Fig. 15.1
The incision of skin-sparing modified radical mastectomy. (a) The circular incision 5 mm away from the areola margin. (b) The biopsy incision around the areola extended toward the outer side of the breast (the incision looked like a table tennis racket). (c) The biopsy incision around the areola extended toward the outside or inside of the breast. (d) The incision after removal of a part of the skin on the surface of the mass
For patients with huge and sagging breasts, especially those whose breast at the healthy side also needs to receive plastic surgery, it is necessary to perform breast plastic surgery at the same time of removing the breast and remove the excessive breast skin to achieve bilateral symmetry. Based on the vertical scar breast reduction method, the incision for partial resection of the skin below the breast can be used to the reduced breast skin. For particularly large breasts, when it is required to reduce the skins in both vertical and horizontal directions, it is recommended that the surgery is completed by several times. The vertical incision is used to reduce the horizontal skin at first (Fig. 15.2a), and the breast reconstruction is performed; the vertical skin is reduced 6 months later, and the incision is made in the inframammary fold, and then the “orecchiette” of breast reconstruction is removed and reconstructed (Fig. 15.2b). The advantages of the fractional resection are the same as the characteristics of the vertical breast reduction, and it can reduce the length of the incision in the inframammary fold and reduce the formation of scars.
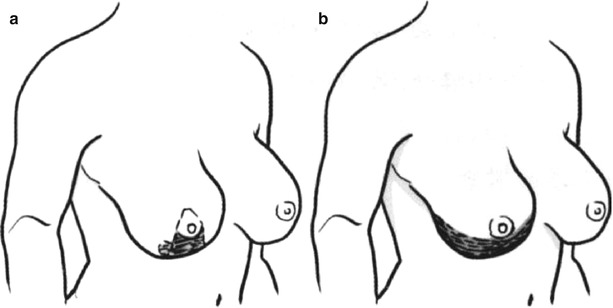
Fig. 15.2
The surgical incision in macromastia patient after sparing modified radical mastectomy. (a) The vertical incision for reducing the horizontal skin. (b) The incision in the inframammary fold for reducing the vertical skin
1.4.3 Surgical Methods
- 1.
Mastectomy and axillary lymph node dissection: The surgeries are performed under general anesthesia. The breast flap is stripped at first, then the subcutaneous resection of mammary tissue is performed, and then the axillary lymph node dissection is performed. Two issues should be paid attention to during mastectomy, namely, the first one is to ensure the blood supply of the skin flap, and the second one is to maintain the intactness of thoracodorsal vessels. When the skin flap is dissected, it is required to not only remove all breast tissue but also ensure a certain thickness to avoid excessive tissue damage caused by the electric knife and maintain a good supply of the skin flap blood supply. Maintaining the intactness of thoracodorsal vessels can make preparations for carrying out vascular anastomosis, if necessary in the process of breast reconstruction, and can increase the safety of surgery. The axillary lymph node dissection can be performed referring to modified radical mastectomy.
- 2.
Immediate breast reconstruction: The TRAM flap or extended latissimus dorsal myocutaneous flap can be selectively used for immediate breast reconstruction after skin-sparing mastectomy. The required skin tissue for immediate breast reconstruction after skin-sparing mastectomy is limited to the area of the nipple and areola. When the second-stage local flap nipple and areola reconstruction is performed, the circular areola skin has been slightly pulled and transformed; thus, it is necessary to make some adjustments. The areola skin should be slightly larger than that in the contralateral side during immediate reconstruction of breast body, and it can be adjusted to the size which is symmetrical to that of the healthy side when the second-stage nipple reconstruction is performed.
- (1)
TRAM flap breast reconstruction: The skin-sparing radical mastectomy retains the pectoralis major muscle and breast skin on the basis of modified radical mastectomy, while the breast reconstruction only requires reconstructing the breast body, and it needs small tissue volume compared to tissue volume needed after radical mastectomy. The TRAM flap pedicled with superior epigastric vessels with removal of tissues in area 3 and 4 can meet the needs of breast reconstruction, and it is an effective and feasible surgical method. After the abdominal incision is sutured, the blood supply of the skin flap is intraoperatively examined; when there are signs of spotted skin and venous congestion, the epigastric inferior vessels and thoracodorsal vessels should be anastomosed to increase the safety of surgery. It is generally adequate to anastomose a vein.
When the TRAM flap breast reconstruction is performed, the patient is placed in the supine position, the contralateral rectus abdominis muscle is taken as the pedicle to harvest TRAM flap, which is transferred to the chest through the subcutaneous tunnel, and the abdominal incision is closed. The following several points should be noted during harvesting of TRAM flap: ① after the epigastric inferior vessels are found with intramuscular separation techniques, the running directions of the blood vessels are confirmed behind the muscles, then the rectus abdominis muscle is separated, and then the muscle is brought into the skin flap minimally; ② in order to prepare for vascular anastomosis if necessary, the epigastric inferior vessels are separated to the femoral artery and vein, and they are harvested as long as possible for standby application; ③ the sputum is aspirated before the patient wakes, and the extubation is timely carried out to prevent the choking caused by respiratory irritation, which will lead to the burst apart of the area where the rectus abdominis muscle is sutured; ④ the drainage tube should be drawn out through the middle of the lower abdomen, because the effusion easily occurs in this site to form the seroma, and the wound healing is delayed; and ⑤ attentions are paid to the repair of abdominal shape. The measures such as deepening the navel area, forming the depression on the middle of the abdomen, and highlighting the outline of the rectus abdominis muscle are adopted to simulate the abdominal morphology of the young woman [13, 14].
- (2)
Breast reconstruction with extended latissimus dorsal myocutaneous flap: The patient is placed into the lateral position to receive mastectomy, axillary lymph node dissection, and breast reconstruction. A crescent-shaped incision is made on the back corresponding to the area covered by the brassiere, and it is bent toward the head side. The flap width is about 7 cm. The latissimus dorsi myocutaneous flap and its surrounding fat tissue are harvested, and then the serratus anterior branch of the thoracodorsal artery is separated and protected and is transferred to the chest via subcutaneous tunnel. The areas of the shoulder and buttock are propped up with pillows after surgery to prevent flap necrosis caused by compression of the donor site, and the patient is encouraged to carry out early activities after recovery from anesthesia. Generally it is not needed to use the breast prosthesis in breast reconstruction with extended latissimus dorsal myocutaneous flap.
When combined with breast prosthesis for breast reconstruction, the muscle should cover breast prosthesis as far as possible, especially in the area around the areola incision, so as to prevent prosthesis exposure when the partial necrosis of original breast skin margin occurs after surgery. When the prosthesis is covered by the muscle, the necrotic tissue can be removed, and the incision is closed and sutured again, or the wound will be healed by dressing change.
- (3)
Breast shaping: The key of breast shaping is to keep the symmetry of the inframammary fold with that at the healthy side. If the inframammary fold is stripped off during mastectomy, the skin and the underlying tissue should be sutured and fixed to form the inframammary fold. When the inframammary fold is fixed, the distance between the areola to the inframammary fold should be equal to that at the healthy side. Otherwise it will easily lead to deviation of nipple position or the insufficient fullness of the lower half of the breast. During breast shaping, the upper and outer side of the skin flap are sutured and fixed onto the upper margin and outer upper side of the cavity gaps in the anterior part of the chest, and the areola area skin is preserved; meanwhile, the epidermis is removed, and the skin flap is folded and shaped; finally, the wound margin is sutured (Fig. 15.3).

Fig. 15.3
After immediate breast reconstruction with the TRAM flap after modified skin-sparing mastectomy
- (4)
Nipple reconstruction and auxiliary operations: At the third month after surgery, the star-shaped flap is used for reconstruction of the nipple and areola after the flap swelling subsides and the condition is stable, and then the colored tattoo is made; thus, the entire process of breast reconstruction is completed. If there is local asymmetry, it is needed to be adjusted with syringe liposuction. In the immediate breast reconstruction after modified skin-sparing mastectomy, the position of the nipple and areola can be limited; in individual case, the nipple and areola reconstruction can be performed ahead of time about 2 weeks after reconstruction of the breast body.
- (1)
1.4.4 Sensory Recovery
After immediate breast reconstruction combined with modified skin-sparing mastectomy, because of the extensive dissection between the skin flap and the base, the sense of the original breast skin disappears transiently. The sense of touch begins to recover firstly at the second week after surgery, and the sense of pain begins to recover at 4 weeks after surgery. At sixth month after surgery, in addition to slight poor two-point discrimination, the sense has been basically restored to the same level as that at the healthy side. A slight tactile and pain sense of the nipple and areola skin can only be restored at the sixth month after surgery.
