Fig. 7.1
Case I. (a) Preoperative performance of recurrent tongue cancer. (b) The tumor invaded the whole tongue, left mandible, left oropharynx side and pyriform sinus, epiglottis root, and left false vocal cord; the left cervical lymph node metastasis invaded the left common carotid artery and the internal jugular vein and cervical skin; there was right cervical lymph node metastasis. (c) The patient underwent resections of the whole tongue, whole throat, left mandible, left faciocervical skin and soft tissue, and left common carotid artery, dissections of the left cervical radical lymph node and right cervical functional lymph node, and trachea fistula making. (d) Design of transverse rectus abdominis myocutaneous flap (the flap was 25 cm × 10 cm in size). (e) Skin flap preparation; the transverse rectus abdominis myocutaneous flap pedicled with the inferior epigastric artery was harvested. (f) Reinforcement of the abdominal wall with tissue patch. (g) The donor site of the skin flap was closed and sutured directly. (h) The skin flap was used for defect repair during surgery; the skin and subcutaneous tissue of the skin flap were incised to be divided into two parts, one part was used to repair the hypopharynx and oral defects and another part was used to repair the cervical and facial defects. (i) Vascular anastomosis: the vascular anastomoses were performed in the right superior thyroid artery and internal jugular vein. (j) The situation when the operation was completed. (k), (l) At 2 months after surgery, the wound healed well, the skin flap healed well, the tracheostomy stoma was smooth, and the patient could take semiliquid diet
Case II
The patient, male, 47 years old, at 6 months after resection of the right oral buccal cancer in the other hospital, had right facial mass for 2 months. Physical examination: the mouth opening was limited, the postoperative scars were observed at the corner of the mouth, a nodular mass was visible on the right side of the face with red and swollen surface and obscure boundary, and the mass was fixed. MRI showed that the tumor invaded the full thickness of the right oral buccal area and right maxilla and mandible. Pathological diagnosis: highly and moderately differentiated squamous cell carcinoma. The patient underwent a wide range of resection of the right buccal area and right prostatectomy, resection of the right maxilla and mandible, and the repair with free thigh anterolateral myocutaneous flap under general anesthesia (Fig. 7.2).
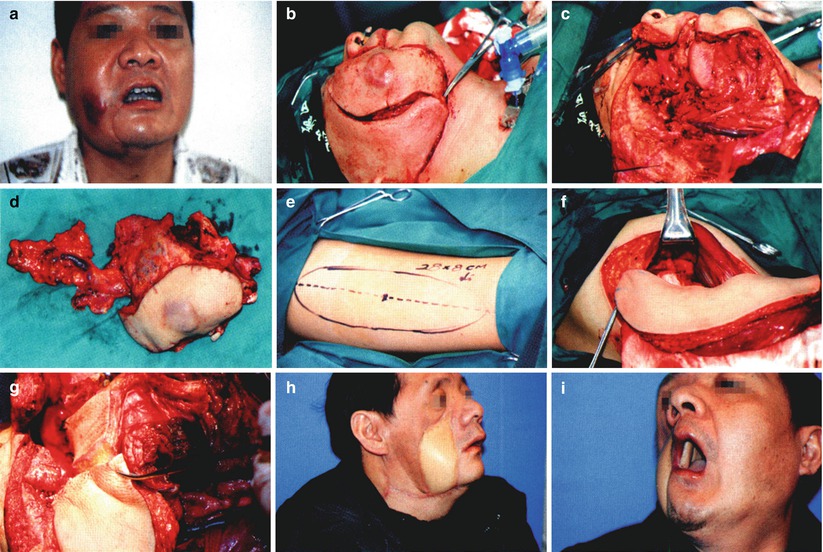
Fig. 7.2
Case II. (a). Before surgery. (b) The patient underwent a wide range of resection of the right buccal area and right maxilla and mandible. (c) The huge perforating defect in the right buccal area after surgery and the defects in the right maxilla and mandible, and the defect reached up to the lateral skull base. (d) The specimen was removed. (e) The right anterolateral thigh skin flap was designed as 28 cm × 8 cm in size. (f) The anterolateral thigh cutaneous flap was harvested and transplanted. (g) After the anterolateral thigh skin flap was partially incised and folded, one part was used to repair the defects in the oral buccal area, right maxilla, and lateral skull base, and another part was used to repair the defects in the facial buccal area. (h), (i) At 6 months after surgery, the wound healed well; the skin flaps healed well; the degree of mouth opening was acceptable; the patient spoke clearly and could take the semiliquid diet
Case III
The patient, male, 51 years old, had a mass in the left lower gingiva for 6 months and had left facial redness and swelling for 1 week. Physical examination: the size of the left facial redness and swelling was 3 cm × 2 cm, and the subcutaneous hard mass was palpable and fixed. The degree of mouth opening was acceptable. A cauliflower-shaped mass was located at the left lower buccal gingival side, and it had invaded the left oral buccal area. Pathological diagnosis: highly differentiated squamous cell carcinoma. The patient underwent radical resection of left gingival cancer, full-thickness resection of the left buccal area, and the repair with the deep inferior epigastric perforator skin flap under general anesthesia (Fig. 7.3).
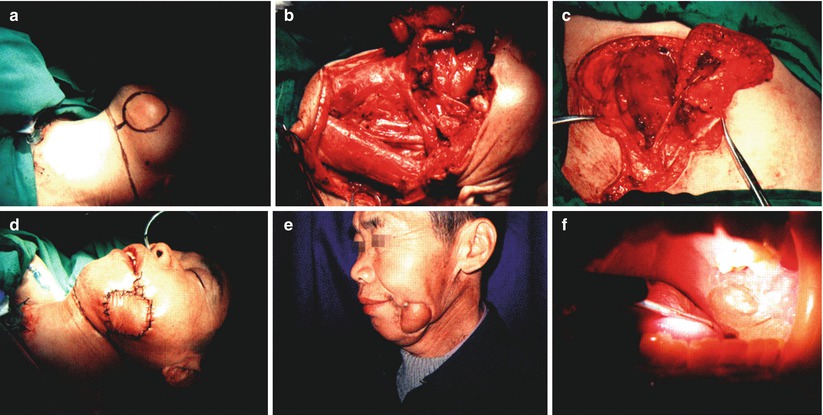
Fig. 7.3
Case III. (a) The mass in the left lower gingiva invaded the left mandible and the oral buccal area, and the facial skin was invaded. (b) The patient underwent full-thickness resection of the left buccal area, partial resection of the left body of mandible, and dissection of the left cervical functional lymph node. (c) The perforator skin flap pedicled with the deep inferior epigastric artery was harvested. (d) The middle part of the skin flap was partially removed, the skin flap was folded, a part was used to repair the oral buccal defect, and another part was used to repair the facial buccal defect. (e), (f) At 3 years after surgery, the skin flaps healed well, the mouth opening seemed fine, there was no recurrence, and the intraoral skin flap was mucosalized
2.2 The Repair with a Free Skin Flap and a Pedicled Skin Flap
2.2.1 The Skin Flaps for Selection
The perforating defects in the upper part of the face and the lip-cheek region can be repaired with the forehead skin flap (pedicled axial pattern skin flap) plus free forearm or scapular skin flap, of which the former is mostly used as the lining and the latter is mostly used as the outer covering. The perforating defects in the lower part of the face and the upper part of the neck can be repaired with pedicled pectoralis major myocutaneous flap plus the free forearm skin flap, and sometimes they can also be repaired with cervical skin flap (or superior trapezius myocutaneous flap) plus free scapular skin flap. The patients with perforating defects and mandibular defects can be repaired with fibula-peroneal artery perforator flap, the fibula flap is used to repair the mandibular defect, the peroneal artery perforator flap is used to repair the defects in the oral buccal and gingival area, and the facial buccal defect is repaired using the ortho-position skin flap or another free skin flap.
2.2.2 Typical Case
Case IV
The patient, male, 49 years old, had a mass in the right lower gingiva for 3 months. Physical examination: the right side of the face was uplifted, and a subcutaneous hard mass was palpable with poor activity. The degree of mouth opening was acceptable. There was a cauliflower-shaped mass in the buccal side of the right lower gingiva and the vestibular groove. The loosening of fourth and fifth lower right teeth reached grade 3. CT showed that the right lower gingival mass invaded the mandible and cheek muscle, and the subcutaneous fat space disappeared. Pathology: highly and moderately differentiated squamous cell carcinoma. The patient underwent radical resection of right gingival cancer, full-thickness resection of the right buccal area, and repair with the free fibular skin flap and the submental ortho-position skin flap under general anesthesia (Fig. 7.4).
Fig. 7.4
Case IV. (a), (b) Preoperative appearance. (c) Incision design; it was noted to preserve the integrity of the corner of the mouth, incise the lower lip instead of the corner of the mouth, and design the submental platysma myocutaneous flap with the pedicle in the posterior part. (d) Radical resection of the right gingival cancer; the right facial buccal area of about 4 cm × 4 cm was removed, and the right oral buccal area and the mandibular body were removed, and then the perforating defect in the right buccal area was formed after surgery. (e), (f) Radical resection specimen. (g), (h) The fibula-peroneal artery perforator flap in the left calf was harvested. (i), (j) The fibula flap after shaping was used to repair the mandibular defect, and titanium plate fixation was performed, the peroneal artery perforator flaps was used to repair the oral buccal and gingival defects, and the submental platysma myocutaneous flap was transferred to repair the facial buccal defect. (k), (l) The stitches were taken out at 8 days after surgery, the wound healed well, the skin flaps healed well, the degree of mouth opening was acceptable, there was still swelling in the faciocervical area, and the speaking was clear. (m), (n) At 3 months after surgery, the degree of mouth opening was 4 cm; the intraoral skin flap healed well; a small amount of hair growth was observed; the appearance was satisfactory; the speaking and eating seemed fine
2.3 The Repair with Transplantation of Double Free Tissue Flaps
2.3.1 The Skin Flaps for Selection
The transplantation of double free tissue flaps is commonly used in the repair of the oral perforating defect combined with complex defects of other tissues, for example, combined with the defects in the upper and lower jawbones and the defect in the nose. It is often very difficult to repair this kind of complex defect satisfactorily with a folded skin flap, which is often repaired with the transplantation of double free tissue flaps. To some extent, the transplantation of double free tissue flaps means that four blood vessels must be anastomosed at least, that is, two arteries and two veins. There is no doubt that in order to ensure the success of the surgery, there is a higher requirement on the technique of vascular anastomosis. In clinics, the fibular skin flap plus the anterolateral thigh skin flap or the latissimus dorsi myocutaneous flap plus the forearm skin flap is mostly selected. This method is particularly suitable for the defect after combined radical resection of cranio-jaw. It can not only fill the dead space and protect the brain tissue but can also form the new palate and repair the facial defects. This approach requires two arteries and two veins for anastomosis. If only one artery and one vein are available for the patients with insufficient supplying vessels in the receptor site, the forearm skin flap can be selected as the bridge skin flap in the middle part, the arteries and veins at one end of the forearm skin flap are anastomosed with those of another forearm skin flap or other myocutaneous flaps, and such skin flaps can also be called as the tandem skin flaps (Fig. 7.5). Among numerous skin flaps, it is most appropriate to take the forearm skin flap as the bridge skin flap (or middle skin flap) because it is an arterial pattern skin flap, and the diameters of both ends of the blood vessel are similar. In addition, the supplying vessel of the anterolateral thigh skin flap such as the descending branch of the femoral circumflex artery and the supplying vessel of fibula flap such as the distal end of the peroneal artery can also be used as the bridge blood vessels. The diameters of the ends of the blood vessels of most skin flap are very thin, and they are difficult to be taken as the blood vessels for vascular anastomosis.
Fig. 7.5
Schematic diagram of tandem skin flaps
2.3.2 Typical Case
Case V
The patient, female, 67 years old, had a mass on the right side of the nose and face combined with ulceration for 3 years. Physical examination: the ulcers are visible on the right side of the nose, nasal floor, nasal columella, facial buccal area, upper lip, and vermilion; the ulcer surfaces were covered by dry scabs, the margin uplifts were irregular, and the boundaries were not clear. Pathological diagnosis: highly differentiated squamous cell carcinoma. The patient underwent extensive resection of the right side of the nose, facial buccal area, upper lip cancer, free forearm skin flap, and repair with free auricle compound tissue flap under the general anesthesia (Fig. 7.6).

Fig. 7.6
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
 Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors




Case V. (a) The surface appearances of skin cancer involving the right upper lip, facial buccal area, nosewing, nasal tip, nasal columella, and nasal floor; the right nostril was significantly reduced. (b) The facial skin cancer was extensively removed, which led to the perforating defects in the upper lip and right buccal area and the defects in the right nosewing part of nasal septum, nasal columella, nasal tip, and bilateral soft triangles; the right nasal bone and part of maxilla at the outer side of the piriform aperture were partially removed, and the maxillary sinus was not opened. (c) The forearm skin flap was designed according to the defects in the upper lip and buccal area; three parts such as the defect in the intraoral part of the upper lip, the defect in nasal floor, and the defect in the right buccal area were repaired respectively. (d) The forearm skin flap was folded to repair the defects in the upper lip, nasal floor, and buccal area; the vascular pedicle was passed through the subcutaneous tunnel to reach the neck and was anastomosed with the facial artery and vein. (e) The auricle compound tissue flap was designed according to the nasal defect. (f) The auricle compound tissue flap pedicled with superficial temporal artery and vein was harvested. (g) The auricle compound tissue flap was used to repair defects in the nosewing, nasal columella, nasal tip, and soft triangle of upper lip; the supplying vessels of the skin flap such as the superficial temporal artery and vein were anastomosed with the supplying vessels of the forearm skin flap such as the distal ends of radial artery and vein, and the nostrils were supported with plastic tubes for shaping. (h) The postauricular flap was used to repair the defect after harvesting of the auricle compound tissue flap; the donor site of postauricular flap was directly closed and sutured. (i), (j) The reexamination was carried out at 8 months after surgery; the skin flap healed well; the appearances of the nose, upper lip, and facial cheek were basically satisfied; the degree of mouth opening was acceptable; the eating was normal; the speech was clear; the nasal ventilation seemed fine; the appearance of donor site of skin flap in the right ear auricle was satisfactory
Related posts:
Microcirculation Model for Invasive Animal Monitoring
Composite Osseomusculocutaneous Thymus Allotransplantation Model
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Tissue Engineering and Oncological Surgery
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
