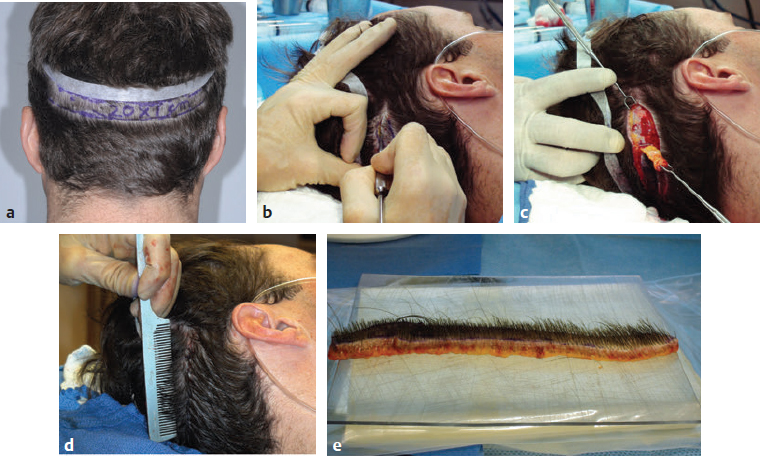
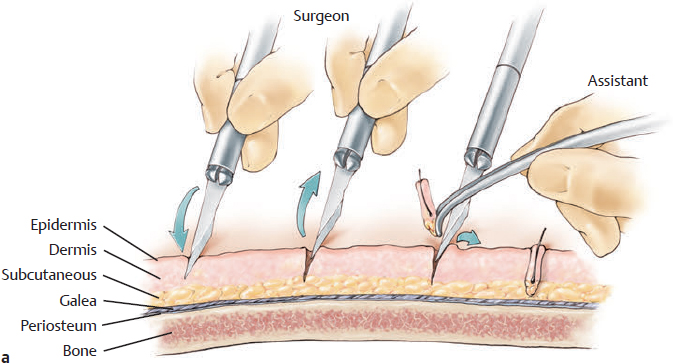
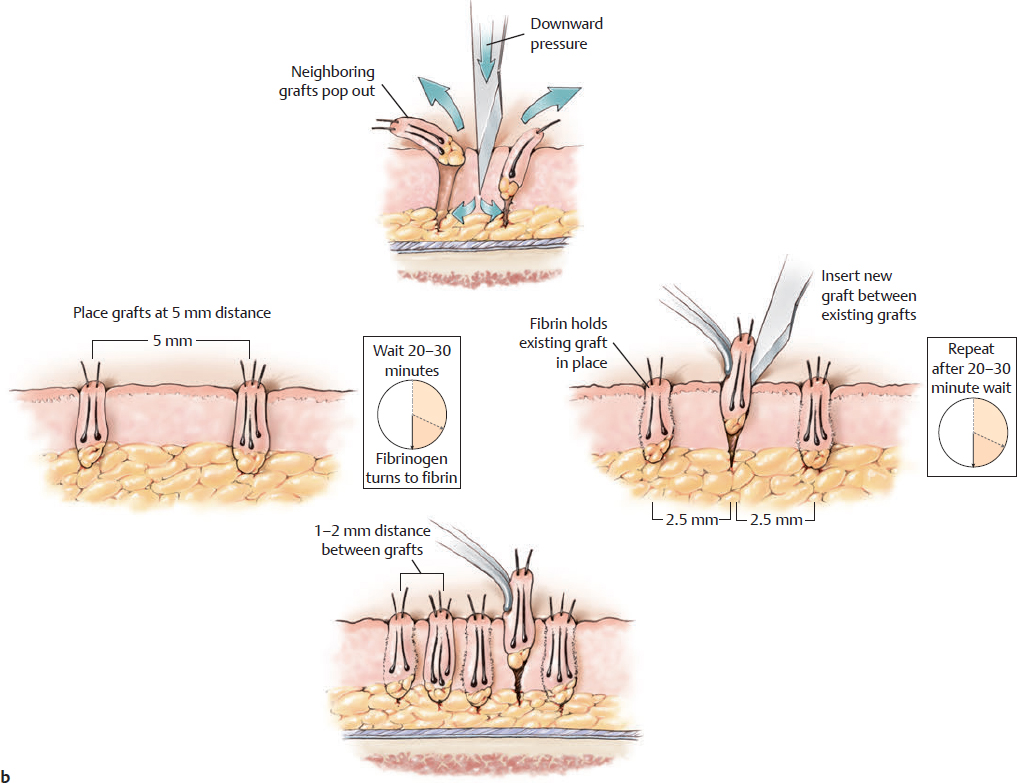
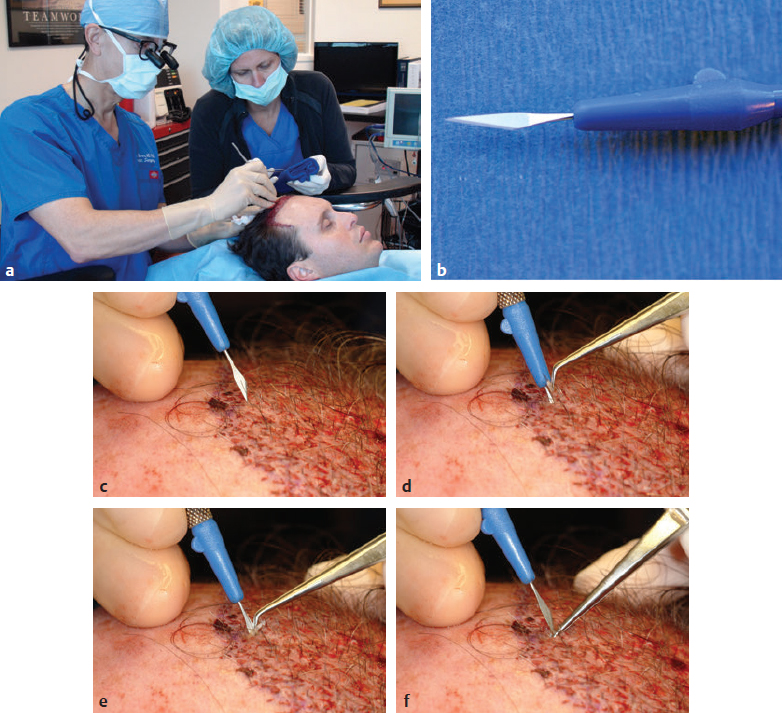
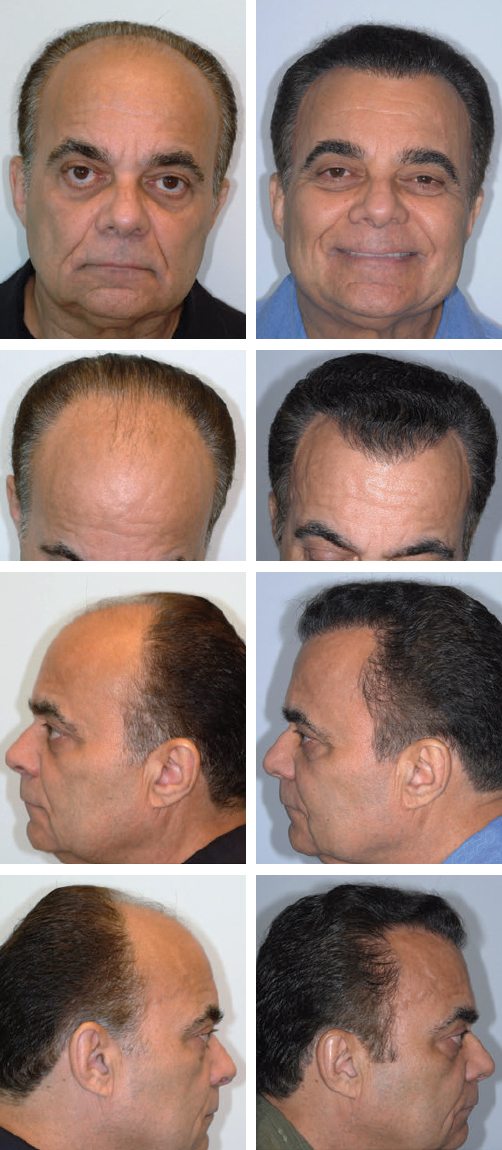
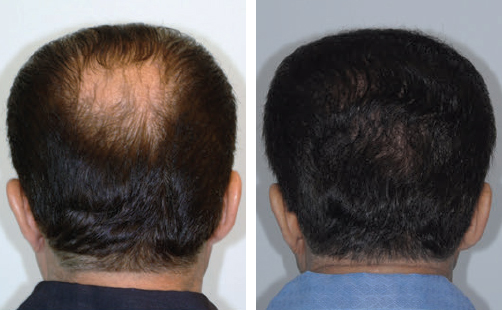
CHAPTER Hair transplantation was popularized in the late 1950s by Orentreich,1 whose work spurred many important concepts for aesthetic surgeons. For example, Orentreich presented the donor “dominance concept” that the genesis of hair is at the root of each individual hair follicle and that roots transplanted from a donor area (occipital and temporal areas) to areas of baldness will continue to grow hair as long as it would have in the donor area. This is the key to hair transplantation: the hair in the donor area is resistant to the effects of dehydrotestosterone (DHT), which is why it continued to grow, whereas the hair in the areas of baldness (the top of the head and crown) is not. Of course, getting the hair to grow is not enough; it must grow and look natural. With that in mind, it is fairly easy to determine whether a patient is a good candidate for hair transplantation. As for any other elective procedure, the surgeon must make sure the patient has a low risk for surgical complications. If the surgeon has any doubts about the patient’s health, clearance should be obtained from the patient’s primary care physician. If the patient is taking anticoagulants, the surgeon must determine whether it is safe for the patient to discontinue them. Hypertension, diabetes, and other conditions that affect surgical safety and healing must be under control. My technique is based on 30 years of private practice; it is the most common procedure performed in my practice.2–11 Many of my patients have experienced unfavorable results elsewhere and are seeking revision. When planning hair transplantation, surgeons must think and plan for the long term; even on young patients, a mature hairline should be designed. The level of the hairline is an important component of facial aesthetics. It frames the face and defines the proportions of the face. Ideally it is about a third of the vertical length of the face. There is no magic measurement from the eyebrows to the hairline; the ideal distance varies depending on the craniofacial proportions. The surgeon must artistically design it for each patient individually to mimic a natural mature hairline. The surgeon marks the planned hairline preoperatively, ensuring the patient understands that a hairline that is appropriate for a 16 year old will not look