1.4.5 Complications
The common complication of the skin-sparing modified radical mastectomy is the partial necrosis of the original chest skin. It is mainly due to the fact that the stripped skin is too thin or the electric knife damages the skin tissue. Slavin reported that the incidence rate was as high as 21.6% in 51 cases of patients, while Hidalgo reported that the incidence rate was zero in a group of 28 cases of patients. In our group of patients, only one patient had chest skin congestion and redness after surgery, and there was only 1.5 cm of necrosis in the incisal margin skin, which healed after conservative treatment.
The axillary effusion is often caused by intraoperative incomplete hemostasis or poor drainage. The negative pressure drainage tube should be adjusted and replaced when the axillary effusion occurs to ensure smooth drainage and prevent air leakage, and the local pressure dressing is performed. One patient underwent drainage for 12 days after surgery, and then the wound was healed. The local small effusion in parasternal area may be treated by puncture and suction, and the pressure dressing is performed. When the prosthesis is used for breast reconstruction, the perforation of the prosthesis should be prevented.
1.5 The Modified Radical Mastectomy with Preservation of Nipple and Areola and the Immediate Breast Reconstruction
With the progress of the treatment of breast cancer, maintaining the perfect morphology of the female breast at the same time of radically curing the tumor has achieved broad consensus. Based on the Fisher’s theory of breast cancer biology, the surgical treatment of breast cancer has experienced the transitions, such as Halsted radical mastectomy, extended radical mastectomy, and modified radical mastectomy, and is now developing toward the direction of breast-conserving surgery which combines the mass resection or quadrant resection with radiotherapy; thus, the scope of local resection is increasingly narrowed. Traditionally it is believed that the breast cancer surgery should completely remove the breast tissue and all ductal epithelial tissues including those in the area of the nipple and areola. Along with the progress of treatment of breast cancer, especially after carrying out of the breast-conserving treatment, there has been a qualitative change in the understanding of the breast cancer tumor characteristics. The treatment of breast cancer should be the same as the treatments of other tissue tumors, and the purpose is to remove the tumor tissue and the possibly involved surrounding tissues and lymph nodes. Therefore, some people are continuously exploring the methods for breast cancer treatment with preservation of the nipple and areola since a very early period at home and abroad. With the constant improvement of breast reconstruction technology in recent years, the modified radical mastectomy with preservation of the nipple and areola is attached with great importance again. Combined with immediate breast reconstruction, it has become the gland replacement therapy in its true sense.
The progresses of the modified radical mastectomy with preservation of the nipple and areola mainly focus on continuous improvement of surgical incision, and it is expected to reduce surgical scars and improve cosmetic results. The surgical incisions reported in the literatures include inframammary fold incision, U-shaped incision, anterior axillary fold incision, etc., and the methods for breast reconstruction include breast prosthesis implantation, TRAM flap, and latissimus dorsi myocutaneous flap. We used subaxillary longitudinal incision to simultaneously complete the breast cancer resection and the breast reconstruction with expanded latissimus dorsi myocutaneous flap, and the surgical results were improved significantly.
1.5.1 Indications
It is mainly applied to early breast cancer patients with requirements for breast reconstruction whose lesions are far away from the nipple and areola without general surgical contraindications, and it is not suitable for patients with advanced tumors.
1.5.2 The Use of Subaxillary Longitudinal Incision for Immediate Breast Reconstruction with the Expanded Latissimus Dorsi Muscular Flap After the Modified Radical Mastectomy
- 1.
Incision design: A longitudinal incision is made at the midaxillary line under the armpit, and a length is about 10–15 cm; thus, the incision is completely covered when the upper limbs are sagging, and no surgical scars are left on the chest and back. The incision is near the anterior axillary fold, and it is easy to expose the incision scar when the upper limbs swing (Figs. 15.4 and 15.5).
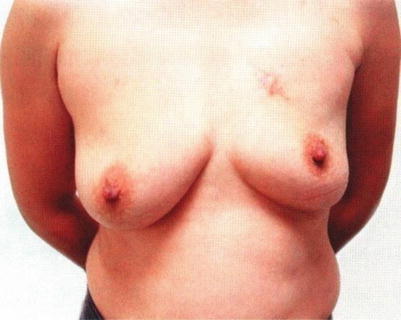
Fig. 15.4
After immediate breast reconstruction with the expanded latissimus dorsi muscular flap after the modified radical mastectomy with preservation of the nipple and areola

Fig. 15.5
The lateral chest wall incision of immediate breast reconstruction with the expanded latissimus dorsi muscular flap after the modified radical mastectomy with preservation of the nipple and areola
- 2.
Surgical methods
- (1)
Mastectomy and axillary lymph node dissection: The surgery is performed under general anesthesia. The patient is placed in the lateral position; the breast flap is separated and stripped at first and then is separated to the inframammary fold; subsequently, the subcutaneous resection of mammary tissue is performed; after that, the axillary lymph node dissection is performed. The subcutaneous injection of the saline solution containing a little adrenaline for vertical separation is conducive to surgical operation. When the breast is resected, it is required to not only remove all breast tissue but also ensure a certain thickness to avoid excessive tissue damage caused by the electric knife and maintain a good blood supply of the skin flap. Maintaining the intactness of thoracodorsal vessels is the premise of breast reconstruction with latissimus dorsal myocutaneous flap. The axillary lymph node dissection is completed through the same incision. When the tumor is near the breast skin, the skin with a width of 3 cm on the surface of the mass is removed, and the wound margin is directly sutured.
- (2)
Breast reconstruction with extended latissimus dorsal myocutaneous flap: The saline solution containing a little adrenaline is subcutaneously injected through vertical axillary incision with epidural anesthesia needle, then the back flap is separated and stripped, and then the latissimus dorsal myocutaneous flap and its surrounding fat tissue are harvested; subsequently, the serratus anterior branch of the thoracodorsal artery is separated and protected and is transferred to the chest via subcutaneous tunnel. The negative pressure drainage tube is placed in the donor site. Generally it is not needed to use the breast prosthesis in breast reconstruction with extended latissimus dorsal myocutaneous flap (refer to relevant chapters for surgical methods).
- (3)
Breast shaping: The key of breast shaping is to keep the symmetry of the inframammary folds with that at the healthy side. If the inframammary folds are stripped off during mastectomy, the skin and the underlying tissue should be sutured and fixed to form the inframammary fold. When the inframammary fold is fixed, the distance between the areola and the inframammary fold should be equal to that at the healthy side, and otherwise it will easily lead to deviation of nipple position or the insufficient fullness of the lower half of the breast. During breast shaping, the muscle surface of the myocutaneous flap is folded and sutured to form the breast body, and the lateral margin of the breast body is sutured and fixed to prevent tissue lateral displacement after surgery. After the shaping is completed, a negative pressure drainage tube should be placed along the inframammary fold. The negative pressure drainage tube is routinely placed in the site of axillary lymph node dissection, and the compression bandaging is performed moderately with the pectoral girdle.
- (1)
- 3.
Progress in the harvesting of expanded latissimus dorsi muscular flap: The use of subaxillary longitudinal incision for immediate breast reconstruction with the expanded latissimus dorsi muscular flap after the modified radical mastectomy with preservation of the nipple and areola avoids the surgical incision scar on the breast surface. At the same time, how to reduce the scars on the back donor site and shorten the axillary scar has become one of directions for the scholars to explore. With the popularity of endoscopy, the endoscopic harvesting of expanded latissimus dorsi muscular flap can avoid the surgical scar on the donor site, but because the body shows a certain curvature and lacks natural cavities, and the difficulty of surgical operation is increased, some scholars hold adverse opinions. United States Anderson Cancer Hospital reported the application of robot-assisted harvesting of expanded latissimus dorsi muscular flap in 2011, which is likely to be one of the future development directions.
1.5.3 The Use of Breast Incisions in Immediate Breast Reconstruction After the Modified Radical Mastectomy
The use of subaxillary longitudinal incision for immediate breast reconstruction with the expanded latissimus dorsi muscular flap has obvious advantages, but when the TRAM flap or breast prosthesis is used for reconstruction, this incision is not suitable. The incisions reported in the literatures include inframammary fold incision, U-shaped incision, and periareolar incision, of which the breast incision has excellent exposure, and the scar is not obvious; thus, the reconstruction effect is good.
The breast incisions of the modified radical mastectomy with preservation of the nipple, areola, and breast skin are roughly divided into three types:
- 1.
