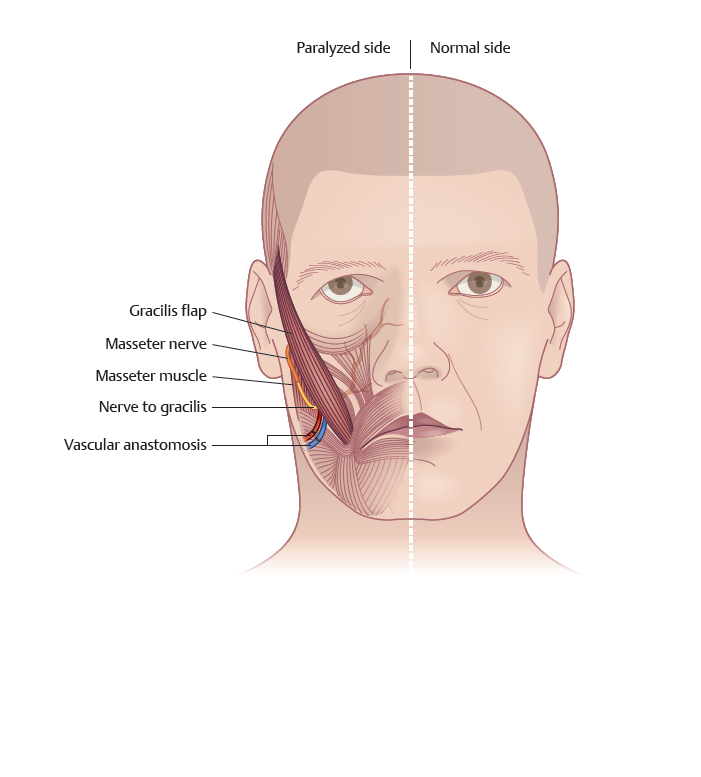
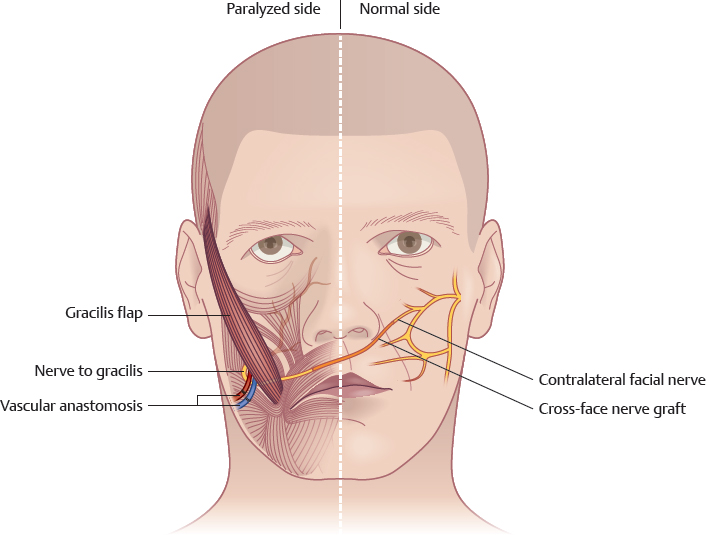
CHAPTER Paralysis of the facial mimetic muscles causes loss of voluntary facial movements, loss of involuntary facial expression, and dysfunction in facial tone. It is a devastating condition with profound functional, aesthetic, and psychological consequences. Symptoms may include ocular dryness and tearing, speech difficulties, oral incontinence, impairment in mastication, and obstruction of the nasal airway. Significant emotional distress is the result of facial disfigurement, impaired communication, and social dysfunction. Facial paralysis manifests as a spectrum of conditions, either unilateral or bilateral, that range from partial to complete weakness. It may be congenital or acquired; acquired conditions include neoplasms, trauma, infection, and iatrogenic and idiopathic causes. Reanimation of the paralyzed face focuses on restoration of form and function. Goals are to achieve protection of the eye, facial symmetry at rest, and voluntary symmetrical facial movement and to restore involuntary mimetic facial expression.1 The most significant unit for reconstruction, from a functional and aesthetic perspective, is the buccal–zygomatic muscle complex (BZMC), responsible for smiling and for the tone of the cheeks. This complex includes the risorius, the zygomaticus major and minor, and the levator anguli oris muscles and is normally innervated by tributaries of the zygomatic and buccal branches of the facial nerve. Significant functional problems are associated with paralysis of the oral musculature, including drooling and speech difficulties. A flaccid lip and cheek can lead to difficulties with chewing food, cheek biting, and pocketing food in the buccal sulcus. However, the main emphasis of surgery is usually centered on reconstruction of a smile. Three elements are required for the formation of a smile: 1. Neural input 2. A functioning muscle innervated by the nerve 3. A proper muscle orientation All three factors contribute to the determination of which reconstruction would be ideal. Reconstructive modalities in dynamic reanimation can be classified by two basic criteria: 1. Whether reconstruction is based on the facial nerve or on a different cranial nerve2 2. Whether the working muscle unit is the original BZMC or a transferred muscle flap3 Facial nerve–based reanimation can be based on an ipsilateral facial nerve, depending on the presence of a functional branch or stump. Duration of paralysis is the principal determinant for the need for muscle transfer. If duration is less than a year, the BZMC is assumed to be viable. Facial muscles become irreversibly atrophic or too weak to work properly by 24 months. After this point muscle transfer is indicated.1 Primary facial nerve repair is possible in cases of recent trauma to the facial nerve. If there is a large gap between the proximal and distal nerve stumps, a sural cable nerve graft is used to interconnect between the stumps of the zygomatic–buccal facial branches with an ipsilateral trunk of the facial nerve.1 In case of recent paralysis in which a functional facial nerve branch is available only on the contralateral face, a cross-face nerve graft is used to relay facial nerve input across the face to the BZMC. Axons from the contralateral facial nerve regenerate through the sheath of the graft. They innervate the muscle over 4 to 6 months.3–5 Because muscle atrophy can develop while the facial nerve regenerates, an ipsilateral motor nerve can be transposed to serve as a temporary innervator (“babysitter”) to the muscle. Thus muscle tone is preserved while waiting for the cross-face grafts to grow across, and spontaneous smiling is restored.1,6 At the first surgery two nerve grafts are connected to the upper and lower trunks of the normal contralateral facial nerve. Then they are tunneled across the face through the upper lip. These nerves are banked in the paralyzed pretemporal region and marked or immediately connected to selected corresponding branches. At that same procedure, a short nerve cable graft is used to connect the nerve to the masseter with the distal stump of the affected