Fig. 16.1
Different types of chest wall tumors may cause complex chest wall defects. (a) Cauliflower-like tumor. (b) Ulcerative type tumor. (c) Expansive type tumor. (d) Sternal defect tumor
Therefore, the chest wall defect repair should aim to restore the continuity of the chest wall structure to protect the thoracic organs, maintain normal respiratory and circulatory functions, and obtain a good shape at the same time.
1.1 Resection of a Chest Wall Tumor
Before deciding to carry out the chest wall mass resection, it is required to confirm the diagnosis to exclude chest wall tuberculosis, multiple myeloma, and lymphoma. As long as the general conditions in the patients are good, and there is no distant metastasis, all benign and malignant chest wall tumors should be surgically removed. The metastatic chest wall tumors, including the direct chest wall invasion of malignant tumors of intrathoracic internal organs, as long as the primary focus has no recurrence, or has been removed completely, the surgeon should strive to resect the metastatic chest wall tumor, to achieve the purpose of curing or prolonging the life and reducing the pain. For radiosensitive malignant tumors such as lymphoma and Ewing’s sarcoma, most scholars believe that the use of radiotherapy + surgery has a more satisfactory curative effect. The patients with multiple myeloma should be treated mainly with chemotherapy and supplemented by radiotherapy, and the patients with solitary single myeloma without systemic symptoms may undergo resection and receive postoperative radiotherapy and chemotherapy. The patients with breast cancer and chest wall invasion of lung cancer should receive postoperative chemotherapy and radiotherapy according to the principles of treatments of breast cancer and lung cancer. The osteosarcoma patients should receive postoperative chemotherapy. For various rare malignant bone tumors in ribs and sternum including single well-circumscribed tumor, such as malignant osteoblastoma, malignant eosinophilic granuloma, and malignant giant cell tumor, the patients should be treated by surgery as far as possible. Some tumors should receive radiotherapy after chemotherapy at first, and then they can be resected when the tumor bodies are reduced.
The surgical method should be selected according to the growing location, size, and pathological type of the chest wall tumor. The patients with smaller benign chest wall tumors just need to undergo local tumor resection, and without the need for the repair with artificial materials; but the patients with large area chest wall defect after tumor resection need to undergo chest wall reconstruction with artificial materials. For chest wall tumors which are primary or metastatic malignant or have malignant biological behaviors, if involving the ribs, the tumor including a normal rib respectively above and below the lesion, and all ribs, muscles, and soft tissue attached by the tumor, parietal pleura, and regional lymph nodes should be removed, its front and rear surgical margins should also be kept a distance of 3–5 cm away from the tumor margins, and the samples are taken from the margins (top, bottom, left, and right) and sent for rapid pathological frozen section examination. If the tumor has invaded the lungs, partial lung resection or pulmonary lobectomy should be carried out simultaneously. For malignant tumors which directly invade the chest wall (such as breast cancer and lung cancer), en bloc resection of the chest wall including the primary focuses should be performed.
Sometimes, the chest wall cancer patients have undergone surgical treatments for many times when they visit the hospital, with repeated recurrence, the tumor body is huge, or the ulcer ruptures repeatedly, accompanied by the stench or distant metastases; it is required to confirm the nature of the treatment before surgery, whether it is radical treatment or palliative treatment.
If the tumor has a biological characteristic that is prone to local recurrence, but is not prone to distant metastasis or has no distant metastasis, it is needed to emphasize the thoroughness of tumor resection and provide opportunity of radical cure to the patient. If the patient has a distant metastasis at the same time, the treatment is mainly aimed at treating the burst bleeding and stench of the ulcer, removing the local disease and improving quality of life, or creating the conditions for postoperative chemotherapy and radiotherapy (only suitable for chemotherapy-sensitive tumors). It belongs to the palliative treatment. It is noteworthy that even the palliative treatment should also emphasize the thoroughness of local resection or the incision that is located within the tumor body; it is difficult to heal completely.
It is required to confirm the nature of the local ulcer in patients receiving radiotherapy; whether it is radiation-induced ulceration or tumor recurrence, it requires biopsy or intraoperative frozen section examination. If it is radiation-induced ulceration, some patients may retain the support structure such as ribs, and the remaining radioactive damage can be biologically removed by the covering tissues with good blood supply; if it is tumor recurrence, it is required to carry out complete resection. For some patients with breast cancers which are mainly presented as ulcers, the neoadjuvant chemotherapy can be carried out to reduce the range of the tumor body, and then the surgical treatment is performed.
