CHAPTER Reconstruction of the scalp and cranium can entail some of the most challenging, sophisticated, and rewarding surgical procedures that comprise a reconstructive surgeon’s practice. Much of the challenge lies in the task of replacing like tissues with like, protecting vital structures, and the myriad options that exist. With any reconstructive procedure, planning entails a precise determination of the tissue components that are or will be missing, the size of the defect, and any anticipated exposure of vital tissues. The surgical goals may vary from closing a wound to reconstructing a part. These goals are modulated by consideration of the patient’s age, existing comorbidities, and wound healing deterrents (e.g., smoking, radiation, infection, previous cranioplasties, and persistent tumor). Successful reconstruction of the scalp demands a detailed knowledge of the unique anatomy that is inherent in this region. For example, the hirsute quality of the scalp with its characteristic quality and density of hair places the remaining, neighboring scalp and its associated procedures (local flaps, tissue expansion) at a premium and vice versa for treatment of alopecia. In the majority of cases, the inelasticity of the scalp prevents primary closure of most wounds, and in such cases, the healing by secondary intention, tissue expansion, skin graft or substitute coverage, locoregional flaps, or free tissue transfer may be indicated to close the wound or defect. However, when the defect is massive, or composite in nature (i.e., with concomitant cranial bone loss), the treatment goals shift toward safe, reliable closure of the defect to protect vital structures with a secondary objective of reconstructing the scalp by restoring a hair-bearing surface in a staged fashion. In the latter scenario of a composite defect, a multidisciplinary approach, with a neurosurgeon and on occasion other specialists, is absolutely necessary. Unfavorable results of scalp and cranial reconstruction can be divided into two broad categories: (1) aesthetic and (2) functional or protective. Unfavorable aesthetics include unsightly scars, contour irregularities, and abnormal qualities of skin, including color, texture, composition, and hair patterns. The function of the scalp and cranium, in addition to appearance, is generally related to protection of underlying structures, and unfavorable results occur when the integrity of the scalp or cranium is compromised. Additionally, the cranium serves to help regulate cerebral spinal fluid and venous pressures of the brain and meninges, and loss of large portions of the cranium may predispose to the syndrome of the trephined. Proper preoperative planning is essential to avoid unfavorable results. When planning reconstruction of any scalp defect, several factors must be considered: • Location and three-dimensional size of the defect • Components of the defect (skin, pericranium or cranium, dura) • Surrounding tissue quality • Age and health of patient • Status of disease (control or palliation) If wound closure is the primary goal, following the sequential steps of the ‘‘wound closure’’ ladder is appropriate (e.g., secondary intention, primary closure, skin graft, locoregional flap, free flap). If the main goal is to reconstruct the defect or deformity, especially in aesthetic reconstruction, the process should not be sequential; instead the best option should be used, even if a more straightforward procedure would work to close the wound.1 Summary Box Unfavorable Results of Scalp and Cranial Reconstruction Aesthetic Functional/Protective • Unsightly scars • Qualitative difference of skin • Contour irregularities – Too thick – Too thin – Shrink-wrap – Denting (loss or thinning of bone) – Protruding (excess or malpositioned bone) • Wound-healing issues – Exposure of hardware, prosthetics, tissue expander, bone grafts or flaps, and dura – Meningitis – Epidural, subdural, or brain abscess • Cranial defect The next consideration is determining the limitations that may preclude obtaining the initial goals and ensuring that the patient, family, and surgeon have realistic expectations. The magnitude and complexity of a scalp defect depends upon a variety of causative factors. They may be full-thickness or partial-thickness in depth and can be classified as congenital or acquired. Congenital defects may include2 cutis aplasia or defects arising from other congenital lesions (congenital nevi, congenital vascular malformations, and congenital tumors). Acquired scalp defects have several possible causes: • Injuries, such as burns • Blunt or penetrating trauma • Avulsion injuries leading to ‘‘degloving’’ of the scalp • Tumor invasion • Infection • Oncologic resection • Radiation • Wound-healing difficulties Preoperative anticipation of potential difficulty with direct closure when the scalp