The periareolar incision: If the areola circumference is small, if necessary, the incision can be extended toward the inside or the outside and even the inferior side according to the location of the tumor, which facilitates the exposure (Fig. 15.6a).
- 2.
The incision at the lateral side of the breast, the incision along Langer’s line above the breast, or the arc incision at the lateral side of the breast: All these incisions are located on the breast surface on the outside of the nipple, along the static tension line of the breast skin, which is conducive to reducing the scar formation (Fig. 15.6b).
- 3.
The incision at the lower part of the breast: This incision is particularly useful for patients with huge and sagging breasts, and the breast skin can be reduced, and the breast can be shaped during mastectomy, especially in the patients with the breast at the healthy side requiring plastic surgery simultaneously (Fig. 15.6c).
The mastectomy and axillary lymph node dissection are carried out via abovementioned incisions, and it is necessary to retain a certain thickness of the tissue at the bottom of the nipple to prevent papillary necrosis. If necessary, an additional skin incision can be made in the armpit, which is conducive to axillary lymph node dissection. The reconstruction method selectively uses the first-stage prosthesis implantation, dilator-prosthesis implantation, or TRAM flap reconstruction according to the circumstances.
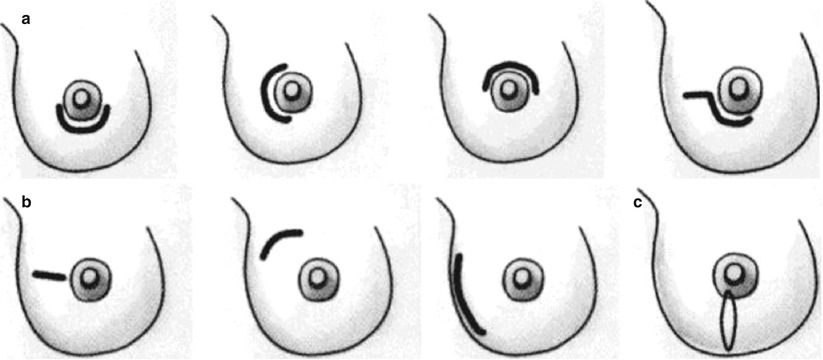
Fig. 15.6
Three types of incisions of the modified radical mastectomy with preservation of nipple, areola, and breast skin. (a) The periareolar incision. (b) The incision at the lateral side of the breast, the incision along Langer’s line above the breast, or the arc incision at the lateral side of the breast. (c) The incision at the lower part of the breast
1.5.4 Complications
The common complication of the modified radical mastectomy with preservation of the nipple and areola is partial or total necrosis of the nipple and areola, and it is mainly due to the fact that the stripped skin is too thin or the electric knife damages the skin tissue.
The axillary effusion is often caused by intraoperative incomplete hemostasis or poor drainage. The negative pressure drainage tube should be adjusted and replaced when the axillary effusion occurs to ensure smooth drainage and prevent air leakage, and the local pressure dressing is performed.
1.6 Breast-Conserving Treatment and Immediate Breast Reconstruction
With the progress of breast cancer treatment, now it is considered that the early breast cancer belongs to the systemic disease, and the distant metastasis is closely related to tumor biological characteristics, while the surgical removal of the breast tissue aims to remove the tumor tissue and control the local growth and recurrence of the tumor, and the scope of the surgical resection shows a narrowing trend. In recent years, the breast-conserving treatment mainly including partial breast resection combined with postoperative radiotherapy has been gradually popularized in oversea countries. The breast-conserving treatments in European and American countries have accounted for 70% of early breast cancers and account for only about 20% in Japan. The works in this aspect have been gradually carried out in areas such as Shanghai, Beijing, and Tianjin of China. However, due to factors such as the special caution of the oriental peoples, the fear of the tumor, poor tolerance to tumor recurrence, as well as insufficient popular science propaganda education on breast cancers and due to the fact that the tumors have developed into middle and advanced stage when the patients visit hospital, the breast-conserving therapy has not been popularized and applied in China. According to meeting data of the breast cancer branch of Shanghai Anti-cancer Association on December 25, 2010, the breast-conserving surgeries in Shanghai account for about 7–9% of breast cancer surgeries, and most patients still receive preferably the modified radical mastectomy. The breast-conserving treatment has three purposes: ① to completely remove the tumor tissue including the part of normal breast, ② to meet the requirements of female physical beauty, and ③ to maintain the sensation of the breast as far as possible.
So far, a lot of surgical methods for breast-conserving treatment have been reported, including names such as mass resection, segment resection, local lesion resection, quadrant resection, and partial breast resection. Except for the quadrant resection, other methods do not particularly limit the resection range of surrounding normal breast tissue. We hold the opinion that they are more appropriately to be called as partial breast resection, and its connotation is to remove the tumor tissue and part of the surrounding normal breast tissue. The breast-conserving treatment is defined as partial breast resection combined with local radiotherapy. If the tumor is located in the upper outer quadrant of the breast, the patient should also undergo axillary lymph node dissection simultaneously. After the early-stage breast cancer patients undergo quadrant resection with postoperative radiotherapy, the survival rate and local recurrence rate are the same as those of patients after undergoing mastectomy; but for some patients with smaller breasts, excessive tissues are removed in quadrant resection, which affects the appearance of breast. So far, the best volume of resection of normal tissue around the tumor still has no clear criteria, and further clinical studies are expected to be carried out.
1.6.1 Influence Factors on Breast-Conserving Treatment
- 1.
Oncological factors
- (1)
The frozen section examination of incisal margins should be carried out intraoperatively, but the pathological examination can only provide the approximate situation. Theoretically, the complete histological examination for incisal margins of the tumor with a diameter of 2 cm requires at least 2000 sections, but in the actual clinical work, a small number of sections can be only taken to reflect the local situation. Therefore, by contrast, the nature of the tumor can better determine the volume of resection of tissue and the prognosis.
- (2)
The histological features of the tumors: 1 cm of breast tissues surrounding the tumor should be removed in patients with the sclerosing ductal carcinoma with clear boundaries; the volume of resection of tissues in the patients with invasive glandular carcinoma with unclear boundaries should be increased, and the examination of incisal margins is carefully performed; for the patients with invasive ductal carcinoma, which grows invasively along the ducts, the resection volume should be further extended, and the careful pathological examination is performed. It is reported in the literatures that the local recurrence rate of this type of tumors is higher, and it is considered unsuitable for breast-conserving treatment, and the mastectomy should be performed.
- (3)
The breast-conserving treatment is not suitable for the multicenter breast cancer.
- (1)
- 2.
Cosmetology factors: The significance of breast-conserving treatment is to completely remove the tumor tissue but not destroy or destroy as little as possible the appearance of the female breasts. Therefore, the factors relating to cosmetology should be considered during the treatment process.
- (1)
Relationship between the tissue resection volume and the breast size: For the patients with medium-sized or smaller-sized breast, the removal of excessive breast tissue volume can cause serious breast deformation, and the fiber contracture due to the postoperative radiotherapy will further aggravate the breast deformation in some patients. It is generally believed that the tissue resection volume in the patients with medium- and small-sized breasts does not exceed 25% of the total volume; the larger tissue resection volume can be removed in patients with larger breasts. If certain principles for breast reduction surgery in plastic surgery are adopted, a good appearance still can be maintained even though 50–60% of the breast is removed. In this type of patients, the appropriate local dissociation after resection of bulk tissue can maintain good blood supply to the breast tissue, but also maintain the good appearance of the breast shape.
- (2)
The location of the tumor: The breast tissue volume in the upper part within the breast is less and the thickness is thin; thus, the removal of the tumor tissue in this part can cause deformities such as local depression or upper shift of the nipple; on the contrary, the breast tissue volume in upper outer part of the breast is more; thus, the deformation will not easily occur after the tumor in lateral or lower part of breast is resected, and the cosmetic effect is better.
- (3)
The direction of resection of the breast skin and breast: Any surgical incision of the breast should consider related cosmetic surgery principles. In general, the skin incision should be consistent with the skin tension lines, but the nipple will be easily shifted downward when the transverse incision in the lower half of the breast is made to resect a part of the skin. Therefore, the transverse incision should be made in upper half of the breast, and the radial incision should be made in the lower half of the breast. The glandular part is resected using radial wedge or fusiform resection, so as to reduce nipple displacement. The tumor located in the middle of the breast should be resected through areola margin incision or the transverse incision within the areola. The tumor near the areola should be resected together with the nipple and areola, and the nipple and areola can be reconstructed at a later stage.