1.2 Classification of Chest Wall Defects
1.2.1 Classification According to the Extents of the Defects
The chest wall defects can be divided into the simple skin and soft tissue defects, the defects in chest wall support structure such as ribs and sternum, and the full-thickness chest wall defect according to the extents of the defects. The classification according to the extents of the defects may provide guidance for the repair of the chest wall layer by layer.
1.2.2 Classification According to the Positions of the Defects
The chest wall defects can be divided into sternal defect, anterior chest wall defect, lateral chest wall defect, and posterior chest wall defect according to the positions of the defects. The classification according to the positions of the defects can offer help in selection of skin flaps for repair. It is noteworthy that the transverse rectus abdominis myocutaneous (TRAM) flap often can’t reach the upper end of the chest wall, and the forced application will result in distal flap necrosis.
1.2.3 Partition of Chest Wall Defect
The partition of chest wall defect generally refers to the partition of anterior chest wall. For selection of therapeutic regimen, the anterior chest wall can be divided into eight regions. The upper boundary of the anterior chest wall is the clavicle, the lower boundary is the margin of the hypochondrium, the lateral sides are bilateral axillary lines, and the anterior chest wall is divided into three parts such as left, middle, and right parts through the midclavicular lines; then through the horizontal line at the lower boundary of the third rib and the xiphoid process level, the chest wall is divided into three parts, such as upper, middle, and lower parts, so that the chest wall is divided into eight regions (Fig. 16.2).
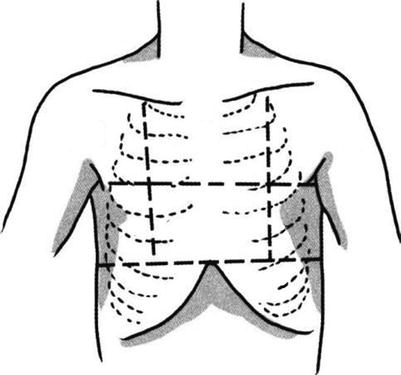
Fig. 16.2
Partition of anterior chest wall 1, 4, and 7 are the right region; 3, 6, and 8 are the left region; and 2 and 5 are the central region
1.3 The Principles for Repair of Chest Wall Defect
In principle, the appropriate method should be selected for chest wall repair and reconstruction according to the range (size), position, and degree of the chest wall defect caused by surgery [6–9].
1.3.1 Objectives of Chest Wall Reconstruction
- 1.
To completely close the thoracic cavity, maintain the integrity of the thoracic cavity and maintain negative intrathoracic pressure.
- 2.
To protect vital organs such as the heart, lungs, and mediastinum, try to maintain the original shape and beauty of the thorax.
1.3.2 Key Points of the Chest Wall Reconstruction
- 1.
Various materials are used to reconstruct the rigid chest wall, in order to restore the ruggedness and stability of the chest wall.
- 2.
The soft tissue and skin are used to cover the rigid chest wall to keep the tightness of the chest wall.
1.3.3 The Surgical Plan Is Determined According to Defected Tissue in the Chest Wall
- 1.
The pleural defects mostly do not require repair, the pleural defect is repaired through the crawling growth of the pleura after repair of chest wall, or the pseudomembrane is formed to close the pleural cavity. The pleural cavity can be closed through fascia transplantation under very rare circumstances.
- 2.
The chest support structure can be repaired through cross-transplantation of ribs, or selectively using titanium, titanium mesh, Medpor bracket, Terylene membrane and bone cement, etc., so as to maintain the stability of the chest wall to prevent paradoxical breathing. Usually it does not require repair when less than three ribs are removed, and it is required to repair the support structures when more than four ribs or sternum are removed. Currently, the titanium mesh and Terylene membranes are most commonly used for repair of the support tissue of the chest wall, of which the titanium mesh not only has a certain support strength, but also has a certain activity, and is used widely in recent years. When used, the titanium mesh is bent into the thoracic curvature and is fixed onto the ribs and sternum with 3–5 mm titanium screws.
- 3.
The repair of soft tissue such as the skin should take into account the etiologic factors of the chest wall defect; the invasive tumors often cause deep and widespread defects; the blood supply of the area surrounding the radiation damage is often poor, which often results in poor wound healing. According to the size of the defect, the local or ortho-position skin flap can be selectively used for repair. The commonly used flaps include the pectoralis major myocutaneous flap, latissimus dorsi myocutaneous flap, transverse rectus abdominis myocutaneous flap, and omental flap. It is worth noting that, although the microsurgical technology has matured, there are more available tissue flaps in the thoracoabdominal wall, the technical requirements for microscopic free skin flap transplantation with vascular anastomosis are high, and the clinical application is less. In addition, since the presence of involuntary movements such as breathing in the chest, and compared to other sites, the skin flap has a certain shearing force, it is easy to form effusion, the drainage tube should be placed for a long time and should not be taken out in a hurry even in the case of small drainage volume, and it should be placed for 3–5 days.