has been compromised by one of these circumstances or conditions is crucial to success. The initial evaluation of the defect is based on its size and location, tissue involved, and structures exposed, such as pericranium, cranium, devascularized bone flaps, prosthetic material, dura, brain parenchyma, or vessels. In addition, the quality of the surrounding tissue (scarring, infection, radiation) and aesthetic concerns such as contour, skin color match, hairline, brow position, and subunits (e.g., forehead) must be considered.3 After assessing the size and location of the defect (or anticipated defect), the structures involved, the surrounding tissue quality, and the patient’s comorbidities, the next step in preoperative planning is to define the operative goal. Is the goal to close the wound or reconstruct the defect? Sometimes these two goals are in sync. If aesthetic reconstruction is the goal, then multiple staged procedures may be needed to obtain the best result. Frequently, wounds are initially closed in the most straightforward way, with the anticipation that secondary reconstruction with tissue expansion or other reconstructive technique will be performed secondarily. In the case of terminal disease, one may adjust the reconstructive approach depending on whether the goal is control or palliation. If tissue quality is poor due to scarring, radiation, or infection and if local options are unavailable or unreliable, then distant tissue is indicated. Sometimes, even if local, less complicated options are technically feasible, they are more likely to have an unfavorable result, because distant tissue is safer and more reliable in ensuring uncomplicated healing.4–6 This approach is especially important if there is exposure of vital structures. It is critical for the surgeon to not only determine the etiology of the defect, but also to identify patients at high risk who therefore have a higher chance of a detrimental outcome. In this regard, it has been our overwhelming experience that previous radiation, previous or concurrent infection, exposed hardware, concurrent cerebrospinal fluid (CSF) leak, previous multiple cranioplasties, and cigarette smoking are deterrents to successful reconstruction of the complex scalp defect.7 In these cases, the complication rate has been noted to escalate to 59% in one study.8 To help guide reconstructive choices in these difficult scenarios and minimize major complications as well as unfavorable results, we have developed a severity scoring system: The University of Chicago CRAnial Severity Score of Hostility (CRASSH)9 (Table 54.1), which serves as a tool for decision-making in the reconstruction of composite scalp–cranial defects. Table 54.1 University of Chicago CRAnial Score of Severity of Hostility (CRASSH)
54
Reconstruction of the Scalp and Cranium
Avoiding Unfavorable Results and Complications in Reconstruction of the Scalp and Cranium
Preoperative Planning and Patient Selection
 Color
Color
 Texture
Texture
 Composition: hair (alopecia)
Composition: hair (alopecia)
 Soft tissue
Soft tissue
 Cranium
Cranium
 Marginal necrosis
Marginal necrosis
 Unstable skin/scar
Unstable skin/scar
 Wound breakdown
Wound breakdown
 Infection – Wound
Infection – Wound
 Superficial
Superficial
 Deep
Deep
 Loss of brain protection
Loss of brain protection
 Syndrome of trephined
Syndrome of trephined
Etiology and Analysis of Defects
Patient Selection
Preoperative factor | Score |
Current or history of infection | 1 point |
Previous radiation | 1 point |
Previous failed reconstruction | 1 point for every event |
Large cranial defect (>60 cm2) | 1 point |
Previous CSF leak | 1 point |
Open wound | 1 point |
History of tobacco use | 1 point |
Source: From Fong AJ, Lemelman BT, Lam S, et al. Reconstructive approach to hostile cranioplasty: a review of the University of Chicago experience. J Plast Reconstr Aesthet Surg 2015;68:1036–1043.
Procedure and Technique Selection
If there is a large cranial defect with reliable soft tissue coverage and a CRASSH score of 0, almost any cranioplasty technique, alloplastic or autologous, will have a low morbidity rate. Similarly, if a patient with unreliable soft tissue coverage has a low CRASSH score, particularly without having a previous or concurrent infection, then a regional, distant, or free flap should be used to provide reliable soft tissue coverage over the cranial reconstruction (alloplastic or autologous). The more complicated the patient’s history regarding high risk for wound-healing issues (i.e., the higher the CRASSH score), the more likely more reliable soft tissue coverage should be used, the less likely alloplastic material is acceptable as a bony substitute, and the more likely autologous bone is the best choice. Patients with the most hostile wounds (CRASSH of more than 3) do best with vascularized autologous bone.