facial nerve. Within 2 to 3 months the paralyzed muscle will regain tone and then will begin to function in a mass pattern motion. Sometimes at the same procedure or about 6 to 9 months after the initial procedure,5 at a second surgery, the paralyzed side will be reoperated. The two cross-face nerve grafts that were banked are identified, split into fascicles, and connected to the facial nerve branches distal to the prior masseter–facial nerve repair. Within 3 to 6 months spontaneous facial nerve motion is initiated by the contralateral facial nerve that should take control of the motion. If the masseter nerve action is still noticeable and unsightly, the master branch can be transected. Fig. 56.1 Two-stage cross-face nerve graft and free gracilis muscle transfer. Facial nerve–based reanimation for long-lasting paralysis necessitates both reinnervation and muscle transfer. Various muscles are available for muscle transfer. However, the gracilis muscle is preferable. The neuromuscular pedicle is reliable and relatively easy to prepare. A segment of muscle can be cut to any desired size based on the neurovascular pedicle, thereby making the flap customizable to the patient’s facial proportions. There is no functional loss in the leg, and the scar is reasonably well hidden7 (Fig. 56.1). When an ipsilateral nerve is available, a one-stage free gracilis muscle flap transfer is performed. The flap is inset subcutaneously in the paralyzed cheek from the modiolus to the temporal fascia above the auricle. The blood vessels of the flap are anastomosed to facial or superficial temporal vessels and its motor nerve is sutured to the ipsilateral facial nerve zygomatic branch. When an ipsilateral nerve is unavailable, a two-stage cross-face sural nerve graft and free gracilis muscle transfer is fabricated. In the first stage, the nerve graft is harvested, anastomosed to a contralateral facial branch responsible for smiling stimulus, tunneled across the face to the paralyzed side, and banked in the upper buccal sulcus. In the second stage (which is scheduled 9 months later) the free gracilis is transferred and the motor nerve is sutured to the cable graft that was banked. Reanimation of the muscle commences after 4 to 8 months. It reaches full capacity within a year.3,4 When facial nerves are absent on both sides or the patient is older than 60 years of age and nerve growth is impaired, a non–facial nerve reanimation is performed based on the ipsilateral motor nerve to the masseter nerve that is connected to a free muscle transfer. Thus the stimulus to create smiling movement depends on voluntary actions such as teeth clenching. These efforts may become more natural over time. In this procedure there is no donor nerve morbidity (Fig. 56.2). Patients who are unsuitable or do not wish to undergo a microsurgical procedure may be reconstructed by transfer of a local muscle flap, namely the temporalis or masseter muscles.8 The temporalis muscle procedure usually achieves fair static and dynamic results. However, it does not provide spontaneous smile. Summary Box Unfavorable Results and Complications in Facial Paralysis Reconstruction • Functional damage to the facial nerve on the normal side • Weak contraction and poor smile on the paralyzed side • Worsened state of paralysis • Adhesion between skin and transferred muscle • Deficient transverse smile motion • Bulky cheek • Pronounced facial asymmetry • Unaesthetic muscle tension • Failure to fixate the upper lip muscle • Asymmetrical smile action • Inability to spontaneously operate the muscle and smile • Inability to create total symmetry in bilateral facial paralysis • Postoperative complications During the preoperative planning, the plastic surgeon must remember that facial paralysis patients present with a broad spectrum of signs and symptoms. Thus treatment varies by patient. A thorough history and physical examination are imperative to avoid unfavorable results. The patient’s emotional status, concerns, and expectations, must be determined. For some, attaining a symmetrical appearance at rest is more important than achieving a true dynamic smile. Older patients are more likely than