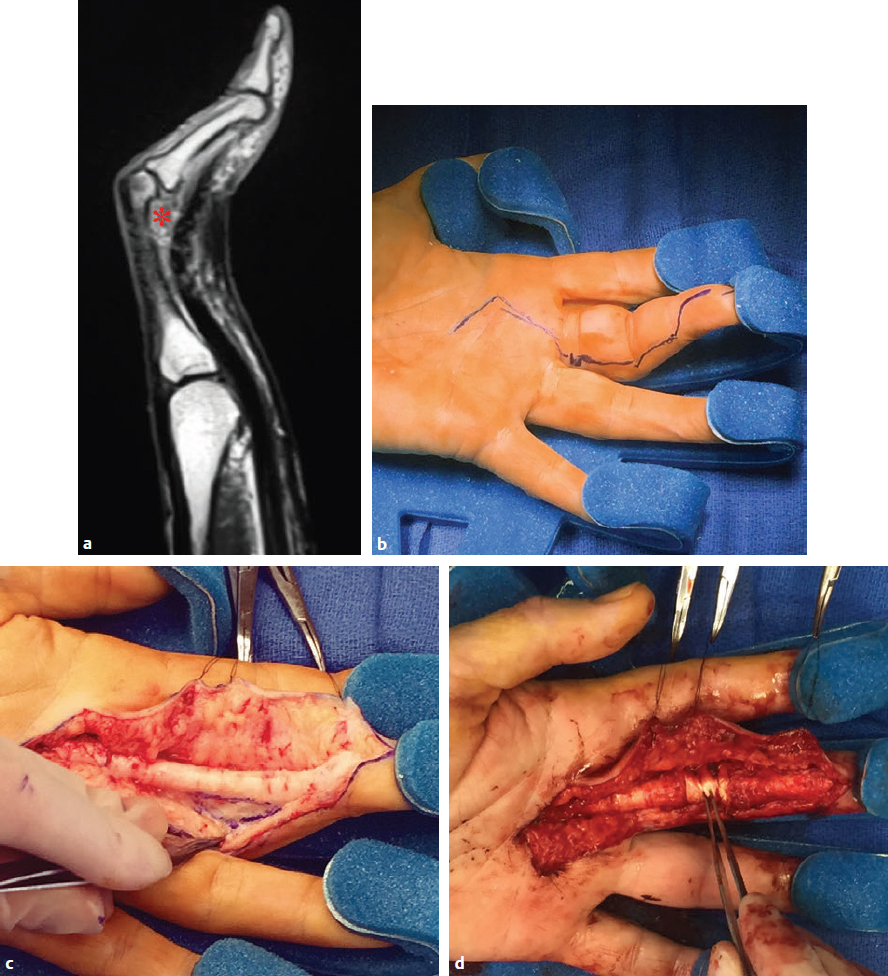
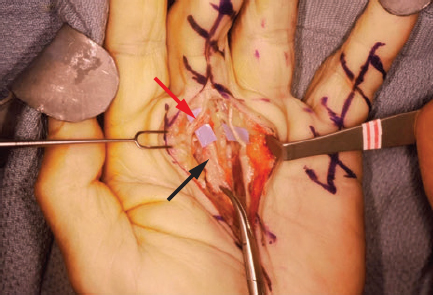
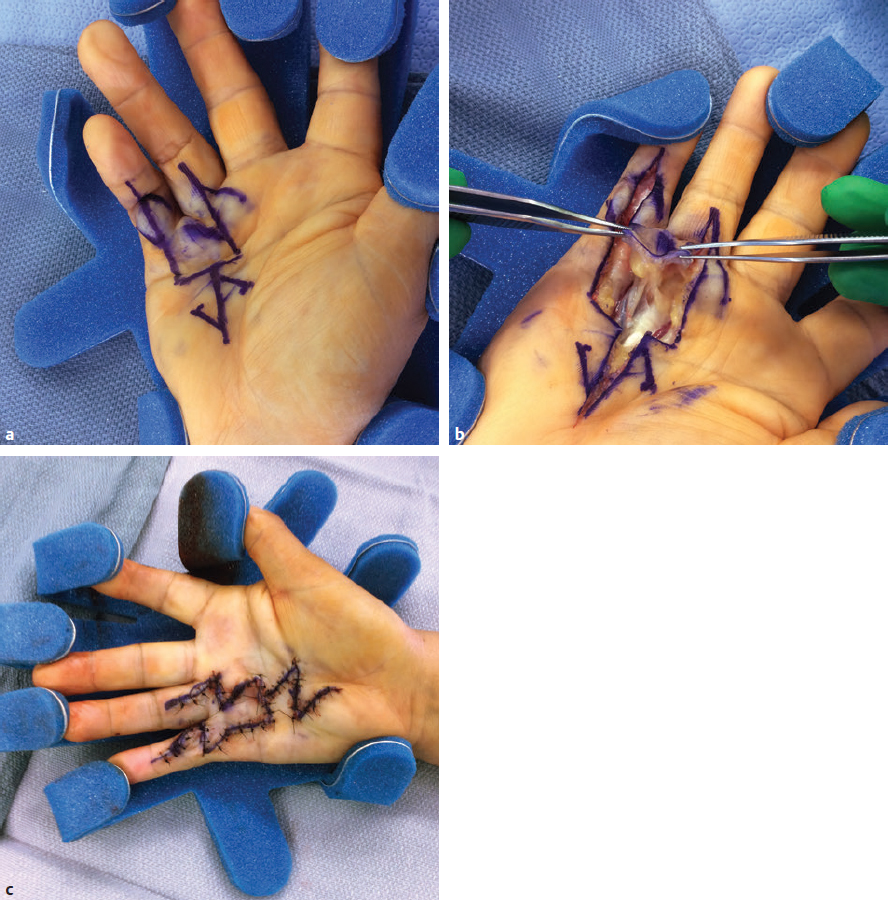
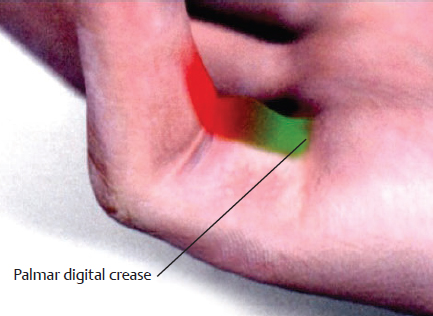
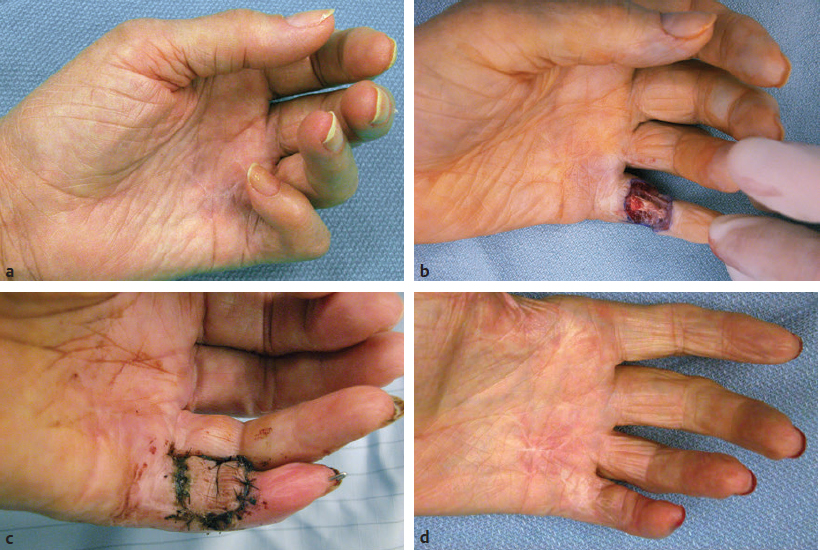
CHAPTER Although it is important to discuss the demographics and natural history of any disease, it is especially essential to do so with Dupuytren’s contracture or Dupuytren’s disease for risk assessment and potential avoidance of complications. These two terms refer to the same condition and may be used interchangeably. Dupuytren’s disease is a benign fibromatosis of the palmar digital fascia that has an autosomal dominant inheritance pattern with variable penetrance.1 Northern Europeans are more commonly affected than any other group, spawning nicknames such as “Viking’s disease” and “Celtic hand,” but all races and ethnicities have reported cases.2 Incidence is approximately 4% in the United States but is as high as 30% in Northern European countries.3,4 Dupuytren’s diathesis refers to a subset of patients with poor prognosis and a high risk of disease progression and recurrence. It was originally described by Hueston5 as individuals of Western European ancestry with a positive family history, bilateral involvement, and ectopic lesions. It was modified to include male gender and age at onset of younger than 50 years.6 The pathogenesis of Dupuytren’s disease can be divided into three stages: (1) proliferative, (2) involutional, and (3) residual.7,8 Formation of nodules begins in the early cellular proliferative stage. As disease progresses to the involutional stage, the nodules decrease in size and myofibroblasts predominate and follow lines of tension, which create cords. During the residual stage, nodules may completely disappear, and the fibrous cords thicken. Myofibroblasts largely disappear, leaving behind a hypocellular collection of type I and type III collagen. This third phase is when significant contractures may develop, and intervention may be required. The ring finger is most commonly involved, followed by the little finger, thumb, long finger, and index finger.1 The timing of intervention is an important consideration, because Dupuytren’s contracture follows an unpre dictable, fluctuating clinical course.1,9 With minimal joint contraction, cords may not be fully developed, and the extent of the disease may not have manifested. Operating early in the disease process can actually result in a postoperative contracture greater than the initial presentation.9 However, delaying treatment can also result in a severe contracture that may not be salvageable. The general consensus for intervention of Dupuytren’s contracture is metacarpophalangeal (MCP) joint contracture of 30 degrees or greater, or proximal interphalangeal (PIP) joint contracture of 20 degrees or greater with progression.1 The final consideration, which may prompt earlier treatment, is a patient with functional disability who is unable to carry out activities of daily living or recreational activities. The three primary treatment modalities currently used are fasciectomy, needle fasciotomy, and collagenase injection.10 Having the knowledge of the available methods along with their benefits and limitations is necessary to advise patients on the treatment plan most suitable for them. Patient comorbidities, occupation, lifestyle, and pattern of disease should all be taken into consideration. A healthy business executive with a busy travel schedule who presents with a single precentral cord is likely offered a different treatment option than a patient with multiple comorbidities who has diffuse palmar disease and multiple digit involvement. Fasciectomy can further be classified as open fasciectomy, dermofasciectomy, open palm fasciectomy, partial fasciectomy, and segmental fasciectomy.1 The traditional open fasciectomy is the excision of both normal bands and pathological cords. The aim of this approach is to prevent recurrence by excising fascia that may have the potential of developing into pathologic cords. This method is not commonly used and is outdated because of the high