Intraoperative Considerations
Due to its unique nature, the ideal tissue for scalp defect coverage would be adjacent scalp tissue, thereby following the classic tenet to replace like tissue with like. If there is significant damage to surrounding tissue due to trauma, multiple surgeries, infection, or radiation, defect coverage with local tissue may not be the ideal option to obtain reliable, stable wound closure. The goal of wound coverage from a functional and protective standpoint should be combined with the goal of achieving a cosmetically pleasing (or acceptable) result. Often, this goal requires a combination of different procedures and several surgical stages. In order to achieve an optimal aesthetic result, frequently the final revisions (using locoregional flaps, tissue expansion, hair transplantation, flap thinning, or excision of skin paddles or grafts) must be delayed until stable wound coverage is obtained.
Scalp Reconstruction Options
Primary Closure
Classically, the reconstructive surgeon can resort to primary closure with undermining of isolated scalp defects if the defect is less than 3 cm in diameter, especially if the defect is posteriorly located10 (Fig. 54.1). Frequently, post-traumatic wounds have the appearance of tissue loss but, on careful inspection, are found to not be missing any tissue. These wounds can usually be closed directly if minimal tissue needs to be débrided. Limitations of that approach may exist based on the surrounding tissue quality or exposure of vital structures. Maneuvers that facilitate closure, such as local advancement flaps, undermining the tissue, and scoring of the galea11 helps in reducing tension and increases the chances of stable wound coverage. However, the surgeon must be careful to not score too deeply or close under too much tension, both of which will compromise the blood supply and lead to marginal necrosis, wound breakdown, or alopecia.
Secondary Intention
Dr. Frederic Mohs’ initial approach12 of healing small forehead and scalp defects with secondary intention by granulation, contraction, and reepithelialization, can be used and is often applied in the case of paramedian forehead flap donor sites. In the congenital case of cutis aplasia, simple defects can be allowed to close by secondary intention with the application of a topical antimicrobial, and no surgical intervention is needed.13 Although healing by secondary intention frequently leads to acceptable results in patients of Western European descent (Fig. 54.2), patients with darker skin frequently heal with more noticeable hypopigmented or hyperpigmented scars. In the scalp area, the healed defect will be alopecic but will have also reduced in size significantly because of the contraction component of secondary healing.14
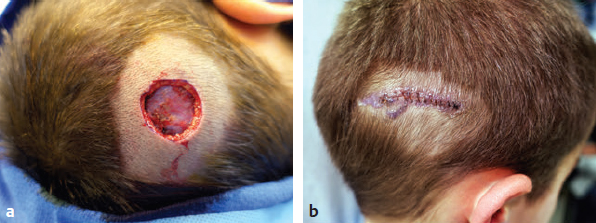
Fig. 54.1 Primary closure. Posterior scalp wound (a) facilitated by loose skin from the neck (b).

Fig. 54.2 Healing by secondary intention. (a) A patient with an open scalp wound referred for closure. (b) One month after treatment with a topical antimicrobial. (c) After 3 months.
Skin Grafting and Tissue Expansion
Skin grafting of the scalp is a relatively straightforward procedure that provides reliable wound closure. Skin grafting of the scalp has several disadvantages:
• Difficulty in matching the color, texture, and thickness of skin
• Suboptimal restoration of the contour
• Lack of hair if used in hair-bearing regions
Patients who are bald and have defects in these non–hair-bearing areas are often best served with a skin graft, whereas defects within the hair-bearing portion are typically aesthetically unacceptable. Color differences can be minimized by harvesting from the scalp. Using hair-bearing scalp has the added advantage of hiding the donor site under hair (when it grows back) (Fig. 54.3). Split-thickness skin grafts typically do not tolerate radiation very well, especially if a significant amount of desquamation occurs from the radiation.3 If adjunctive radiation is anticipated, the surgeon should consider using a fasciocutaneous flap instead; if it desquamates, it has the capacity to reepithelialize.
Robinson (1908)15 was the first to describe that a skin graft can take directly on pericranium rather than waiting for the wound to be covered by granulation tissue first. Another method to be considered when the outer table of the cranium is exposed is to drill burr holes into the diploe, await granulation tissue to cover the bone, then skin graft the granulation tissue. Alternatively, the outer table of the skull can be removed or burred down and a skin graft can be placed directly on the well-vascularized diploe.16 Without the gliding capacity of the pericranium, however, these grafts are often prone to minor wound breakdown. This is also the case in wounds devoid of pericranium that are covered initially with a bilayer wound matrix or acellular dermal matrix, which has gained popularity for scalp wounds of this nature17,18 (Fig. 54.4).