- (4)
Scar contracture after surgery and radiotherapy: The surgery and radiotherapy may cause fibrosis, and the wound hematoma or seroma can further cause scar formation to lead to contractures and even lead to the nipple displacement. The induration can be palpated in local area in some patients, which is softened gradually and disappears over time. The surgical trauma should be reduced as far as possible during surgery; thus, the subcutaneous extensive dissection is avoided; meanwhile, the careful hemostasis is carried out, and the principles of noninvasive surgery are strictly adhered to.
1.6.2 Indications
It is mainly used in patients with early-stage breast cancers who require breast-conserving treatment, including tumors of stages l and 2 and 2a. The best indications are focal ductal carcinoma in situ and invasive carcinomas of stage T1N0M0 andT1N1M0.
There are more than two lesions in different quadrants for the same breast; the affected breast has diffuse calcifications; there is diffuse ductal carcinoma, and the treatment unit does not have conditions for radiotherapy. All of the above conditions should be considered as the surgical contraindications. The patients receiving breast-conserving treatment should be followed up regularly. If the breast-conserving treatment fails, the surgical resection will be performed at any time. Therefore, the breast-conserving treatment should also be used with caution in patients lacking regular follow-up.
1.6.3 Surgical Methods
- 1.
Partial breast resection: Firstly, the methylene blue is used to mark the surgical skin incision and the resection range of the breast; if there is a biopsy incision, the biopsy incision scar should be removed together as far as possible. The skin flap is separated on both sides to fully expose the tumor, then en bloc resection of 1–2 cm of breast tissue surrounding the tumor is performed, and the depth reaches up to the pectoralis major muscle, including part of the pectoralis major muscle fascia. If the bottom is near the pectoralis major muscle, a part of pectoralis major muscle should be removed, and the resection depth is consistent with that of the modified radical mastectomy (see Fig. 15.6). The resection specimen is marked with suture lines. Although in theory, the frozen sections cannot fully reflect the situation in surgical margins; it is still necessary to carry out frozen pathological examination in clinical practice. If the surgical margins are invaded, the resection range should be expanded.
- 2.
Effects of gravity action: After partial breast resection, the breast tissue defects can be aligned and closed by themselves with the help of gravity action; thus, most of them do not need to be sutured. Due to the gravity action, the incisions in middle upper and lower parts of the breast can’t be closed, and furthermore the incision wound is ripped off. Therefore, the breast tissues in these parts need to be sutured. When the glandular tissue is selectively sutured, it is recommended to use the absorbable suture lines. When the alignment is performed, tight knots or distorted tissues should be avoided; otherwise, the local induration can be palpated after alignment. The patient is placed in the semi-recumbent position during surgery. Whether there is local depression or deformation is observed, and timely adjustments should be made when the deformation is found. Finally, the drainage tube is placed, and the skin is sutured with nylon threads.
- 3.
Axillary lymph node dissection: In addition to the primary lesions located in the tail of the breast, an additional incision should be selected for the axillary lymph node dissection. S-shaped or axillary fold incision is often used, and specific methods are the same as those of axillary lymph node dissection.
- 4.
The immediate breast reconstruction after breast-conserving surgery can be divided into two types: one type is the surgery to adjust the original breast tissue, and another type is the tissue augmentation surgery.
- (1)
The surgery to adjust the original breast tissue is suitable for patients with larger breasts, and the surgical method is determined based on the breast volume and the resection scope of the breast:
- (a)
For the patients with larger breasts and small-sized resection scope, it is not needed to make special adjustments.
- (b)
For the patients with larger breasts and medium-sized resection scope, the basal breast is slightly separated on both sides of the skin flap, and the breast body is sutured again. The breast tissue near the areola is thicker; thus, two-layer closure should be performed; the breast tissue near the outside of the breast becomes thin; thus, only a layer of closure needs to be performed.
- (c)
For the patients with larger-sized resection scope, the principles for breast reduction surgery can be applied. The defect in lower half of the breast is repaired with inferior pedicle flap, and the defect in upper half of the breast is repaired with superior pedicle flap.
- (a)
- (2)
The tissue augmentation surgery is suitable for patients with a smaller breast size and a relatively large tissue resection volume. Since the original tissue volume is less, and lacks the space for adjustment, it is necessary to carry out tissue transplantation and filling. The commonly used transplants include local subaxillary skin flap and latissimus dorsi myocutaneous flap. According to the size of skin defects, the epidermis of whole skin flap can be removed, and partial skin of the skin flap can also be retained (refer to related chapters and sections for the surgical methods). Most authors believe that TRAM flap should be used in the reconstruction after whole mastectomy, and the TRAM flap should not be used in the repair of partial breast defect. It is noteworthy that for the patients with smaller breasts, relatively large resected breast tissue volume, and severely distorted breast, the morphological effects of the skin-sparing modified radical mastectomy combined with breast reconstruction would be better.
- (1)
1.7 Delayed Breast Reconstruction
1.7.1 TRAM Flap Breast Reconstruction
Hartrampf reported that there was a history of nearly 20 years since the use of TRAM flap for breast reconstruction, and it is currently the most commonly used surgical method for breast reconstruction and has been called as the standard surgery for breast reconstruction [12].
- 1.
Applied anatomy: The rectus abdominis muscle is located on both sides of the abdominal midline, and the upper end is wider and the lower end is narrow. The upper end starts from the xiphoid and the areas of fifth to seventh costal cartilages, and the lower end terminates at the pubic symphysis and pubic crest. The rectus abdominis muscle is located within the sheath of rectus abdominis muscle, with three to four tendinous intersections, and Hunter’s line is located between both left and right sheaths. The anterior sheath of the rectus abdominis muscle is intact, the posterior sheath forms into the semicircular line at 5.8 cm below the umbilicus, and there is no posterior sheath below this line.
The blood supply of the TRAM flap mainly comes from the superior and inferior epigastric arteries and their accompanying veins. The upper one-third of the rectus abdominis muscle is supplied with blood by superior epigastric vessels. The middle and lower parts of the rectus abdominis muscle are supplied with blood by inferior epigastric vessels. There are very big individual differences between superior and inferior epigastric vessels. It is generally believed that there exist direct anastomosis branches between superior and inferior epigastric vessels within muscles.
Single-pedicled TRAM flap is divided into four regions according to the status of the blood supply: region I is located on the surface of the abdominal rectus pedicle, and the blood supply is best; region II is located on the surface of the contralateral abdominal rectus muscle, and the status of blood supply takes second place; region III is located on the outside of the abdominal rectus pedicle, and on the same side of the muscle pedicle, the status of blood supply takes third place; and region IV is located on the outside of the contralateral abdominal rectus muscle of the pedicle and on the contralateral side of the muscle pedicle and is symmetrical to region III, and the blood supply is worst (Fig. 15.7).
Fig. 15.7
Partitions of blood supply of pedicled TRAM flap
- 2.
Surgical method and indications: The safe blood supply range of TRAM flap pedicled with unilateral superior epigastric vessels is about 60% of the skin flap, namely, regions I and II and part of region III. For patients with scars in the center of the lower abdomen, the blood supply to the contralateral side of pedicle is affected. The appendectomy scar does not affect the blood supply of the skin flap; if there is a transverse incision scar of the rectus abdominis muscle, the pedicled transfer cannot be performed. Therefore, after the modified radical mastectomy with preservation of pectoralis major muscle, in addition to appendectomy incision, the patients without other abdominal scars are suitable for application of single-pedicled TRAM flap.
After radical mastectomy or extended radical mastectomy, the required tissue volume is large, while the tissue volume of the single-pedicled TRAM flap is inadequate; for patients with scars in the center of the lower abdomen, the contralateral blood supply of the single-pedicled TRAM flap is affected, and the surgical methods such as double-pedicled TRAM flap, vertical rectus abdominis myocutaneous flap or combined with additional vascular anastomosis, and free transplantation should be selected. The surgical method combined with additional vascular anastomosis is selected preferably.
- 3.
Surgical design: The marker line is made in the patient in standing position before surgery – ① the range of tissue defect in the anterior part of chest, a wide range of tissue defects need to be filled from the infraclavicular area; ② the inframammary fold which is symmetrical to that at the contralateral side; ③ the midpoint of the xiphoid process; and ④ the midpoint of the upper pubic hair.