natural at age 40 or 50 years and older. The hairline should also be slightly irregular, with no rows or lines—in essence, a no-line hairline. Single-hair grafts should be used at the hairline. I prefer the strip technique for donor site harvesting. Referred to as follicular unit transplantation (FUT), this technique involves harvesting a narrow horizontal ellipse of scalp from the donor area (occipital and temporal areas), incising parallel to the hair follicles and closing primarily without tension. This allows the donor site to heal very well with minimally detectable scarring. This technique is described in detail later in this chapter. An alternative technique for harvesting the donor hair is follicular unit extraction (FUE), in which a 0.8- to 1-mm round punch blade is used to extract the follicles one by one, manually or by robotics. A large area of donor scalp needs to be shaved. This makes it extremely difficult to harvest a high percentage of intact hair follicles, because it is difficult to go exactly parallel to each hair root along its length and extract them all intact when only the surface is visible. Incomplete and transected grafts do not grow hair well. Although there is a learning curve in both techniques, I prefer (FUT) because of the broad visibility with background lighting and magnification of each hair root from top to bottom and the ability to keep the graft at least 95% intact, hence increasing the viability and growth. Most patients have limited donor hair, so it is essential not to waste any. I place the patient supine and use intravenous sedation with midazolam and fentanyl and occipital and supraorbital nerve blocks with 0.5% bupivacaine with epinephrine 1:200,000. For a small child, general anesthesia may be better. Once the area is well anesthetized, tumescence infiltration is used along the donor ellipse to limit bleeding and assist in the graft dissection. I use the following solution: • 120 mL of normal saline • 20 mL of 2% plain lidocaine • 1 mL of epinephrine 1:1,000 • 40 mg of triamcinolone The same solution is used to infiltrate both the donor and the recipient area. By adding triamcinolone, patients have significantly less postoperative pain and edema. The occipital-temporal area generally has the thickest, most permanent hair. The donor site ellipse varies in dimensions depending on the number of grafts planned and the density of the donor site. If 2,000 or more grafts are planned, generally the ellipse measures 20 to 30 cm by 1 cm at the midline, up to 1.5 cm gradually tapering to 1 cm over the temporal areas (Fig. 28.1). The donor strip is sliced into 1- to 2-mm slivers (ellipse). The grafts must be handled as atraumatically as possible. The grafts are grasped with jeweler’s forceps by the fatty tissue under the hair bulbs or by the tissue around them, not by the hair bulb or dermal hair papilla itself (Fig. 28.2). The grafts should initially be placed at about 5 mm from each other, beginning at the front hairline and proceeding posteriorly. As fibrinogen turns into fibrin (15 to 20 minutes later), the grafts become more secure in place. A second pass is then made anteriorly between the previously inserted grafts, setting the grafts about 2.5 mm apart. Packing them densely too soon often causes them to “pop out”; reinserting them can be frustrating and time consuming. Again as the fibrinogen turns into fibrin more passes are made, placing more grafts between those already placed until there is approximately 1 to 1.5 mm between grafts11 (Figs. 28.3 and 28.4). Dressing consists of a nonadherent dressing, gauze, and a 3-inch elastic bandage (Fig. 28.5), which are removed on the second postoperative day. The donor site sutures (3–0 Prolene) are removed on the 10th postoperative day. The hair begins to grow at 3 to 4 months and appears aesthetically pleasing at around 6 months; the final result is evident at around 12 months (Fig. 28.6). This hair transplantation procedure is always successful. By handling the grafts gently and atraumatically, at least 90% of the grafts should grow good, healthy hair. Fig. 28.1 (a) Making the ellipse no more than 1 cm wide ensures closure without tension and a safer and more predictable degree of minimal scarring. (b,c) Harvesting with a no. 10 Bard Parker blade under ×3.5 loupe magnification, making the incision parallel to the hair shafts. The plane of dissection is just deep to the hair follicles and superficial enough to avoid injury to significant vessels and sensory nerves. A small amount of subcutaneous fatty tissue is often left over the galea or fascia. (d) A tension-free closure, such as with 3–0 simple running Prolene, is important, because it allows for optimal donor site healing. Closing without undermining is preferred but not essential. (e) Donor strip (ellipse) on the sterile silicone board, with background lighting to further increase visibility of the hair roots. Fig. 28.2 (a) Surgical assistants dissecting follicular unit grafts under ×10 magnification. (b) Slivers of scalp 1 to 2 mm thick, incised parallel to the hair follicles, maintaining them intact from beginning to end. The harvested donor tissue must be kept chilled in normal saline solution. (c) Follicular unit dissection from out of the slivers. Accuracy is imperative for graft survival and ultimate growth. (d) Magnified view of one-, two-, and three-hair follicular unit grafts. Notice the integrity of each graft. Fig. 28.3 (a) “Stick and place” technique on the scalp. (From Barrera A, Uebel C, eds. Hair Transplantation: The Art of Follicular Unit Micrografting and Minigrafting. 2nd ed. New York: Thieme Medical Publishers; 2014.) (b) Placement of grafts. (From Barrera A, Uebel C, eds. Hair Transplantation: The Art of Follicular Unit Micrografting and Minigrafting. 2nd ed. New York: Thieme Medical Publishers; 2014.) However, the number of hair grafts done will affect the result. For patients who want as much density as possible, assuming they have sufficient donor hair, the procedure can be repeated several times. I prefer to wait a year between sessions to assess the results and allow the scalp to recover completely. A year later, or any time thereafter, the area can be regrafted, filling in between the previous grafts to further increase the hair density. Fig. 28.4 (a) A surgical assistant and the surgeon insert all the grafts using the “stick and place” technique. (b) A no. 22.5 blade is used for the scalp. (c) The surgeon selects each site and the blade inclination that will allow the hair to grow at the most optimal angle (inclination), mimicking any residual thinning hair (if available). Using single-hair follicular units at the front hairline (approximately 1 cm) is key; posterior to that point, one-, two-, three-, or four-haired follicular units may be used. (d) The graft is brought into position to slide it along the blade shaft, into the recipient slit. (e) The graft is inserted using the blade as a shoehorn. (f) The graft is held in place with the tip of the blade as the jeweler’s forceps are retracted to prevent it from pulling out. Fig. 28.6 A 63-year-old patient before (left) and after (right) having 8,109 follicular unit grafts inserted in three sessions. (These images provided courtesy of A. Barrera.) This section details the unfavorable results that can occur from hair transplantation, how to prevent them, and how to correct them (Video 28.1).12–19 Most unfavorable results are caused by poor planning and execution of the procedure. Summary Box
28
Hair Restoration
Current Hair Transplantation Techniques

Avoiding Unfavorable Results in Hair Restoration

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