Tissue expansion is certainly an ideal reconstructive option of choice for hair-bearing scalp defects, because no other technique can provide ‘‘like tissue’’ for large defects.19,20 Temporary skin grafting with the anticipation of subsequent removal after tissue expansion of adjacent local tissue from the same aesthetic unit provides a superior cosmetic outcome (Fig. 54.5). The main disadvantages of tissue expansion are the need for multiple procedures, the temporary aesthetic deformity of having expanders, and the lengthy treatment period of several months during expansion, necessitating optimal compliance from the patient and/or caregivers.19,21 The major complications associated with tissue expansion are wound breakdown, extrusion, and infection. Wound breakdown and extrusion can be minimized by placing the incisions perpendicular rather than parallel to the direction of expansion (see Fig. 54.5d), avoiding folds in the expander and avoiding having any incisions overlying the expander, its tubing, and port.19 Another consequence of tissue expansion is the molding or erosion of the skull from the pressure of the expander (see Fig. 54.5i). Although this can potentially lead to disastrous consequences,22 bony contour irregularities caused by tissue expansion generally spontaneously improve with time. To minimize unfavorable results, not only do the previously mentioned issues need to be considered, but the plan of how the expanded flaps will be moved needs to be determined at the time of insertion. Axial transposition flaps will more likely accomplish the goal rather than direct advancement flaps. In addition, because whether expanded flaps will totally cover the defect to be resurfaced cannot be easily predicted, it is prudent to only excise the lesion or scar after ensuring the expanded flap will indeed cover the defect. Otherwise, the surgeon might be tempted to “push” the limits of the flap and compromise its circulation, or areas that cannot be resurfaced with the expanded flap may need repeat grafting.
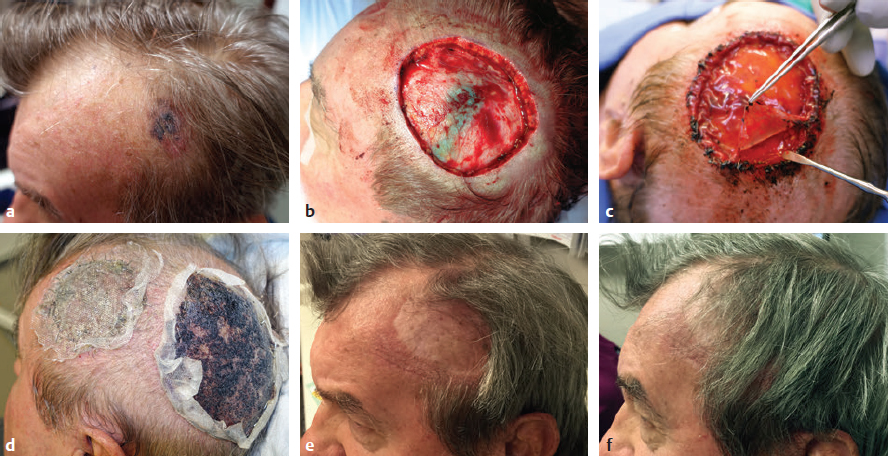
Fig. 54.3 (a) Melanoma of the left anterior scalp. (b) Wide excision. (c) Wound temporized with bilayer wound matrix. (d) Split-thickness skin graft harvested from hair-bearing scalp. (e) Aesthetic deformity of the recipient site and hidden donor site 1 year later. (f) The patient uses a “comb-over” technique in an attempt to hide the aesthetic deformity.
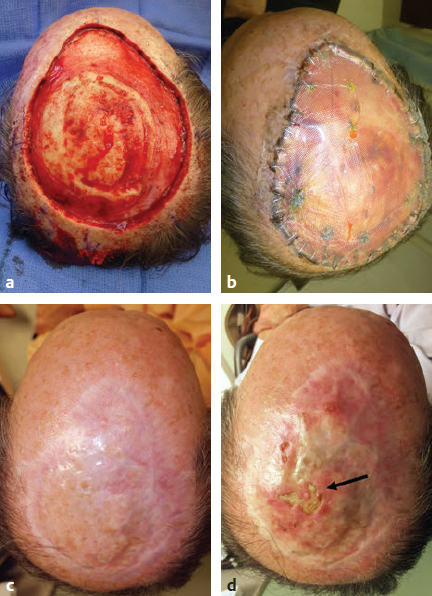
Fig. 54.4 (a) Wide excision of skin cancer with removal of outer table of calvarium. (b) After placement of bilayer wound matrix. (c) Fourteen months after split-thickness skin graft. (d) Minor trauma to adherent skin graft 3 years after placement. Atrophic changes occurred over time.