younger patients to be worried about brow ptosis, ectropion and drooping of the cheek with concomitant drooling, deglutition, and impaired speech. Patients who are unable to fully understand the proposed reanimation plan and noncooperative patients are more prone to poor results and dissatisfaction. This is secondarily related to poor compliance. It should be noted that children will have a higher success rate to achieve spontaneous smiling because of their faster nerve fiber growth, brain plasticity, and faster cortical “rewiring” in cases of non–facial donor nerve reanimation. The patient’s general health status must be evaluated; its sustainability for free muscle transfer and reinnervation must be carefully assessed. This includes an assessment of the patient’s ability to undergo a substantial operative procedure under general anesthesia and an evaluation of comorbidities that may affect the fate of microvascular muscle transfer. In facial paralysis reconstruction, a complete symmetry and normal function cannot be totally achieved. However, the procedure can improve functional limitations such as lack of corneal protection, speech problems, drooling, and facial expression. When the effects of the paralysis are subtle, the surgeon must assess the potential benefits to be obtained from surgery, and this is often a function of how severe the paralysis is perceived to be by the patient and an assessment of the impact on the patient’s general well-being. At the same time, it is crucial to address the patient’s expectations and determine whether they are realistic. The patient should be counseled regarding the long time it would take to achieve motion, which is usually around 5 to 12 months. If reanimation is based on a non–facial nerve approach, the patient should be well informed that he or she may not achieve involuntary movement or a truly spontaneous smile nor an identical smile to the contralateral side. Reinnervation progresses slowly in older individuals. However, it is difficult to determine what constitutes “older,” because muscle reinnervation can occur at any age. We are reluctant to perform cross-face nerve grafts on patients who are older than 55 years. Failure to determine the actual etiology of the injury or the time of onset of paralysis may lead to a poor choice of reconstruction modality. For example, if a resection of an acoustic neuroma resulted in incomplete facial paralysis, the reconstructive surgeon should communicate with the neurosurgeon to determine whether the tumor was completely resected and thus whether it may grow back, in which case the ipsilateral facial nerve should not be used as a source for reinnervation, because it may cease to function if the tumor recurs or a secondary procedure is performed on the neuroma. Another example is a patient who had a facial trauma with deep lacerations across the facial nerve anatomy. The surgeon must be able to determine whether there was a concomitant fracture to the base of the skull, which could result in facial nerve injury in and of itself, and thus repairing the nerve at a peripheral location would not improve the paralysis. Physical examination should include the brow motion, the eye, the nasal airway, the mouth, and surrounding structures. The brow’s position should be noted at rest and movement. Visual acuity in each eye should be documented. The height of the palpebral aperture should be measured and compared with the normal side. The degree of lagophthalmos and the presence of a Bell’s reflex will indicate the risk of corneal exposure. The lower eyelid position should be measured and the tone of the lower eyelid should be assessed by the snap test and the position of the inferior canaliculi punctum. In addition, the patient should be examined for corneal irritation or ulceration. The nasal airway is assessed by forced inspiration. A collapsed nostril and drooping of the cheek represent loss of muscle tone. Philtrum deviation, the presence or absence of a nasolabial fold, the amount of commissure depression and deviation, the degree to which the upper lip droops, the presence of vermilion inversion, the amount of bilateral commissure movement, and