morbidity and no significant reduction in recurrence rates. Dermofasciectomy involves excision of the diseased fascia and the overlying skin with subsequent skin grafting.1,11 It was believed that the skin graft decreases the chance of recurrence by serving as a division between diseased and nondiseased fascia. The utility of this procedure is primarily in patients with recurrent aggressive disease and associated skin involvement or shortage. The open palm technique originally described by McCash12 is the excision of involved fascia through a combined transverse palm and zig zag finger incision with subsequent closure of the digital incision only. Most hand surgeons practice a modification of the McCash technique by leaving partial wounds open to avoid closing incisions tightly and compromising skin flap vascularity. The open palm technique remains a treatment option for diffuse palmar disease and multiple MCP contractures.13 Leaving the transverse incision open avoids skin grafting and allows for immediate active range of motion. Partial fasciectomy has long been the mainstay of surgical treatment for more severe contracture.1,10 Only the diseased fascia is removed under skin flaps. It is the treatment of choice for multiple digit involvement and recurrent Dupuytren’s contracture. Segmental fasciectomy is performed through multiple small transverse incisions, removing only segments of the cord to release the contracture while leaving behind the intercalary fragments. Its use is less common but it has the benefit of minimal surgical dissection and scarring.1 Needle fasciotomy can be performed in an office setting or outpatient treatment room without the need for sedation or tourniquet use, and the hand is prepped with antiseptic solution.14,15 Multiple portals should be marked longitudinally over the cord at a minimum of 5 mm apart. The procedure sequence is usually from distal to proximal portals. After injecting local anesthetic at the portal sites, a 25-gauge needle with the bevel oriented perpendicular to the cord fibers is used to pierce the skin through the dermis. A transverse fasciotomy is performed by sweeping the needle from side to side, advancing deeper with each sweep until the cord is fully released. The contralateral hand should be used to palpate the cord and apply gentle traction and passive extension of the finger. Multiple fasciotomies are performed at the portal sites until disruption of the cord is appreciated. Strenuous grip activities are avoided for 1 week. Postoperative therapy is usually not needed. Collagenase Clostridium histolyticum is a newer FDA-approved treatment for Dupuytren’s contracture.16,17 The two metalloproteinase enzymes work on all types of collagen, while sparing type IV collagen. Type IV collagen is prevalent in basement membranes of neurovascular structures, which offers the benefit of preserving arterioles, nerves, and epithelium with collagenase injection.17 Up to two separate cords can be injected simultaneously with reasonable efficacy. The 0.58-mg dose is diluted per specifications based on the site of injection and injected directly into the cord. The patient usually returns within 24 hours for gentle passive extension of the finger to initiate cord rupture. Patients should then be fitted for a nighttime splint to be worn for up to 4 months to maintain finger extension and instructed to perform finger extension and flexion exercises during that time. Summary Box Common Complications in Dupuytren’s Contracture Intervention • Neurapraxia and digital nerve injury • Skin necrosis and skin tears • Joint and scar contractures • Recurrence and disease progression • Complex regional pain syndrome and flare reactions • Flexor tendon transection and rupture Managing patient expectations before surgery is the first step in managing complications.1 Patients should be educated on the cause of Dupuytren’s disease and the possible recurrence and progression of the disease after correction. They should have a clear understanding of the expected outcomes and the limitations of the treatment, especially in the presence of substantial PIP contracture. The importance of the recovery period needs to be understood by the patient, because optimal functional outcome is dependent on the patient’s rehabilitation effort. Fig. 68.1 A spiral cord (black arrow) is clearly identified during fasciectomy of the middle finger Dupuytren’s contracture. Note the displacement of the digital neurovascular bundle (red arrow) by the spiral cord. To minimize the risk of neurovascular injury, the surgeon needs to have a thorough understanding of the anatomy. Proximal to the distal palmar crease, the digital nerves remain deep to the transverse fibers of the palmar fascia and can be dissected with assurance that the nerves do not wind around it.18 However, beyond the level of the distal palmar crease, the nerves can sharply turn over the top of the band and create a potential for injury. Normal fascial bands in the hand become cords when they are pathologically thickened and contracted.8 Recognition of the different types of cords is helpful to the dissection and prevention of accidental nerve injury10 (Fig. 68.1). Spiral, lateral, and abductor digiti minimi cords are known to displace the neurovascular bundle (NVB) superficially and to the midline. In the presence of a spiral cord, the structure first encountered at the digital flexion crease is often the NVB rather than the fascia of the cord.1 Dissection of the NVB should be started in the palm where the cords coalesce and followed to the palmar digital junction.1,18 Fasciectomy can be initiated by transecting the cord at the level of the superficial arch. It is found that release of the cords in the palm may help to partially correct the contracture and facilitate the dissection into the digit. If a digital artery injury is suspected, digital perfusion through the other digital artery should be evaluated by release of the tourniquet before skin closure. Vasospasm is the more common cause of transient digital ischemia.10 It is recommended to flex the finger to relieve traction, wrap the finger with warm saline-soaked sponges to improve capillary refill, and apply topical lidocaine or papaverine in the wound to facilitate smooth-muscle relaxation.19 Sufficient time should be allowed for interventions to work before formal exploration, because early dissection will further aggravate the vasospasm. Nerve injuries associated with needle fasciotomy are minimized with intradermal anesthesia because of preservation of sensory feedback.14 Patients should be assessed for fingertip sensitivity before and after local anesthesia and frequently throughout the procedure. Assessment of the skin overlying the cord may be helpful to prevent digital nerve injury. At the level between the distal palmar crease and the proximal digital crease, a spiral cord may be present that can cause medial and volar displacement of the neurovascular bundle.20 Unless the overlying skin is directly adherent to the cord, which would minimize the risk of an interposed digital nerve, caution should be taken at this level during needle fasciotomy. A Doppler examination should be performed if a spiral cord is suspected.14 Areas of identified Doppler tones should be marked to indicate where portal sites should be avoided. Injury to both digital arteries with needle fasciotomy is rare and preventable with thorough knowledge of the anatomy.10 Preoperative assessment of the quantity and quality of the skin is essential for incisional planning and wound closure. Skin necrosis is the most feared complication and is usually related to devascularization of a flap or to wound closure under tension.21 Rather than risking wound closure under excessive tension or using questionably viable flaps on exposed tendons, the central palm wound may be left open to heal by secondary intention. In the fingers, a midline longitudinal incision with z-plasty closure is preferred.21 The midline longitudinal incision ensures that the pedicle of the flap does not lie within the watershed area. Multiple z-plasties are advised to distribute tension and to provide a greater gain in length compared with a single z-plasty. When raising the skin flap, as much fatty subdermal layer as possible should be preserved to prevent vascular compromise (Fig. 68.2). However, if there is deep dermal involvement by Dupuytren’s disease, this may not be possible. Z-plasty should be avoided at the skin crease if possible, because this area often has minimal subcutaneous fat18 (Fig. 68.3). When there is skin shortage or potential for excessive tension under closure, alternative options may be to leave the wound open, skin graft, use a rotational flap, or even to use a heterodigital or cross-finger flap. Fig. 68.2 (a) Incision design with z-plasty flaps for contractures to adjacent fingers can only be safely performed if undermining is avoided and deep blood supply is preserved in critical areas. (b) By preserving perforating blood supply to this distally based flap and adjacent z-plasties, viability to skin flaps is ensured. (c) Tension-free closure is accomplished. Before wound closure, the tourniquet should be deflated to evaluate for flap viability and hemostasis.21 Evaluation for adequate hemostasis is important, because development of postoperative hematoma under the thin skin flaps can compromise flap viability. If uncertain about hemostasis, the surgeon may consider leaving the palmar incision open or placing a small, flat, soft drain. Skin tears are the most common complication, and it is not always possible to avoid them.20 Flexion creases are prone to skin tears and should not be used for portal sites.14 Places with redundant, mobile skin are the best areas for fasciotomy portals. At areas with nodular skin involvement, Eaton22 recommended dispersing the tension by using more portals, deferring definitive stretching until multiple portals have been released, and pushing on adjacent skin toward the firm area to protect it from the overall stretch. If a portal is beginning to tear, the surgeon might avoid further extension if it will propagate to an unmanageable wound. Fig. 68.3 The z-plasty should start with a midvolar longitudinal incision, because this lies in the “safe-zone” watershed area between the two digital arteries. Although a z-plasty as drawn by the solid line does not result in the transverse limbs being in the digital flexion crease, this may be a safer design than that created by the dotted lines because the thinnest part of the flap is then at the flexion crease directly across the base of the flaps. It is unnecessary to preferentially have the z-plasty flaps traverse precisely into the flexion creases. Skin tears are often sustained during a finger extension procedure. It is most common with MCP contracture greater than 50 degrees, especially if the skin overlying the cord is calloused.16 Meals and Hentz16 outlined a sequential four-step manipulation technique to minimize skin tears: 1. Flex the PIP joint while extending the MCP joint. 2. Flex the MCP joint while extending the PIP joint. 3. Extend both joints together. 4. Press on and disrupt any residual intact cords while keeping the finger extended under moderate tension. These steps can be repeated several times if necessary. If a skin tear is imminent, the surgeon may consider stopping and performing gentle passive progressive extension (Video 68.1). A clear understanding of the anatomical structures surrounding the interphalangeal (IP) joints is necessary to minimize persistent flexion contracture or lack of complete extension after fasciectomy.23 Curtis23 lists several mechanical factors that may limit the extension of the IP joints: • Inadequate skin over the volar surface of the finger • Fascia contractures within the finger • Contracture of the flexor tendon sheath within the finger • Contracted flexor muscles or adherent flexor tendons • Contracture of the volar plate • Shortening of the oblique retinacular ligament • Adherence of the accessory volar ligament to the neck and condyle of the proximal phalanx If there is greater than 30-degree residual PIP joint contracture after thorough resection of the involved fascia and flexor tenolysis, a volar plate release can be performed.23 If extension still cannot be obtained after volar capsulotomy, the oblique retinacular ligament can be excised on either side of the PIP joint. The surgeon may even make a conscious intraoperative decision not to perform volar release on any PIP joint contracture of less than 30 degrees, because many will relapse24 (Fig. 68.4). Final extension may then be accomplished with postoperative therapy. Fig. 68.4 (a) This patient with a little finger proximal interphalangeal (PIP) flexion contracture required not only fasciectomy but also volar joint release. Intraoperatively, the finger was able to gain full extension. (b) Postoperatively, the patient demonstrated full flexion of the fingers, but (c) the PIP joint remained painful and swollen. The PIP flexion contracture relapsed to 30 degrees. (d) In contrast, a patient with a similar little finger PIP flexion contracture did not require PIP joint release and was able to reach full extension by fasciectomy alone. Full postoperative flexion (e) and extension (f) was maintained. The morbidity commonly associated with joint release was avoided. Flexion deformity can occur if there is an imbalance of force between the extensor and flexor tendon. Powerful flexors readily overcome the chronically stretched and weakened extensor tendons of Dupuytren’s contracture and draw the finger into flexion.25 A nighttime extension splint may be required to correct the flexion deformity. A recent systematic review concluded that there is no efficacy in routine postop erative night splinting and that it is only indicated with early recurrent contractures.26 Flexor tendon bowstringing can also be a cause of flexion deformity because of the greater force applied by the flexors when important pulleys are accidentally resected during dissection.27 This reinforces the importance of finding the precise plane between the deep fascial dissection and the flexor sheath. Recurrence of flexion contracture, whether in a previously operated area or outside the surgical zone, does not necessarily indicate inadequate primary excision.28 It can represent a local progression of the disease or new disease in fascia outside the original operated area. Recurrence rates for each procedure vary greatly in the literature.29 The reason for this inconsistency is related to a lack of standard definitions of recurrence and a time point for reporting recurrence. A recent systematic review identified the range of recurrence rates to be 12 to 39% for fasciectomy, 50 to 58% for needle fasciotomy, and 10 to 31% for collagenase.30 Current available treatments are intended to release contractures rather than treat the underlying pathology; therefore recurrence is not unexpected and prevention is often not possible.1 Accurate identification of disease severity and careful preoperative planning is key to reducing further morbidity. Presenting contracture severity and number of involved digits are both correlated with complication rates and subsequent recurrence.30 Understanding of the disease prognosis will help to select which treatment options will be effective and be able to provide long-term benefit. An elderly patient with a single, palpable cord causing MCP joint contracture may benefit from a trial of needle fasciotomy or collagenase injection. Dupuytren’s diathesis may rather benefit from partial fasciectomy, because there is greater initial correction and lower recurrence rates compared with needle fasciotomy and collagenase injection.5,30 CRPS is more commonly reported after fasciectomy compared with needle fasciotomy and collagenase injection. It is also more prevalent in females.30 Diagnosis relies on clinical assessment, because there are no reliable or specific tests.31 It should be suspected in patients reporting pain out of proportion to what would be expected from the inciting event or that lasts beyond the average healing time for the injury. Individuals should be referred to a specialty pain clinic early for initiation of appropriate medications.10,31 Because it is difficult to identify the patients who will develop CRPS, it is recommended to take precautions