1.3.4 The Surgical Plan Is Determined According to the Partition of Chest Wall Defect
- 1.
Repair of chest wall soft tissue defects: Due to different ranges of chest wall soft tissue defects, their repair methods are different. The repair methods of region 1, 4, and 7 are the same as that of region 3, 6, and 8, the local rotation flap is used for repair, the skin flap donor site is repaired with skin transplantation, or the vascularized latissimus dorsi myocutaneous flap transplantation is used for repair. For the chest wall soft tissue defect in single region such as region 4 or 6, when the defect range does not reach the midline area of the bone, the chest rotation skin flap is often selectively used for repair, and the skin flap donor site is repaired with skin transplantation. The soft tissue defect in region 2 or 5 is repaired with unilateral pectoralis major myocutaneous flap transplantation, and the donor site is repaired with free skin transplantation. Region 1 and 3 defects combined with region 2 and 5 defects are repaired with chest rotation flaps at the healthy side and the affected side, and the donor sites are repaired with skin transplantation. In the bone defect in the central region of the chest wall (region 2 and 5), or when there are lateral region defects (region 1, 4, 7, 3, 6, and 8) combined with partial bone defect in region 2 and 5, their repair methods can adopt the sandwich-type chest wall prosthesis made by double layer polyester mesh plus bone cement or the titanium mesh and the pectoralis major myocutaneous flap transplantation, or the pectoralis major myocutaneous flap plus latissimus dorsi myocutaneous flap transplantation, or two local rotation flaps are used for repair; the female patients can also use the breast transfer for repair (relatively simple), or the transverse rectus abdominis myocutaneous flap (TRAM flap) and inferior epigastric artery perforator flap are used for repair.
- 2.
Repair of chest wall bone defect: For the chest wall bone defects in different sites, the emphasis points of the chest wall reconstruction are also different.
- (1)
The defects in sternal region, namely, region 2 and 5: After the occurrence of the sternum and bilateral rib cartilage defects, the thoracic integrity and stability are damaged to a greater extent, then the heart and great vessels behind it are also vulnerable to external force influence, and therefore it is required to carry out chest wall reconstruction and focus on the reconstruction of its bony framework. The authors believe that the titanium mesh or the sandwich-type chest wall prosthesis consisting of Prolene mesh + bone cement + Prolene mesh is used to repair the bony framework, and then the pectoralis major muscle flap or latissimus dorsi muscle flap is used for coverage. These ruggedness, stability and shaping, and clipping of this method are satisfactory. But attentions must be paid to avoid the exothermic effect of the bone cement in the process of shaping damages to the adjacent tissues or organs.
- (2)
The defects in the upper chest wall, namely, region 1 and 3: Because the upper chest wall, namely, region 1 and 3, is covered by thicker tissues such as the scapula, latissimus dorsi muscle, and pectoralis major and minor muscles, if the defect is smaller, it can be directly sutured or covered by local muscle flap. Especially for the chest wall defect locating in the scapula area, the defect can be retained without chest wall reconstruction. But for the patients with defect area larger than 6 × 6 cm, continuous removal of more than three ribs and intercostal tissues, the chest wall reconstruction should be carried out; it is recommended that Prolene mesh is used to repair the defect.
- (3)
The defects in the middle and lower chest wall, namely, region 4, 6, 7, and 8: Because the middle and lower chest wall is not covered by thicker tissues, if it cannot be directly sutured to carry out the chest wall reconstruction, the diaphragm or Prolene mesh can be selectively used for reconstruction; if the diaphragm cannot be used for reconstruction, the Prolene mesh is used to repair the chest wall defect, and its surface is covered with latissimus dorsi muscle flap or TRAM flap.
- (1)
- 3.
Repair of full-thickness chest wall defects: If the defects in the skin, muscles, and bones of the chest wall are greater, they often need to be repaired by combined use of artificial materials and autologous tissue materials, the artificial materials are used to repair the bony structure of the chest wall, and the autologous tissue materials are used to repair the local skin and muscle defects. The authors advocate that it is better to use the artificial materials such as Prolene mesh or titanium mesh or sandwich method of Prolene mesh and bone cement to repair the chest wall defects, the skin flap and artificial materials should be separated with the muscle flap or greater omentum, which can improve the surgical successful rate. The adjacent myocutaneous flap or latissimus dorsi myocutaneous flap or TRAM flap is used as the myocutaneous flap.