the upper incisor show when smiling should all be noted. Speech should be assessed. An intraoral examination should include evaluating dental hygiene and the evidence of cheek biting. The presence of synkinesis, the simultaneous contraction of two or more groups of muscles that normally do not contract together, should be documented. The most common types of synkinesis are eye closure with smiling, brow wrinkling when the mouth is moved, and mouth grimacing when the eyes are closed. The level of injury to the nerve, if it is unknown, can be assessed clinically. Injury to the nerve within the bony canal may result in loss of ipsilateral taste appreciation, hyperacusis, and facial weakness, because the chorda tympani and nerve to the stapedius may be injured at this level. Injury to the seventh cranial nerve near the geniculate ganglion will also result in decreased secretory function of the nose, mouth, and lacrimal gland. Fig. 56.3 (a) Before reconstruction. (b) After the reconstruction, the heavy face and cheeks make it hard to notice the underlying muscle motion. An assessment of other cranial nerves, particularly the fifth if it may serve as a donor nerve, is also preformed both to assess added morbidity to the facial paralysis and for possible donor motor nerves. Performing cranial nerve transfer using the same nerve on the contralateral side with absent or weak function may result in a devastating disability in jaw motion if the masseter nerve was used or with tongue function if the hypoglossal nerve was used. Missing the presence of thick skin and fatty cheeks creates a higher risk for unsatisfactory outcome, because there is a higher probability that muscle motion would go unnoticed under the bulky soft tissue and skin (Fig. 56.3, Video 56.1). The first stage of the procedure involves dissection of the facial nerve on the unaffected side through a preauricular incision with a very short submandibular extension. When preparing the nerves, the surgeon meticulously identifies and individually stimulates nerve branches with a nerve stimulator to map their action. The most devastating error at this stage is a functional damage to the facial nerve on the normal side. Fortunately this catastrophic complication is unlikely, because there are typically two to four branches that activate the BZMC, and the sacrifice of one of these branches does not generally interfere with the final function of muscles in the normal side. However, to avoid this possibility, the most dominant branch, which creates the strongest contraction while stimulated, should be used. For this a light amplitude of stimulation should be used (nerve detector set to 0.5 mA), because with stronger stimulation, the current can pass to other branches through the surrounding tissue, stimulate them, and create a stronger contracture than the specific branch may create. Careful examination of the patient’s smile pattern preoperatively, especially in congenital conditions, may reveal that the acting group of smile muscles is limited in its action or that only the zygomaticus major or minor is functioning. In such cases, extra caution should be taken not to use the single nerve branch to that muscle and rather to choose another donor nerve or, with extreme caution, split the main functioning nerve. Facial nerve mapping clearly identifies which nerve fibers stimulate the orbicularis oculi and the orbicularis oris or lip retractors. When stimulated, the facial nerve branches that produce a smile and no other movement are selected. If the nerve that was chosen simultaneous to creating a smile also activates the nostril or the eyelid, the future formed smile on the paralyzed side will be activated by normal-side blinking or by normal-side nostril motion. When this happens, eyelid closure or unsightly motion shows on the normal side when trying to create a smile (Fig. 56.4, Video 56.2). Fig. 56.4 Before (a) and after (b) an unintentional use of a nerve branch that activated the nostril to create a smile. Also, if the branch that is chosen is too small and carries a small number of functioning axons, an unnoticeable weak contraction and a poor smile will show on the paralyzed