in all patients during the perioperative period.32 Measures such as elevation of the hand to prevent swelling and providing adequate analgesia to minimize pain and anxiety should be applied. For patients who have severe disease and will require an extensive operation, it may be helpful to admit patients to the hospital after surgery for better postoperative pain control. The surgical management of coexisting Dupuytren’s disease and carpal tunnel syndrome was first studied by Nissenbaum and Kleinert33 in 1980. They reported an 87% complication rate in 15 patients who were treated with simultaneous carpal tunnel release and fasciectomy. Gonzalez and Watson34 later reported that there was no significant difference in complication rates in the combined group compared with fasciectomy alone. They recommended these two procedures be performed concomitantly when indicated to avoid an extra operation and progression of symptoms. A recent survey to the members of the American Society for Surgery of the Hand (ASSH)35 concluded that controversy remains among hand surgeons regarding this issue. A comparison of reported data on CRPS and stiffness did not find an increased rate of these two complications. Consequently, they concurred with the recommendations of Gonzalez and Watson. Postoperative extension splinting has been traditionally applied after fasciectomy to prevent recurrent joint contractures during the healing process. Studies have found that sustained tension to the healing tissues may promote local reactive changes, leading to excessive scar formation and flare reaction.36 Patients who exhibit flare reaction initially have a normal postoperative course followed by symptoms of pain, erythema, and stiffness during the third to fourth week after surgery. When placed in postoperative tension-free splints, the incidence of flare reaction was lower. It has been proposed that the mechanical stress on vessels causes decreased lumen diameter, which limits the oxygen delivery to tissues and promotes continued fibroblast formation, scarring, contracture, and possibly sympathetic flare. It was also found that delaying joint extension in the early wound-healing phases with tension-free splinting did not result in loss of motion gained from surgery.36 Flexor tendon injury is a rare complication after needle fasciotomy.10 If there is a suspicion that the needle is in the flexor tendon, a small amount of passive motion at the distal interphalangeal joint is applied to evaluate for movement of the needle with fingertip motion.14,15 If movement of the needle is observed or if the patient reports pain or paresthesia, the needle should be withdrawn and repositioned (see Chapter 61). Rare flexor tendon ruptures have been reported after collagenase injection to cords at the PIP joint of the little finger.37 Several modifications are recommended to avoid tendon ruptures. Before injection, the cord is palpated for the proximal and distal end to identify the midportion where the cord is maximally separated from the underlying tendon.16,17 The needle is then inserted in that area and care is taken to ensure that the needle does not go through the cord. For central cords, it is recommended to not inject more than 4 mm distal to the palmar digital crease and to insert the needle in a horizontal or coronal plane. For PIP joint contractures, it is advised to insert the needle close to the palmar digital crease and no more than 2 to 3 mm in depth (see Fig. 68.4). Many patients complain of numbness after surgery that is usually caused by digital nerve traction during dissection. This results in sensory neurapraxia, which is a transient nerve conduction block that typically improves within 6 to 12 weeks.38 A systematic review of outcomes for Dupuytren’s contracture reported neurapraxia occurring in 0.4 to 52% of cases with partial fasciectomy and 2 to 3% of cases with needle fasciotomy.30 Patients should have close follow-up, and if symptoms persist with no clinical improvement, they may benefit from appropriate diagnostic workup and possibly exploration.10 The incidence of digital