During chest wall reconstruction, attention must be paid to placing drainage tubes between layers of materials to timely drain the exudate and eliminate the dead space, so that various layers of tissues can timely cling close and heal early. If there is fluid retention, the secondary infection will easily occur, resulting in failure.
1.4 The Commonly Used Repair Method
1.4.1 Local Skin Flap
The wounds after resection of tumor in the resection can be repaired with local skin flap; the design of the skin flap is to contain blood vessels as far as possible, such as lateral chest wall flap and intercostal flap; and when the random pattern skin flap is used, attention should be paid to the length-to-width ratio of the skin flap.
- 1.
Case I After chest wall tumor resection, if the support structures of the chest wall are intact, the random pattern skin flap is used for repair (Fig. 16.3).

Fig. 16.3
Case I. (a) The wound after chest wall tumor resection. (b) Skin flap design. (c) After repairing and suturing the wound with rotation of random pattern skin flap
- 2.
Case II Giant chest wall tumor. The patient underwent multiple surgeries in other hospitals and had tumor recurrence involving the sternum, and the abdominal skin flap is used for defect repair after extensive resection (Fig. 16.4).
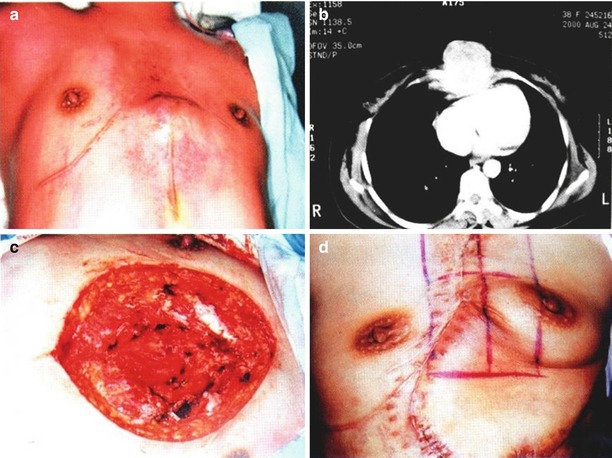
Fig. 16.4
Case II. (a) Giant chest wall tumor before surgery. (b) Preoperative chest CT showed that the tumor involved the sternum. (c) The wound after extensive resection of the tumor. (d) After repair of the wound with rotation of abdominal skin flap
1.4.2 Latissimus Dorsi Myocutaneous Flap
The latissimus dorsi muscle is a flat and triangular muscle with its flat and wide aponeurosis starting from the lower six thoracic vertebras, all lumbar vertebras, sacral vertebras, supraspinous ligament, and posterior iliac crest. The muscle fibers are divided into two parts, such as the upper horizontal part and the inferior oblique part, and aggregate toward the upper outer side and end at the spine of the lesser tubercle of the humerus. The latissimus dorsi myocutaneous flap has a blood supply from multiple sources, including the thoracodorsal artery, intercostal artery, and lumbar artery as well as their accompanying veins, of which the thoracodorsal vessels are the main nutrient vessels. The thoracodorsal artery is the terminal branch of the subscapular artery. The subscapular artery is given off from the third section of the axillary artery and passes through the armpit to run downward, subsequently gives off the circumflex scapular artery, and, finally, becomes the thoracodorsal artery. The thoracodorsal artery and vein run under the myolemma at the inner surface of the latissimus dorsi muscle; after entering into the muscle, they are divided into the lateral branch and the medial branch; the lateral branch runs downward at 2–3 cm behind the anterior margin of the muscle bell, and the medial branch is parallel to upper margin of the muscle and run inward. The motor nerve of the latissimus dorsi muscle is the thoracodorsal nerve, which accompanies with the blood vessels to enter into the muscle.
The latissimus dorsi myocutaneous flap pedicled with the thoracodorsal artery, and its rotational arc can reach up to the head and neck, shoulder, upper limb, and ipsilateral chest. It has a wide range of clinical applications, is one of skin flaps with most extensive range and most versatile functions in the body which are available for free transplantation or pedicled transplantation, and is commonly used for repair of a large area of skin and tissue defects and the defects which are associated with muscle defects and require carrying out functional reconstruction and the breast reconstruction.
An oblique line which is parallel to the anterior margin of the latissimus dorsi muscle is drawn at 2 cm behind the anterior margin of the latissimus dorsi muscle, and it is the body surface projection of the thoracodorsal vessels. The myocutaneous flap is designed along the body surface projection line. The transplanting method and harvesting range for latissimus dorsi myocutaneous flap are determined according to the wound status in the donor site. The more commonly used design methods include the latissimus dorsi myocutaneous flap which takes the skin on the waist and back as the main donor site and the transverse latissimus dorsi myocutaneous flap which takes the upper half back of the transverse skin as the main donor site. When the surgery is performed, the patient takes the lateral position or hemilateral position, the skin tissue is incised for the armpit along the anterior margin of the latissimus dorsi muscle, the anterior margin of the latissimus dorsi muscle is exposed, the clearance behind the muscle is bluntly dissected, and the thoracodorsal artery, vein, and nerve can be exposed. The blunt dissection is continuously performed toward the distal end, the travel path of the neurovascular bundle in muscle is determined, the end point of the muscle is cut off, the desired width and length are harvested, and the latissimus dorsi myocutaneous flap is formed to repair the wound. The donor site is directly sutured or treated with skin transplantation.
- 1.
Case III The patient, female, 56 years old, had left chest wall radiation-induced ulceration caused by the radiotherapy after bilateral breast cancer surgery, and the ribs were exposed; after the diseased tissues were removed, the titanium mesh was used to repair the ribs, and the latissimus dorsi myocutaneous flap was used to repair the soft tissue defect (Fig. 16.5).
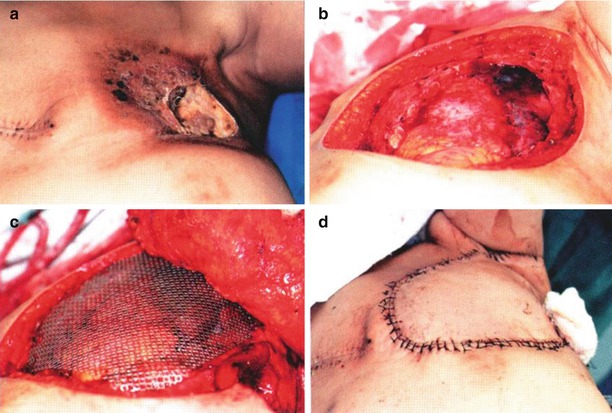
Fig. 16.5
Case III. (a) Left chest wall radiation-induced ulceration caused by the radiotherapy after bilateral breast cancer surgery, and the ribs were exposed. (b) The wound after resection of diseased tissue. (c) The titanium mesh was used to repair the ribs. (d) After repair of soft tissue repair defects with latissimus dorsi myocutaneous flap
- 2.
Case IV The patient, female, 42 years old, had left chest wall radiation-induced ulceration caused by the radiotherapy after left breast cancer surgery, and the ribs were exposed and necrotized; after resection of diseased tissue, the titanium mesh was used to repair the ribs, and the latissimus dorsi myocutaneous flap was used to repair the soft tissue repair defect (Fig. 16.6).
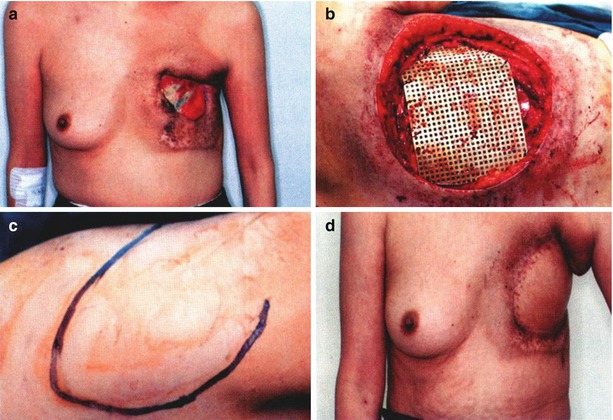
Fig. 16.6
Case IV. (a) The radiation-induced ulceration caused by the radiotherapy after left breast cancer surgery, and the ribs were exposed and necrotized. (b) After resection of diseased tissue, the titanium mesh was used to repair the ribs. (c) Design of the latissimus dorsi myocutaneous flap. (d) The latissimus dorsi myocutaneous flap were used to repair the soft tissue repair defects
1.4.3 Rectus Abdominis Myocutaneous Flap
According to the need of the repair, the rectus abdominis myocutaneous flap can be designed as longitudinal rectus abdominis myocutaneous flap and transverse rectus abdominis myocutaneous flap. For repair of the chest wall defects, the longitudinal rectus abdominis myocutaneous flap is more commonly used, and it is required to confirm that the internal thoracic vessels are not damaged before surgery; otherwise it is needed to selectively use other skin flaps for repair. The lower abdominal TRAM flap is mostly used for breast reconstruction.
The rectus abdominis muscle is located on both sides of the abdominal midline and is separated by the abdominal white line. It starts from the pubic symphysis and pubic bone, travels upward, and ends at the front of the sternum xiphoid periosteum and the fifth to seventh costal cartilages. The whole length of rectus abdominis muscle is divided into several muscle bellies by three to four transverse tendinous intersections; the tendinous intersections are closely integrated with the anterior sheath of the rectus abdominis muscle. The blood supply of the rectus abdominis myocutaneous flap is mainly from the superior and inferior epigastric arteries; the superior epigastric artery is a direct continuation of the internal thoracic artery, and it passes through the sternocostal triangle downward to reach the rectus abdominis muscle, penetrates into the muscle from behind the rectus abdominis muscle, and is anastomosed with the branch of the inferior epigastric artery near the navel; the inferior epigastric artery is given off from the medial wall of the external iliac artery below the inguinal ligament, at the junction of the inner two fifth and the outer three fifth of the inguinal ligament, and it runs obliquely toward the upper inner side behind the transversalis fascia, after crossing the lateral margin of the rectus abdominis muscle; it goes up to enter into the rectus abdominis muscle from behind the muscle and forms into the terminal branch near the area beside the navel. In the process of running within the muscle, both the superior and inferior epigastric arteries give off myocutaneous perforators to feed the skin tissue on the surface and are anastomosed respectively with the branches of lateral perforators of the posterior intercostal arteries, the anterior cutaneous branches of lumbar arteries, superficial epigastric artery, and superficial iliac circumflex artery. The rectus abdominis muscle is subject to control of the lower six pairs of intercostal nerves.
When the longitudinal rectus abdominis myocutaneous flap is designed, the myocutaneous flap ranges up to the xiphoid process and down to the site above the pubic symphysis. The medial side is the abdominal midline, and the lateral side can exceed the lateral margin of rectus abdominis muscle. The skin tissue, fascia, and the anterior layer of anterior sheath of the rectus abdominis muscle are incised layer by layer. When the superior epigastric artery is taken as the pedicle, the rectus abdominis muscle is transversely cut off at the distal end of the myocutaneous flap, and the inferior epigastric artery and vein are ligated and severed; the dissection is performed at the deep surface of the rectus abdominis muscle to the pedicle of the xiphoid myocutaneous flap, and the pedicle of skin should have enough length to facilitate rotation. The navel is retained in situ. The incised anterior sheath of the rectus abdominis muscle is sutured, and the abdominal donor site is closed and sutured (Fig. 16.7). If the required tissue volume is large, the TRAM flap in the lower abdomen can be used.
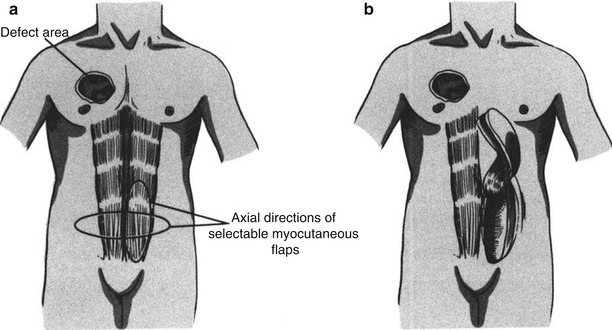
Fig. 16.7
Schematic diagram of repair of the chest wall defect with longitudinal transverse rectus abdominis myocutaneous flap. (a) The myocutaneous flap ranges up to the xiphoid process and down to the site above the pubic symphysis. The medial side is the abdominal midline, and the lateral side can exceed the lateral margin of rectus abdominis muscle. (b) When the superior epigastric artery is taken as the pedicle, the rectus abdominis muscle is transversely cut off at distal end of the myocutaneous flap, the dissection is performed at the deep surface of the rectus abdominis muscle to the pedicle of the xiphoid myocutaneous flap, the pedicle of skin should be easy to rotate, and the navel is retained in situ
- 1.
Case V The patient, female, 48 years old, had right advanced breast cancer, with locally recurrent ulceration and bleeding, accompanied by the stench. After the removal of the tumor from the rib surface, the defect was repaired with the contralateral longitudinal transverse rectus abdominis myocutaneous flap, and the postoperative chemotherapy was carried out, which significantly improved the quality of life of the patient (Fig. 16.8).