When TRAM flap is designed, it is required to determine the upper margin of the skin flap at first. Since the perforating branches of blood vessels around the navel are thickest and richest; the upper margin of TRAM flap is located at 0.5–1 cm above the navel; the upper margin passes through the slight upper side of the mons veneris, and it should be considered that the donor site can be sutured directly. Especially in younger patients, the abdominal skin is already strained and lacks of sagging; thus, the lower margin of the skin flap should be shifted upward moderately to prevent the donor site wound dehiscence or partial skin necrosis, while the incision in the pubic hair easily leads to necrosis of the middle part of the apron-like flap in upper abdomen. The skin flap presents as fusiform, and the range is limited between bilateral anterior superior spines that is limited within the blood supply range of the epigastric inferior vessels and the superficial inferior epigastric vessels. If exceeding this range, the blood supply area of the superficial circumflex iliac vessel will be brought into the skin flap, which becomes the cause of partial skin flap necrosis. In order to reduce the distortion of the pedicle when the skin flap is transferred, the contralateral rectus abdominis muscle of the reconstructed side is usually selected as the muscle pedicle. Recently, it is reported that the ipsilateral rectus abdominis muscle is also used as the muscle pedicle.
Part of rectus abdominis muscle and its sheath: The blood supply of the skin flap is ensured preferentially for the part above the navel, and the lateral one-third of the rectus abdominis muscle is only retained. A 2–3 cm-wide rectus abdominis anterior sheath in the middle part is harvested, and the medial two-thirds of the muscle is brought into the pedicle. The muscle pedicle is separated upward to the costal margin, then the superior epigastric artery and vein which enter into the body from underneath the costal cartilage are confirmed, and subsequently the skin flap is rotated and transplanted to the chest and is temporarily fixed. Only a part of the rectus abdominis muscle is harvested, and a part of the rectus abdominis muscle and its sheath are retained in the abdomen as much as possible, which is an important measure to prevent the abdominal complications such as abdominal weakness and abdominal wall hernia.
- 4.
Surgical method: The surgery is performed under general anesthesia; the urethral catheter is placed before surgery. The thoracic scar is removed at first. The skin flap in anterior part of the chest is separated, upward to the infraclavicular area, outward to midaxillary line, inward to the parasternal area, and downward to the inframammary folds. The subcutaneous tunnel is made from the center of the chest to the abdomen, and when the subcutaneous tunnel is made, it is supposed to prevent the excessive separation of inframammary fold at the affected side and the damage to the morphology of the intermammary groove.
The area around the navel is incised, and the navel is separated from the skin flap. Then the upper margin of TRAM flap is incised and obliquely enters into and incises the fat layer toward the head side, which is conducive to bringing more adipose tissue and main periumbilical perforator vessels into the skin flap. The apron-like flap is separated toward the side of the head, the costal arch edge is crossed, and the subcutaneous tunnel in the chest wound is connected to. When the abdominal flap is separated, some adipose tissues are retained on the surface of the sheath of the rectus abdominis muscle, which is conducive to lymphatic drainage. The lower margin of TRAM flap is incised. At the contralateral side of the pedicle and starting from the outside, the separation is performed on the fascia surface to the center of the abdomen. At the ipsilateral side of the pedicle, the separation is performed from the outside to the inside to expose the myocutaneous perforator at the lateral side of the rectus abdominis muscle. The perforating branches of intercostal artery given off at the lateral margin of the rectus abdominis muscle are severed.
At the junction of the middle and lower one-third of the skin flap, the sheath of the rectus abdominis muscle is incised at the outer side of the myocutaneous perforator, and then the rectus abdominis muscle is separated to find the inferior epigastric artery and vein and confirm the running directions of the blood vessels. It is noted that the muscle is brought into the skin flap minimally. In order to prepare vascular anastomosis if necessary, the inferior epigastric vessels are separated to the femoral artery and vein, and they are harvested as long as possible for standby application. The abdominal wall hernia occurs mostly in the lower abdomen; thus, the rectus abdominis muscle and its sheath should be retained on this site as much as possible to prevent the formation of postoperative abdominal wall hernia. Namely, 3 cm-wide rectus abdominis muscle and its sheath below the navel are harvested, and both inner and outer sides of the rectus abdominis muscle and its sheath are retained.
The anterior sheath of rectus abdominis muscle is closed from top to bottom, and eight shaped two-layered sutures are performed using no. 2 silk suture line. The anterior sheath of the contralateral rectus abdominis muscle is also partially sutured, so as to maintain the symmetry of abdominal wall tension. The navel area is fixed with the anterior sheath of rectus abdominis muscle, so that the navel can be located in the center position; or the anterior sheath of the contralateral rectus abdominis muscle is partially incised, and the navel is fixed to the center position (Fig. 15.8). The patient is adjusted in a semi-sitting position. An opening is made in the center of the skin, and the fatty tissue surrounding the opening within the inner face of the skin is cut off, so that the newly formed navel can have deeper depression. A longitudinal incision is made in adipose tissue layer at the center of abdomen above the navel, and the skin flap is turned over, and then a portion of adipose tissue at the margin of the longitudinal incision is cut off to form a subcutaneous depression. The skin flap is put back to original place and is fixed with the anterior sheath by several stitches at the depression site in the center of the abdomen and the bilateral flanks, so as to simulate the morphology of the abdomen in young females. The drainage tube is placed, then the suprapubic wound is adjusted and sutured from the outside to the inside to avoid the formation of “orecchiette” on both sides, and, finally, the periumbilical area is sutured.
Fig. 15.8
Schematic diagram of TRAM flap breast reconstruction
At the same time of using TRAM flap to carry out breast reconstruction, the effect of abdominoplasty is also achieved for the donor site in the abdomen, especially for middle-aged women. Therefore, the treatment principles for the abdominal donor site are the same as those for the abdominoplasty. When the anterior sheath of the rectus abdominis muscle is closed, the anterior sheath of the contralateral rectus abdominis muscle is also partially sutured and closed to maintain the symmetry of abdominal wall tension, so that the navel can be located in the middle position. The navel is fixed with the anterior sheath of the rectus abdominis muscle during surgery, and a Y-shaped opening is made in the umbilical area at the middle line of the skin. The fatty tissue surrounding the opening within the inner face of the skin is cut off, so that the newly formed navel can have deeper depression. A portion of adipose tissue at the center of the upper abdomen is removed intraoperatively to form a subcutaneous depression, and the appropriate fixation with the anterior sheath is performed at the depression site in the center of the abdomen and the bilateral flanks, so as to simulate the morphology of the abdomen in young females.
According to methods for resection of breast cancer, the shaping methods of breast are slightly different. The design of skin flap is divided into transverse and longitudinal shape, and single-pedicled TRAM flap is designed mostly as longitudinal shape. Firstly, the upper outer one fourth of skin flap, namely, the region IV of the flap, is incised (see Fig. 15.7), and the upper end of skin flap is fixed and sutured to the upper margin of the lacuna in the anterior chest to simulate the caudate lobe of the breast and the anterior axillary fold; then the medial, lower, and lateral sides of the breast are fixed and the excessive skin is removed; furthermore, the folding and shaping are carried out and the wound margin is sutured. It is noted that the intermammary groove is made, and the breast shape with appropriate sagging and bulging which is symmetrical to that at the contralateral side is ensured. In the patients with modified radical mastectomy, the pectoralis major muscle and the pectoralis minor muscle are retained, and thus the morphology of anterior axillary folds is complete. The skin flap is placed by the inner on the upper part and the outer on the lower part, and the lateral curve of the reconstructed breast is highlighted. In the patients with radical mastectomy or extended radical mastectomy, the pectoralis major muscle is resected, and the tissue defects in the chest are severe. Therefore, it is required to fill the subclavicular and axillary dents and shape the breast ball for the breast reconstruction. The skin flap is placed by the inner on the upper part and the outer on the lower part, and the anterior axillary folds and breast curve are highlighted. In the patients with severe breast tissue defects, it is required to fix the skin flap to the medial upper arm to simulate the stop point and morphology of pectoralis major muscle.
The abdomen is bandaged with a bellyband after surgery, so that the skin flap of donor site is attached to the substrate, while the abdominal wall is strengthened and the formation of abdominal wall hernias is prevented. The pedicle passes through the area of the xiphoid process, and attention should be paid to preventing the local compression, which will affect the blood supply of the skin flap.
The anesthetic technique is particularly important. The aspiration of sputum should be performed before anesthetic awareness. The endotracheal tube is removed timely after anesthetic awareness, and when the extubation is performed, the assistant abdomen should press the abdomen to prevent choking during extubation, which can lead to the burst apart of abdominal wall sutures. The hospital where the authors work in has applied the technique of general anesthesia with laryngeal mask ventilation, namely, the laryngeal mask is used to cover the epiglottis and throat, and no tube is placed in the trachea; thus, the choking during extubation and the tracheal discomfort after surgery can be prevented. In addition, the general anesthesia with tracheal intubation plus the epidural anesthesia can greatly improve the safety of extubation and effectively prevent cracking of abdominal donor site.
The constipation and coughing should be prevented after surgery. The drainage tube is removed 4–5 days after surgery and then the patient can start walking. The stitches are taken out 10 days after surgery, and the patient can be discharged out of hospital if there are no special circumstances.
At the third month after surgery, after the flap swelling subsides and the condition is stable, the star-shaped flap is used to reconstruct the nipple and areola in outpatient clinic, and then, the tattoo coloring is carried out to complete the entire process of breast reconstruction.
- 5.
TRAM flap: The free transplantation of TRAM flap pedicled with inferior epigastric artery and vein maintains the epigastric inferior vessels as the main supplying vessels of the lower abdominal skin and subcutaneous tissue, and TRAM flap has good blood supply and less fatty degeneration and induration compared to the pedicled transfer. Partial rectus abdominis muscle is merely harvested and included into the flap, which reduces the damage to the abdominal muscles. For surgeons mastering skilled microsurgical techniques, the flap necrosis rate is 1–3%. In the 1990s, the free TRAM flap breast reconstruction had an increasing trend, and compared with pedicle transplantation, the disadvantages are that the operation time is prolonged by 1–2 h and the skilled microsurgical techniques are required, and the result of survival of skin flap is all or nothing.
The surgical operation is basically the same as that of the pedicled transfer. It is required to retain the epigastric inferior vessels as long as possible when the skin flap is separated. The branching blood vessels of the thoracodorsal vessels, the internal thoracic vessels, and the axillary artery and vein are generally selectively used as the blood vessels of the receptor site (Fig. 15.9). It is worth noting that although the required lengths of the inferior epigastric vessels are limited, it is recommended to separate and preserve the inferior epigastric vessels as long as possible for standby application when the internal thoracic vessels are selected for vascular anastomosis. Therefore, they can be anastomosed with the internal thoracic vessels or thoracodorsal vessels at the healthy side when the internal thoracic vessel at the affected side cannot be used due to anastomotic opening occlusion. The internal thoracic vessels are located at 1 cm beside the sternum, closely clinging to the subchondral area. When the internal thoracic vessels are exposed, firstly, the perichondrium in front of the costal cartilage is stripped off with the periosteal elevator, and the costicartilage is bitten off with rongeur forceps, and then the ophthalmology small scissors are used to cut open the costal perichondrium at the underside of the costal cartilage. If the perichondrium around the costal cartilage is stripped and then the costal cartilage is removed according to the general method, this will easily damage the thoracic artery and vein. When the internal thoracic vein is too small and cannot be used, it is required to harvest the saphenous vein of the lower limb to be bridged with the thoracic dorsal vein, or the cephalic vein of the upper limb is reversed and translocated and is anastomosed with the vein of the skin flap.
Fig. 15.9
The blood vessels in the receptor site which is available for vascular anastomosis
The blood circulation status of the skin flap is closely observed within 1 week after surgery. The surgical exploration should be timely performed when it is suspected that the anastomotic thrombosis is formed. The embolism area is removed, and the anastomosis should be carried out again.
- 6.
Inferior epigastric perforator flap: Koshima and Soeda (1989) firstly reported the inferior epigastric perforator flap completely without the rectus abdominis muscle. [18] took the lead in using this flap in breast reconstruction. The inferior epigastric perforator flap is the hypogastric skin flap which takes the inferior epigastric vessels as the vascular pedicle and takes its major vascular branch in periomphalic area as the nourishing blood vessels. Before surgery, the ultrasound or CTA is used to locate the perforating vessels; the shape and design of the skin flap are the same as those of TRAM flap. The major perforator vessels of the inferior epigastric vessels are found at the surface of the rectus abdominis muscle during surgery, and then the rectus abdominis muscle is separated along their traveling direction to look for the main trunk blood vessel. To protect the supplying perforator vessels, a little muscle tissue can be retained around the blood vessels. After the skin flap is formed, the supplying perforator vessels are anastomosed with the blood vessels in chest receptor site under a microscope.
The advantages of this method are that the morphology and function of the rectus abdominis are maximumly retained and the damage degree of the abdominal wall is reduced to a minimum level. The disadvantages are that the surgical operation is relatively cumbersome and the operation time is prolonged. It is easy to damage the perforator vessels during separation of blood vessels, especially when the pectus abdominis muscle is not included completely, and the probability of failure of the skin flap is increased.
- 7.
The hypogastric skin flap pedicled with superficial inferior epigastric vessels: The hypogastric skin flap pedicled with superficial inferior epigastric vessels refers to that the superficial inferior epigastric vessels are taken as the pedicle during the transfer and the skin flap is located on the surface of the rectus abdominis muscle; thus, the rectus abdominis muscle is not damaged at all, and the abdominal wall function is preserved to the greatest degree. However, the superficial epigastric vessels have more variation. Only about 20% of patients can use this method.
The flap design is the same as that of TRAM flap. Firstly, the lower margin of the skin flap is incised to look for the superficial epigastric vessels carefully. If the vessel diameter is larger than 1.5 mm, the surgery with superficial epigastric vessel flap can be performed; if there are no superficial epigastric vessels of suitable diameter, the inferior epigastric perforator flap can be used as replacement.
- 8.
Double-pedicled TRAM flap: Double-pedicled TRAM flap is a feasible treatment for the patients with scars in the middle of the abdomen and the need of undergoing reconstruction with the whole TRAM flap after radical mastectomy. Since the double-pedicled TRAM flap needs to harvest bilateral rectus abdominis muscle and the impact on the abdominal wall function is greater, it is particularly important to harvest a part of the sheath of rectus abdominis muscle and use the intramuscular separation techniques during surgery. Attentions are paid to the operation method, and it is not required to synthesize the artificial patch to strengthen the abdominal wall under normal circumstances. For patients with excessive removal of the rectus abdominis muscle and its sheath, it is required to use intraoperatively the autologous fascia, dermal tissues, or artificial patch (polyester mesh) to strengthen the abdominal wall.
The preoperative design and surgical operation are basically the same as those of the single-pedicled TRAM flap. The separation is carried out inward from both sides of the skin flap until the lateral blood vessels are exposed. Then a tunnel on the deep fascia is made at Hunter’s line in the middle of the navel and the lower margin of the skin flap; attention is paid to preventing damage to the perforator vessels at the medial side of rectus abdominis muscle. The anterior sheath of rectus abdominis muscle is incised at the outer side of the perforator vessels. Firstly, the inferior epigastric artery and vein are found. After the running directions of the blood vessels are confirmed, the lateral rectus abdominis muscle and the medial rectus abdominis muscle are splitted off, and then the sheath of the medial rectus abdominis muscle is cut off and gradually separated toward to the head side. Similar to single-pedicled TRAM flap, for the part above the navel, only 2–3 cm-wide anterior sheath of rectus abdominis muscle in the middle part and two-thirds of medial rectus abdominis muscle are harvested, and the lateral one-third is retained; for the part under the navel, only a part of the rectus abdominis in the middle part is harvested, and a portion of the sheath and muscle on both inner and outer sides are retained.
The skin flap is mostly designed as transverse shape after being transferred to the chest. The excessive skin is removed, and the clavicle depression is filled; subsequently, the morphology of anterior axillary fold and the mammary contour are reconstructed (Fig. 15.10)
.
Fig. 15.10
Double-pedicled TRAM flap breast reconstruction. (a) Before reconstruction. (b) After reconstruction
- 9.
Complications: The most common complications after TRAM flap breast reconstruction are flap necrosis and abdominal wall hernia formation in donor site. The complications after breast prosthesis reconstruction depend on the biological characteristics of the prosthesis itself, but the complications after TRAM flap breast reconstruction depend on the patient selection and the operation method and experience of the surgeon. We should be fully aware that the vast majority of complications after TRAM flap breast reconstruction can be avoided.
In earlier application of TRAM flap, the incidence rate of surgical complications was between 20% and 30% [19, 20]. Analyzed the complications in 346 cases of TRAM flap breast reconstruction, and the simple abdominal complication rate was 16% from 1981 to 1984. With the accumulation of surgical experience, the incidence rate of abdominal complications was decreased to 4% from 1985 to 1990. Hartrampf (1987) reported surgical complication rate in more than 300 patients: the partial skin flap necrosis rate was 6%, and the complete necrosis rate was 0.3%, and the abdominal wall hernia rate was 0.3%; in 1991, he reported that the incidence rate of partial skin flap necrosis was 3%, and the complete necrosis rate was 0. The reduction of complications is due to the accumulation of surgical experiences and the full understanding of the risk factors. According to the data from European and American countries, the risk factors related to the complications include obesity, smoking, previously treated with radiotherapy, hypertension, severe systemic disease, etc., with special emphasis on obesity factor. Kroll [21] divided the degree of obesity into four levels: emaciated, standard, obese, and severely obese. Their complication rates of TRAM flap breast reconstruction were 15.4%, 22.7%, 31.4%, and 41.7%, respectively.