nerve division ranged from 2 to 5% of cases with partial fasciectomy and in 0.4% of cases with needle fasciotomy.30 Digital nerve laceration should be repaired to improve sensation and to prevent persistent painful neuroma.32 End-to-end tension-free nerve coaptation remains the treatment of choice.39 When this is not feasible, a conduit can be used for gap lengths less than 10 mm and nerve graft can be used for longer gap lengths. Skin necrosis was reported to occur in 4.3 and 11.1% of patients undergoing fasciectomy for primary and recurrent Dupuytren’s disease, respectively.40 Small areas of skin necrosis will likely heal spontaneously and can be left open if there are no exposed tendons.41 Patients are encouraged to maintain active finger range of motion during the wound-healing phase, even in the presence of an open wound. A very large area of skin necrosis may result in slower healing, infection, or scar contracture. The surgeon may then need to perform an excisional débridement of the necrotic area and repair the defect with possible skin graft or flap. Fig. 68.5 The green zone indicates the safe area to inject a cord affecting the proximal interphalangeal (PIP) joint of the little finger. The red zone shows the danger area near the digital PIP joint crease where potential tendon rupture can occur if the needle is inserted. Skin tears are common after needle fasciotomy and collagenase injection, with rates ranging from 9 to 25% and 9 to 15% of cases, respectively.40 Fortunately, most skin tears heal uneventfully by secondary intention, even when accompanied by a small area of exposed flexor tendon. Avoidance of tendon desiccation is achieved by application of medicated ointment two times a day and wrapping the wound with an adhesive strip bandage until the skin edges are approximated by secondary healing.15 Skin tears rarely need to be closed primarily or require skin grafting. Minor bleeding is not uncommon, and patients are advised to apply gentle pressure, change the dressing as needed, and continue full active finger range of motion during the wound-healing phase. Joint contracture after fasciectomy has been reported to occur in 6.7% of cases and predominantly involves the PIP joint.40 PIP joint contracture may be secondary to extrinsic causes such as skin contracture or diseased palmar-digital fascia.38 The patient in Fig. 68.5 had multiple prior Dupuytren’s contracture releases to the little finger and developed a significant scar contracture. He had a large soft tissue deficit after scar excision that required local tissue rearrangement with multiple z-plasties and an arterialized heterodigital flap from the left ring finger to the palm. PIP joint contracture can also be related to an intrinsic source, such as adhesions to the flexor sheath, tendons, volar plate, or collateral ligaments.38 Intrinsic joint release is an option for a severely contracted PIP joint that is not corrected by fasciectomy alone. As previously mentioned, it is acceptable to not perform volar capsulectomy for PIP contractures of less than 30 degrees, because these will likely relapse.24 Severe, dysfunctional contractures may require salvage procedures such as PIP joint fusion or even ampu tation. The patient in Fig. 68.6 previously had Dupuytren’s contracture release to the left little finger and developed PIP joint contracture. A heterodigital flap was required from the adjacent ring finger to fill in the very large wound and skin deficit during the revision surgery. Another patient (Fig. 68.7) required little finger PIP joint arthrodesis for severe recurrent flexion contracture. The large PIP and volar finger soft tissue deficit was covered with a cross-finger flap. Fig. 68.6 (a) This 61-year old patient developed a severe scar contracture of the little finger after multiple Dupuytren’s contracture releases. (b) After scar excision and release, a template of the large soft tissue wound in the distal palm was created with a rubber Esmarch bandage. (c) A heterodigital vascularized island flap from the left ring finger was dissected back to the branch point of the common