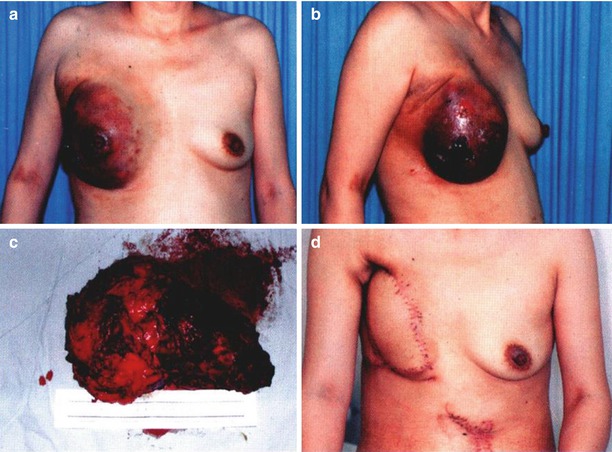
Fig. 16.8
Case V. (a, b) Before resection of right advanced breast cancer, there was local ulceration and bleeding. (c) The resected tumor tissue. (d) After repair with the contralateral longitudinal transverse rectus abdominis myocutaneous flap
- 2.
Case VI The patient, female, had left chest wall tumor. There was left chest wall defect after the removal of the chest wall tumor; through skin flap design, the transverse rectus abdominis myocutaneous flap was used to repair the chest wall defect, and then the wound was sutured (Fig. 16.9).
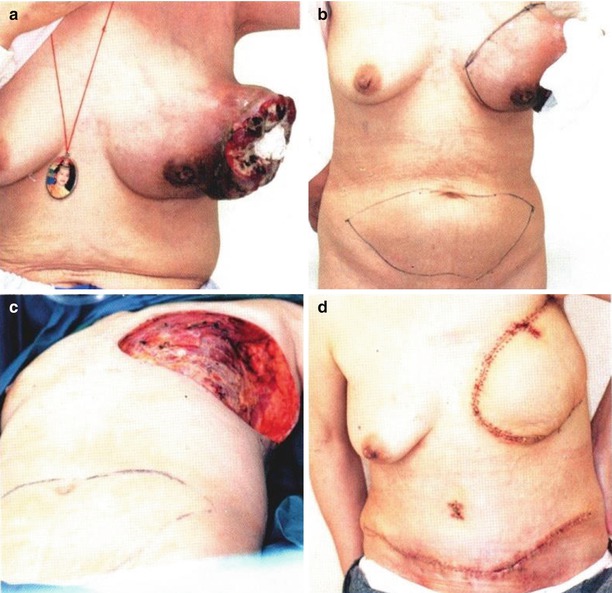
Fig. 16.9
Case VI. (a) Before left chest wall tumor surgery. (b) Skin flap design. (c) The chest wall defect after resection of the chest wall tumor. (d) The defect after resection of the chest wall tumor was repaired with TRAM flap in the lower abdomen
- 3.
Case VII The patient, female, had right breast cancer recurrence after mastectomy, with local ulcers after radiotherapy and chemotherapy. The chest wall defect was repaired after tumor resection with the combined use of Prolene mesh and TRAM flap, and the abdominal donor site was repaired and reinforced with Prolene mesh (Fig. 16.10).
Fig. 16.10
Case VII. (a) Recurrence after resection of right breast cancer, the performance of local ulceration after radiotherapy and chemotherapy. (b) The chest defect wound after tumor resection. (c) The resected tumor tissue included five ribs and cartilages. (d) Prolene mesh was used to repair the chest wall defect. (e) The TRAM flap was dissected. (f) The dissection of TRAM flap was completed. (g) The TRAM flap with preservation of unilateral inferior epigastric artery and vein. (h) Prolene mesh was used to repair and reinforce the abdominal wall in the skin flap donor site. (i) TRAM flap transplantation and the vascular anastomosis were performed, and the chest wall defect was repaired. (j) The appearance after surgery
1.4.4 Pectoralis Major Myocutaneous Flap
The pectoralis major is fan shaped with a large range, and the starting point is divided into three parts such as clavicular part, sternocostal part, and abdominal rib part. The clavicular part starts from the medial half of the clavicle, and the muscle fibers travel obliquely toward the lower outer side; the sternocostal part starts from the front of upper six costal cartilages on the lateral side of the sternum, and in general, the muscle fibers travel parallelly and outwardly; the abdominal rib part starts from the anterior sheath of rectus abdominis muscle and the distal ends of fifth to seventh ribs, and the muscle fibers travel obliquely toward the upper outer side. Three parts of muscle fibers aggregate outwardly to form a flattened tendon to the end of the crest of the greater tubercle of the humerus. The blood supply of the pectoralis major muscle comes from multisource; there are three main sources: the thoracoacromial artery, the pectoral branch of the axillary artery, and the perforating branches of the internal thoracic artery. The pectoralis major muscle is mainly controlled by the lateral pectoral nerve and the medial pectoral nerve.
There are mainly two methods of chest defects repairment with pectoralis major muscle: The first method is to take the perforating branch of the internal thoracic artery as the pedicle to form the myocutaneous flap, and then the myocutaneous flap is turned over reversely to repair the wound. The second method is to take the thoracoacromial artery as the pedicle to form the myocutaneous flap to repair the wound.
The marking method for the body surface projection of thoracoacromial artery approach is shown in Fig. 16.11, ab is the connecting line between the shoulder peak to the xiphoid process, the point o is the point of intersection between the line cd made from the clavicle midpoint and the connecting line ab, both lines are vertical, and the cob line is the body surface travel path of thoracoacromial artery.
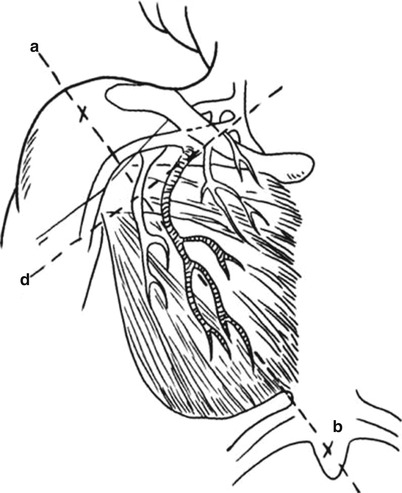
Fig. 16.11
Design of pectoralis major myocutaneous flap (the cob line of the body surface travel path of thoracoacromial artery)
The myocutaneous flap is designed along the body surface line according to the need of repairing the defects, the range of the design reaches upward to the level of armpit crimple and downward to the level of the xiphoid process, the inner boundary reaches the sternal margin, and the outer boundary reaches the anterior axillary line. When the surgery is performed, the pedicle skin is incised firstly, and then the skin and the full-thickness pectoralis major muscle are incised along the outer margin of the skin flap, and the myocutaneous flap is separated at the deep surface of fascia propria. After the pectoralis major muscle is lifted up, the blunt dissection is performed at the deep surface of the pectoralis major muscle to the pedicle, and after the neurovascular bundle locating at the deep surface of pectoralis major muscle is found, the skin at the medial margin of the skin flap is incised along the design line and the full-thickness pectoralis major muscle; the pectoralis major myocutaneous flap is formed and transferred to repair the wound.
Get Clinical Tree app for offline access

- 1.
Case VII The patient, male, 57 years old, had a sternal tumor. The sternal tumor was extensively resected, and after the chest wall defect was repaired with the titanium mesh, the pectoralis major myocutaneous flap is transferred to repair the wound (Fig. 16.12).
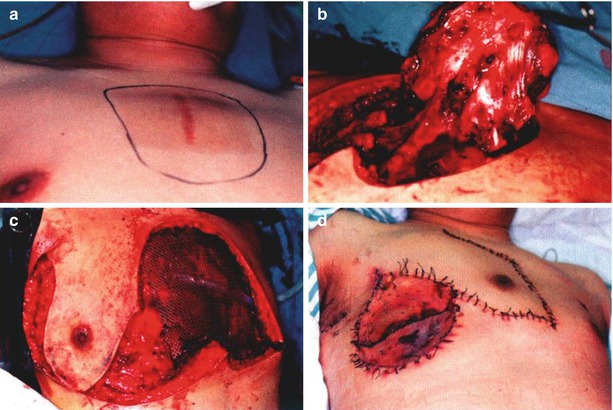
Fig. 16.12
Case VII. (a) Before surgery, the pectoralis major myocutaneous flap was designed. (b) The sternal tumor tissue was extensively resected. (c) The titanium mesh was used to repair the chest wall defect. (d) The pectoralis major myocutaneous flap was transferred to repair the wound, and the skin flap donor site was repaired with skin transplantation
- 2.
Case IX The patient, male, 49 years old, had a sternal tumor. After extensive resection of tumor tissue (including four pairs of costal cartilage and part of the sternum), the sandwich-type chest wall prosthesis made of double layer polyester mesh plus bone cement and the pectoralis major myocutaneous flap are transferred for repair and reconstruction, and the skin flap donor site was repaired with skin transplantation (Fig. 16.13).
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
 Defect Repair After Breast Cancer Surgery
Defect Repair After Breast Cancer Surgery

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