- (1)
Skin flap necrosis: The best way to deal with skin flap necrosis is to avoid the occurrence of the skin flap necrosis. Clinical practice has proved that the safe area which can be carried by the single-pedicled TRAM flap accounts for about 60% of the total skin flap; when single-pedicled TRAM flap is selectively used, the region 4 and part of region 3 of the skin flap should be removed. If the skin flap necrosis is expected to occur during surgery, the inferior epigastric vessels should be anastomosed with the axillary vessels. The blood supply disorder of TRAM flap in earlier stage shows only poor venous return, congestion, and piebaldness in flap, and the microsurgical vascular anastomosis should be performed during surgery. If the venous congestion is found at the next day after surgery, it is required to open the incision again in the operating room and anastomose the epigastric inferior vessels with the axillary vessels.
After the occurrence of skin flap necrosis, when the necrotic boundaries are obvious, the thorough debridement is performed to remove necrotic tissue, and the reshaping is performed. It is noteworthy that the skin flap should be stretched again during debridement, and the reshaping of the breast after removal of necrotic tissue is carried out. If the necrotic tissue is removed during shaping, the debridement is incomplete often due to misgiving that the pedicle is damaged, and the wound cannot heal for a long time.
After debridement and shaping, the breast volume after reconstruction is slightly reduced, and most patients can accept it. For patients with a large range of necrotic tissue and too small breast volume after reconstruction and shaping, the breast prosthesis can be implanted under the skin flap at the second stage.
When the necrosis boundaries are not confirmed, the debridement should be performed after the necrosis boundaries are confirmed, and the antibiotic ointments such as chlortetracycline ointment and SD-Ag cream are topically applied during the waiting period, so as to prevent aggravation of the tissue necrosis due to secondary infection or the effusion under the scab.
- (2)
Abdominal wall weakness and abdominal wall hernia: The abdominal wall weakness is demonstrated as the distension of whole abdominal wall; the abdominal wall hernia is due to the fact that the local abdominal wall tension is too small and the intra-abdominal tissues herniate through this site. In early application of TRAM flap, it is emphasized that attentions should be paid to the blood supply of the skin flap. If excessive muscle and sheath tissue are brought into the skin flap, the incidence rate of abdominal wall hernia is higher. With the improvement of the study on blood supply of the skin flap and the operating techniques, the incidence rate is significantly reduced. We carried out (1999) a group of 34 cases of TRAM flap breast reconstruction; the abdominal wall hernia only occurred in one case. Attentions are paid to that the intramuscular separation techniques are used. More anterior sheath of rectus abdominis muscle is retained, and the sheath is doubly stitched. The sputum is aspirated before the patient wakes, and the endotracheal tube is removed timely to prevent the burst apart of muscle sutures due to choking. The sharp increase of intra-abdominal pressure caused by constipation and cough is prevented after operation, and the abdominal compression bandaging is performed. Furthermore, the patient wears elastic stretch tight pants within 3–6 months. These measures are conducive to prevent the occurrence of abdominal wall weakness and abdominal wall hernia.
In order to prevent the occurrence of abdominal wall hernia, some authors advocate using the artificial patch (including polyester mesh, nylon mesh, etc.), autologous fascia, and dermal tissue to strengthen the abdominal wall. Hein (1998) transplanted the skin tissue which was removed during skin shaping and then was de-epithelialized to the anterior sheath of the rectus abdominis muscle, so as to strengthen the abdominal wall and make good use of waste materials, which had achieved good results. For selection of reconstruction method, the single-pedicled TRAM flap or free transplantation should be selectively used, and double-pedicled TRAM flap is avoided as far as possible.
After the abdominal wall weakness or abdominal wall hernia occurs, the patient should wear reinforced elastic stretch tight pants until the surgical correction at the second stage is performed. The repair of abdominal wall hernia can be carried out together with other local adjustment surgeries. The area of abdominal wall weakness or abdominal wall hernia is separated through original abdominal surgical incision, and the herniated tissues are put back, and then the tissue patch is used for repair and is fixed onto the surrounding healthy anterior sheath and muscles of rectus abdominis muscle or fixed onto bilateral iliac crests. The patient should wear strictly the elastic stretch tight pants within 3 months after surgery and avoid strenuous exercise abdomen.
- (3)
Liquidation of fatty scleroma: The TRAM flap carries a lot of fat tissue, and the fat tissue is fragile and has a poor blood supply; thus, the ischemic degeneration or necrosis liquefaction easily occurs due to poor blood supply or tissue injury. When there is a large amount of liquefied fat, there will be a palpable undulating sensation. It is required to extract it out with a syringe, and the pressure dressing is carried out. The operation often needs to be repeated for multiple times; a small amount of liquefied fat can be self-absorbed. Most fat degeneration and induration can be absorbed with the passage of time, and some of them form into isolated fat indurations in individual cases, which can be removed during implementation of other plastic surgery.
Sometimes the isolated fat induration is easily confused with tumor recurrence, and the local biopsy examination is useful in differential diagnosis.
- (4)
Incision disruption: The sites with incision disruption are mostly located in the margin of the skin flap in receptor site and in the donor site with too large tension during suture. When the skin flap in donor site is designed, it should be considered that it is appropriate as long as the donor site can be directly closed and sutured. The margins of the scar tissue should be removed as far as possible. When there is partial margin necrosis, the suture line should be retained, and the premature removal is avoided, since the suture line can play the role of closing the wound and preventing the expansion of the wound. After the incision disruption, the wound dressing is performed, and the wound heals at the second stage; the large wound after the granulation tissue has grown is repaired with skin transplantation, and the scar tissue can also be removed under the circumstances to make fresh wound, which is sutured directly.
- (5)
Other complications: Other rare complications include:
- (a)
Local effusion under the skin flap: The puncture suction or local drainage can be performed.
- (b)
Scar hyperplasia in donor site: It is common in vertical rectus abdominis myocutaneous flap and rarely occurs in TRAM flap. The treatment is the same as the scar treatment. The scars are removed at the second stage, and the corticosteroid is injected into the scar, and then the silicone gel patch is applied externally.
- (c)
The shape of the reconstructed breast is poor, and it is mainly due to improper method for flap shaping. Different abnormalities should be appropriately adjusted at the second stage.
- (a)
- (1)
1.7.2 Breast Reconstruction with Expanded Latissimus Dorsi Myocutaneous Flap
The traditional latissimus dorsi myocutaneous flap does not carry surrounding adipose tissues and has a small tissue volume; thus, it requires the combined application with breast prosthesis for breast reconstruction, so as to achieve the purpose of being symmetrical to the contralateral breast. The breast prosthesis, as a foreign substance, has complications such as rupture and leakage of the prosthesis and capsular contracture, which have become the focus of attention or discussion. In order to avoid the use of breast prosthesis, Bohme and Hockin proposed the simple application of the latissimus dorsi myocutaneous flap, without the use of breast prosthesis for breast reconstruction, which is adopted by more and more people through continuous improvement. The breast reconstruction with expanded latissimus dorsi myocutaneous flap traditionally refers to carrying the fatty tissue surrounding the latissimus dorsi muscle to be transferred together for reconstruction, and some scholars have recently carried parts of the serratus anterior muscle on this basis, in order to increase the tissue volume for breast reconstruction. The breast reconstruction with expanded latissimus dorsi myocutaneous flap is a good surgical method for medium-sized breasts, especially for oriental females.
Get Clinical Tree app for offline access

- 1.
Partition of the fatty tissue surrounding the latissimus dorsi muscle: Delay (1998) divided the available fatty tissue surrounding the latissimus dorsi into five regions (Fig. 15.11):
Fig. 15.11
Partition of the fat around the latissimus dorsi muscle
- (1)
Region I: It is the tissue located between the skin part of the skin flap and the latissimus dorsi muscle. Any form of latissimus dorsi myocutaneous flap includes this part of the fatty tissue, and blood is supplied by the myocutaneous perforator vessels.
- (2)
Region II: It is the fatty tissue on surface of the latissimus dorsi myocutaneous flap after removal of the skin. Similar to region I, blood is supplied by the myocutaneous, muscle, and fat perforator vessels. The area of this region is large, and the available adipose tissue seems to be thin. In fact, the cumulative tissue volume is very considerable. It is presumed that the area of unilateral latissimus dorsi muscle is 450 cm2, and there is 0.5 cm-thick fat on the muscle surface, the total fat volume can reach up to 225 ml.
- (3)
Region III: It is the scapular fat area and is located on the medial upper margin of the latissimus dorsi muscle. As a continuation of the muscle flap, it can be folded to use, so as to increase the volume of myocutaneous flap. The region travels toward the head side along the medial upper margin of the latissimus dorsi muscle, and blood is supplied by small perforator vessels given off from the latissimus dorsi muscle.
- (4)
Region IV: It is the fat area in the anterior margin of the latissimus dorsi muscle, it is located at 3–4 cm in front of the lateral margin of the latissimus dorsi tissue, and blood is supplied by small perforator vessels given off from the latissimus dorsi muscle.
- (5)
Region V: It is the upper iliac fat area and is located above the iliac crest, also known as love handle, it is a continuation of the lower margin of the latissimus dorsi muscle, and blood is supplied by the muscle and fat perforator vessels of the latissimus dorsi muscle. This region is located in the far end of the skin flap, and the latissimus dorsi muscle is transmigrated into the fascia part in this region, and therefore, the blood supply of this region is weakest.
- (1)
- 2.
Preoperative examination and skin flap design: In addition to conventional examinations on systemic recurrence of the tumor, the situations of the breast at the healthy side and the donor site are the examination key points.
- (1)
Estimation of available back tissues: The index finger and thumb are placed on the anterior margin of the latissimus dorsi muscle, and the skin is nipped up to estimate the thickness of the fat which can be taken advantage of. Attentions are paid to observe the thickness and range of the fat above the iliac crest. The patient with thin back can only provide tissues to reconstruct a smaller breast; the patient with medium-sized body can provide tissues to reconstruct a medium-sized breast, and the patient with hypertrophic back fat can provide tissues to reconstruct a larger breast.
- (2)
Measurement of the function of the latissimus dorsi muscle: The affected upper limb is abducted, and then the examiner holds the affected upper limb with hands and asks the patient to adduct the limb to observe the contraction situation of the belly of the latissimus dorsi muscle. The loss of the contraction function of the latissimus dorsi muscle indicates the thoracodorsal nerve damage, and it also means that the thoracodorsal vessels are damaged. The thoracodorsal vessels are damaged during breast cancer radical surgery; meanwhile, the latissimus dorsi muscle is denervated and atrophic, and the tissue volume of latissimus dorsi myocutaneous flap is reduced; thus, other methods such as TRAM flap should be used for breast reconstruction. The latissimus dorsi muscle with good function means that the thoracodorsal vessels and nerves are intact and undamaged.
There are three methods for skin flap design, namely, the transverse shape, the oblique shape with the outer on the upper part and the inner on the lower part, as well as the oblique shape with the inner on the upper part and the outer on the lower part. The scar of transverse skin flap is covered by bras and the scar is not obvious; thus, the transverse skin flap is more commonly used. The oblique skin flap with the outer on the upper part and the inner on the lower part leads to the longitudinal scar in the back, which impedes the appearance, but is convenient for surgical operations, especially for easy harvesting of the fat in region V. The skin flap design with the inner on the upper part and the outer on the lower part is in accordance with the direction of the dermatoglyph in the back, which is not only convenient for the harvesting of the skin flap but also conducive to the appearance of postoperative scar.
The patient takes a standing or sitting position, and then the lacunas in separation range of the chest and the harvesting range of the fat flap in the back are marked (Fig. 15.12). The flap part presents as crescent shaped and is bent toward the head side. The medial side of the crescent-shaped flap is 3 cm from the midline of the back, and the lateral side reaches the anterior axillary line. The width of the skin flap is about 7 cm, which is appropriate as long as the donor site can be directly closed and sutured. Too wide skin flap has limited increase in fat tissue volume. On the contrary, it will cause serious complications in donor site.
Fig. 15.12
The lacunas in separation range of the chest and the harvesting range of fat flap in the back are marked in the patient in standing or sitting position
The patients take a sitting or standing position, and the preoperative marker lines are made: ① the inframammary fold which is symmetrical to that at the healthy side, ② the contour of latissimus dorsi muscle at the operation side, and ③ design of myocutaneous flap. Firstly, the contour of the bra is roughly marked out on the back, and the oval skin flap is designed at the lower margin of the bra. The skin flap is located in the sarcoplasmic parts at the upper margin of the latissimus dorsi muscle and presents as transverse or oblique shape. The size of the skin flap should meet the requirements for breast reconstruction, and the donor site can be closed and sutured directly. If the skin-sparing radical mastectomy is applied, only a little skin is needed.
- (1)
- 3.
Surgical methods: The patient takes the lateral position with the affected side on top, and the chest scar removal and skin flap separation can be carried out in this position. After disinfecting and draping in surgical area, the affected upper limb is bandaged with a sterile sheet, which facilitates the movement during surgery.
The chest scar is removed, and the lacuna is separated within the preoperative marked range on the surface of the pectoralis major muscle under the skin flap. After the bleeding is stopped, the lacuna is filled with saline gauzes for standby application.
The flap incision is made along the back marking line. After the skin is incised, 0.5 cm-thick subcutaneous fat is retained, and the remaining fat is retained on the surface of the muscle; meanwhile, the undermining dissection of the harvesting area of the muscle and the fat flap are performed. In the process of undermining dissection, a certain thickness of subcutaneous fat should be maintained, and the subdermal vascular network is protected to prevent partial skin necrosis in donor site. Separation is performed on the surface of the muscular fascia at the anterior margin of the skin flap to expose the anterior margin of the latissimus dorsi muscle. The running directions of the blood vessels are confirmed at the anterior margin of the skin flap, and the starting point of the latissimus dorsi muscle is cut off according to the required muscle volume. The skin flap is harvested using the method of from far and near. The separation is carried out in deep layer of the muscle, and the thoracodorsal vessels are included. The myocutaneous flap is lifted up and separated toward the direction of the armpit. The thoracodorsal vessels give off a branch to enter into serratus anterior muscle before entering into the latissimus dorsi muscle. Under special circumstances, when the subscapular vessels are destructed, the latissimus dorsi myocutaneous flap relies on the branch to maintain the blood supply. Therefore, it is required to retain the vascular branch of the serratus anterior muscle as far as possible. Under normal circumstances, retaining the branch does not affect the transfer of the latissimus dorsi myocutaneous flap; if necessary, the surrounding tissues of the vascular branch are appropriately dissociated to increase the length of the branch. On the other hand, even if the subscapular vessels are good, retaining the vascular branch of the serratus anterior muscle is also conducive to the blood supply of the latissimus dorsi muscle. The end point of the latissimus dorsi muscle can be kept intact, partially cut off, or cut off to reconstruct the anterior axillary folds. In general case, it should be cut off completely, so as to prevent deformation of the reconstructed breast due to muscle contractions.
Between two incisions before and after the chest, a subcutaneous tunnel near the armpit is made, and the latissimus dorsi myocutaneous flap is transferred to the chest through this subcutaneous tunnel and is temporarily fixed. The negative pressure drainage tube is placed after both sides of the wound margin of donor site are dissociated, and the direct closure and suture are performed in sequence of the subcutaneous area, intradermal area, and skin.
The patient is adjusted in the supine semi-sitting position, and the flap shaping is performed. The latissimus dorsi muscle is placed in separated lacuna in the front chest, and the skin flap is folded, and then the fat flap is placed under the skin flap. Firstly, the myocutaneous flap is placed near the lower part as far as possible and is fixed with chest muscle, costal perichondrium, and inframammary fold flap, and then the end point of the latissimus dorsi muscle is fixed, respectively, with the medial clavicle and the parasternal line. The muscle flap is fixed with lateral chest wall at the anterior axillary line and is sutured on the fascia of the serratus anterior muscle. When there is partial absence of the pectoralis major muscle, the muscle flap is sutured and fixed with the pectoralis major muscle. The adjustment is made to achieve symmetry with the healthy side. The excessive epidermis is removed, and the drainage tube is placed along the inframammary fold, and then the skin incision is sutured. The protection of thoracodorsal nerve during surgery can reduce the denervation atrophy of muscle in a later period. The volume of the reconstructed breast right after surgery should be slightly larger than that at the healthy side. The pedicle compression is prevented during wound dressing. The upper limb is immobilized for 72–96 h after surgery (Fig. 15.13).
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
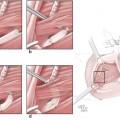 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