digital artery. (d) The flap was transposed to the palm and inset. A groin full-thickness skin graft was used for closure of the donor defect. Early postoperative demonstration of finger flexion (e) and extension (f,g). The patient will need therapy to achieve full PIP flexion and extension. Fig. 68.7 (a) A 73-year-old patient who previously had Dupuytren’s contracture release of the little finger developed a severe flexion proximal interphalangeal (PIP) joint contracture into the palm. (b) A soft tissue deficit on the volar aspect of the little finger was left after PIP arthrodesis. (c) A cross-finger flap from the adjacent left ring finger was used for coverage. (d) The long-term outcome after division of the cross-finger flap with resolution of PIP flexion contracture. Flexor tendon bowstringing is a rare complication. It may be more common in recurrent Dupuytren’s contracture when the flexor tendon sheath is not identified within the scar and is accidentally disrupted.38 Fig. 68.8 shows a patient who had disruption of the A2 pulley resulting in PIP flexion contracture and bowstringing of the left middle finger. He had release of PIP flexion contracture and flexor tendon pulley reconstruction with a tendon graft. Wide-awake tumescent local anesthesia is useful so that full functional correction can be assessed by patient activity (Video 68.2). Although the recurrence rate is highly variable, it is well-established that the overall recurrence rate for partial fasciectomy is lower compared with needle fasciotomy and collagenase injection.30 Repeat surgery for Dupuytren’s contracture presents a challenge for hand surgeons. The anatomy is often distorted because of adherent scar tissue, making dissection difficult and the potential for neurovascular injuries more likely. Therefore reoperation for Dupuytren’s contracture should be preceded by a thorough assessment and planning.1,38 Evaluation of previous incisions and extent of soft tissue contracture may help to anticipate the need for skin grafting and possible flap to achieve wound closure. Identification of previously injured nerves and vessels is helpful. This is done by thorough sensory assessment and a digital Allen test. Patients should once again be counseled on realistic outcomes and the potential for recurrence. They should be warned that postoperative therapy may be more extensive. When compared with partial fasciectomy, the recurrence rate of needle fasciotomy was significantly higher based on a 5-year follow-up from a randomized control trial (84.9 versus 20.9%).42 Patients who developed recurrent disease after needle fasciotomy were offered a second treatment with needle fasciotomy or partial fasciectomy. On average, 50% of the patients treated with repeat needle fasciotomy developed a second recurrence after 4.4 years. Based on these findings, the authors concluded that needle fasciotomy is an effective alternative treatment for recurrent Dupuytren’s disease as long as patients are willing to accept the higher recurrence rate for the benefit of shorter recovery time and less invasiveness.
68
Dupuytren’s Contracture
Treatment Options
Fasciectomy
Needle Fasciotomy
Collagenase Clostridium Histolyticum
Avoiding Unfavorable Results and Complications in Dupuytren’s Contracture Intervention
Patient Expectations
Avoiding Neurovascular Injury
Fasciectomy
Needle Fasciotomy
Wound Healing
Fasciectomy
Needle Fasciotomy

Collagenase Clostridium Histolyticum
Flexion Contracture
Joint Contracture

Flexion Deformity
Recurrence
Complex Regional Pain Syndrome (CRPS) and Flare Reactions
Complex Regional Pain Syndrome
Concurrent Carpal Tunnel Syndrome
Tension-Free Splinting and Flare Reactions
Flexor Tendon Injury
Needle Fasciotomy
Collagenase Clostridium Histolyticum
Managing Unfavorable Results and Complications in Dupuytren’s Contracture Intervention
Digital Nerve Injury
Neurapraxia
Digital Nerve Division
Wound-Healing Complications
Skin Necrosis
Skin Tears
Flexion Contracture
Joint Contracture

Bowstringing
Recurrence
Fasciectomy
Needle Fasciotomy
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine