent NAC and parenchymal necrosis.
Preoperative Markings
An extended Wise pattern is drawn with a lateral extension to address lateral skin and fat roll to provide additional tissue for auto-augmentation ( Fig. 21.2 ). A new breast meridian is drawn in the center of the breast mound. This line will often not cross the medialized nipple position. The new position of the nipple is transposed over the meridian breast line using the inframammary fold (IMF) as the reference point. The superior border of the NAC is then marked 2 cm above the new nipple position. This is used as the reference point to draw a keyhole pattern with 5-cm vertical limbs. A lateral extension is then drawn from the Wise pattern to include the lateral skin and fat roll often to the posterior axillary line and beyond depending on the amount of tissue that needs to be recruited for auto-augmentation. This tissue is supplied by the lateral thoracic perforators and is rotated into the breast for auto-augmentation. The amount of lateral extension used depends entirely on the desired size and degree of asymmetry.