Fig. 54.5 (a) A burn injury to the scalp of a 2-year-old patient. (b) After tangential excision of burn eschar. (c) The wound was closed with a split-thickness skin graft with significant burn alopecia. (d) Incisions for the expander placement, placed perpendicular to the expander. (e) Hair-bearing scalp was expanded for 4 months. (f) The anterior hairline was marked using a template from the contralateral side. (g) A left transposition flap was incised and the expander removed. (h) The area was “resurface-tested” before excision of the alopecic area. (i) Bone molding was noted under the expander. (j) After resurfacing of the entire alopecic area with expanded hair-bearing flaps.
Locoregional Flap Reconstruction
When considering local flap reconstruction of the head and neck, the surgeon must think in two broad categories: aesthetic subunit reconstruction or nonsubunit reconstruction. There are no separate aesthetic units of the scalp, but there is a clear distinction between the hair-bearing scalp and the aesthetic unit of the forehead. When using scalp flaps, the surgeon must be cognizant of the hairline and avoid distortion of the brow. In addition, the reconstructive surgeon must respect the direction of hair growth. A swatch of hair growing in the wrong direction can negatively affect an otherwise excellent reconstruction. The thick, inelastic nature of the scalp can make local tissue rearrangements (with direct closure of the donor site) difficult. Closure under tension often leads to loss of hair in a widened scar, marginal necrosis, and wound breakdown, which is devastating when underlying hardware is used. To avoid this, when large local flaps are performed, the donor sites frequently need to be skin grafted to minimize tension (Fig. 54.6). Rotation, transposition, or geometric flaps can provide acceptable cosmetic results if the defect is small to moderate size.23,24
Multiple locoregional flaps have been described.25,26 For example, Raposio et al27 described the use of three adjacent rhomboid flaps in the vertex area to reconstruct the natural whorl pattern of the hair in that region. A combination of rotation and advancement is often used to cover larger defects requiring a long curvilinear incision, which incorporates at least one of the named scalp vessels, allowing for maximal excursion while maintaining vascularity.
In geometric terms, the length of the rotation flap should exceed five times the diameter of the defect to get adequate tension-free closure28 (Fig. 54.7). Galeal scoring, back-cutting, and undermining of the scalp in the subgaleal plane can help minimize tension as well. The results of these flaps appear better in hirsute scalps than bald heads, which do not have hair or skin lines to hide the scars (Fig. 54.8).

Fig. 54.6 Local transposition flaps that could not be closed primarily because of tension; a skin graft was placed to close the wound without tension.
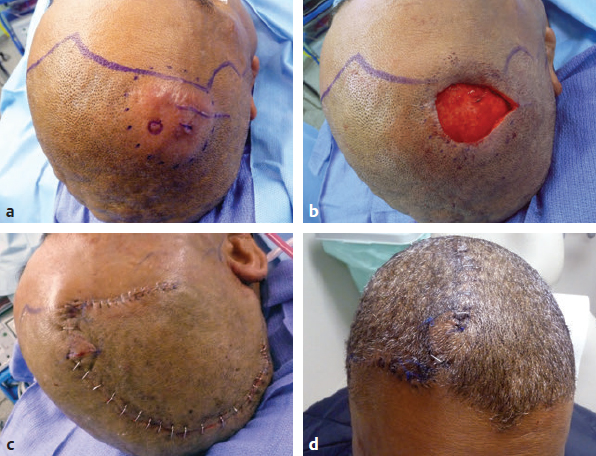
Fig. 54.7 (a) A soft tissue tumor just behind the hairline. (b) After excision. (c) Closure with a large rotation flap to avoid distortion of the hairline or brow. (d) Final result 3 weeks postoperatively.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