side. The sural nerve is the usual donor nerve. It is harvested with the use of a nerve stripper. Stripping of the nerve does not appear to affect its function as a graft.9 The proximal ends of the donor facial nerve branches are sutured to the distal end of the nerve graft such that regenerating axons will travel in a distal-to-proximal direction down the graft to prevent them from diverging into side branches and not reaching their target. The current practice is to use a short nerve graft, approximately 12 cm in length, and to bank the free end in the upper buccal sulcus. A shorter nerve graft achieves stronger muscle contraction and at a shorter time (around 6 months). Placing a longer nerve graft may delay the time for a second stage procedure, and its potential “power” may be decreased. In the second stage the gracilis muscle flap is harvested and transferred to the affected side. For incomplete facial paralysis, during that stage the inset of the muscle on the affected side may lead to an injury to the nerve branches responsible for the residual motion and possibly lead to a worse state of paralysis. Another possible error when dissecting the cheek and preparing the recipient side is subcutaneous dissection of the cheek flap that is too superficial, which may later lead to adhesions between the skin and the transferred muscle (Fig. 56.5, Video 56.3). When preparing the recipient blood vessels, a dissection that is too short may result in a need to place the transferred muscle in a less-favorable orientation. Thus a deficient transverse motion may be created rather than an oblique smile. When harvesting the gracilis muscle, special attention should be taken to prevent an injury to the motor branch. This can occur in some anatomical variations in which the motor nerve that usually inserts into the muscle, together with the vascular bundle, leaves the bundle for several millimeters to 1 cm before arriving at the muscle belly. Such an error may cause total failure of the procedure. Another unfavorable result comes from a muscle harvest that is too bulky, resulting in a cheek that is bulky and pronounced facial asymmetry. To achieve an appropriately thin cheek, the muscle is split longitudinally (about one third to one fourth from its cut surface area), and the anterior portion of the muscle is used. While dissecting that tiny strip from the muscle, the surgeon must ensure the neurovascular bundle enters into that segment and that a good contraction can be created by the nerve stimulator. To determine which segment of the muscle to harvest, the surgeon should assess where the neurovascular bundle enters the muscle, so when the muscle flap is set in place the neurovascular bundle is not too far from the planned nerve anastomosis. Attaching the muscle to the modiolus–oral commissure is a critical step of the procedure. It is usually sutured using three to four 0–0 Vicryl sutures inserted into the fibrotic remnants of the paralyzed orbicularis oris muscle. One suture connects to the commissure, two along the upper lip, and one below the commissure. Preoperative smile analysis determines the points of insertion. The surgeon must be careful not to position the perioral sutures too superficially, a condition that will lead to unaesthetic indentations on the skin and lip eversion with every muscle contraction and with smiling. Correct insertion of the muscle also allows a noticeable nasolabial crease. Failure creates facial asymmetry with no nasolabial fold (Fig. 56.6, Video 56.4).
56
Facial Reanimation Surgery
Reconstructive Considerations
Avoiding Unfavorable Results and Complications in Facial Paralysis Reconstruction
 Bleeding
Bleeding
 Infection
Infection
 Thrombosis
Thrombosis
 Vascular compromise to muscle flap
Vascular compromise to muscle flap
 Incorrect muscle positioning
Incorrect muscle positioning
 Excess bulk
Excess bulk
Preoperative Planning and Patient Selection
Errors in History Taking and in Communicating with the Patient
Errors Resulting from Improper Physical Examination

Errors During Surgery
Facial Nerve–Based Reanimation for Long-Lasting Paralysis

Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine