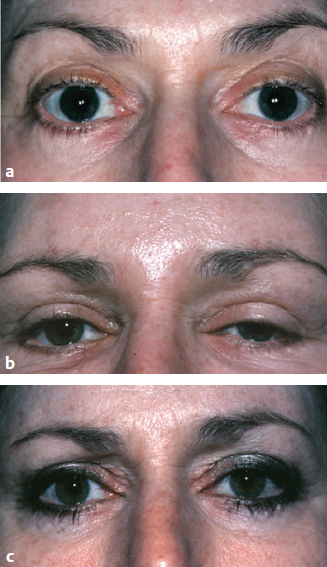
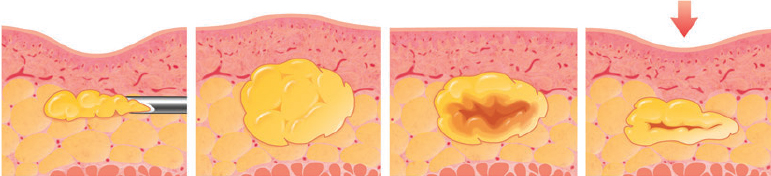
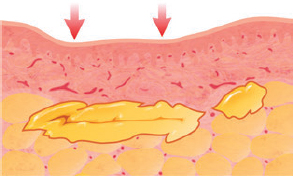
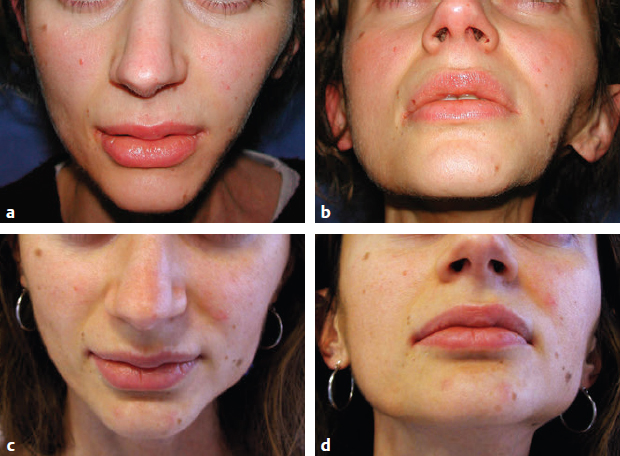
CHAPTER Although fat grafting procedures have an established record of safety and reports of adverse outcomes are uncommon, complications do occur with fat grafting, as with any surgical procedure. The majority of complications are related to aesthetic appearance and are most often associated with the location, manner, and volume in which the fatty tissue is placed into recipient areas. These include overcorrection, undercorrection, visible irregularities, migration of placed fat, and donor site problems.1 Improvement in a patient’s facial or body contours is not always enough for a successful result. One of the most difficult elements of this procedure is reliably predicting what the patient desires before the procedure and what result will make the patient happy; often these are not the same.2 In addition, if the patient is not psychologically prepared for changes in the face or body, for the postprocedure course, or for possible unexpected events, an otherwise successful procedure can be a disappointment. The operating surgeon must be familiar with the complications of fat grafting and should warn the patient about the problems that are most likely to occur during a fat grafting procedure. Before the operation starts, the patient should carefully read and understand the informed consent, in which all the details of the planned procedure are accurately explained along with the predictable outcome, the postoperative course, the patient’s responsibilities during recovery, and potential sequelae and complications. Structural fat grafting has other potential complications, including infection; damage to underlying structures such as nerves, muscles, and glands; necrosis; calcifications; oil cyst formation; and the most dreaded, embolism. Fortunately, the complication rate with fat grafting is extremely low compared with most open surgical techniques and the incidence of unpleasant events decreases significantly with surgeon experience. Summary Box Possible Complications of Fat Grafting Aesthetic Complications Major Complications • Insufficient volume • Resorption • Swelling • Irregularities, lumps, calcifications, oil cysts • Fat migration • Donor site complications • Infection • Damage to underlying structures • Intravascular complications The goal of structural fat grafting is for the grafted fat to survive evenly and predictably. The most common complaint that patients have after the swelling subsides is that they had expected more or less fullness in a specific area. There are numerous factors to consider when estimating the volumes of fat to be grafted, including the resorption rate and intraoperative edema. Obtaining the exact amount of fullness that will satisfy a patient can be difficult. Careful planning and fat preparation are essential. Even after the physician and patient agree on the desired change, many variables will affect the outcome. The surgeon who performs the procedure is commonly asked how much of the grafted fat will survive. At present it not possible to give a satisfactory answer. A good approach is to look at the photographs of patients when they return for follow-up, observing the volume of fat that was grafted on that person to produce a specific change. It is important to understand what different amounts will do rather than focusing on the question of how much will survive. Thus it is even more important to know what 10 cc of fat placed in the face will look like as compared with 20 or 30 cc. After the edema subsides, if the patient expected more fullness than was achieved, a difficult question is whether this adverse outcome is related to insufficient placement or to resorption. Indeed, resorption represents one of the main drawbacks of the procedure, ranging from 25 to 80%.3 Numerous means are available to restrain resorption rate as much as possible: • Obtaining pure fat • Reducing trauma • Preserving viability Ideally, the surgeon should obtain the purest fat possible by eliminating the blood and oily component, along with other debris, with minimal damage to adipose tissue. The presence of blood, fatty acids, and other debris seems to stimulate an inflammatory response, which induces resorption. No matter how carefully the fat is prepared, it will not be 100% pure. Varying degrees of oil, blood, and other impurities, such as lidocaine, are present in the lipoaspirate even after processing. Furthermore, a varying degree of the refined material placed will not be viable. Even with scrupulous technique, a portion of the fatty tissue will die from the negative pressure, exposure to air, and mechanical trauma sustained during harvesting and refinement procedures of the fragile fatty tissue. Forcing the lipoaspirate through a small cannula places a positive pressure and further mechanical trauma on the fatty tissue parcels. This trauma can vary from patient to patient. For instance, in thin patients the fat cells store much less triglyceride, which makes them smaller. When the tissue parcels are composed of smaller cells, they are more likely to flow through the cannulas without rupturing. In heavier patients, the fat cells are engorged with triglycerides and are therefore larger. These larger cells with stretched cell walls can be more easily ruptured by the mechanical maneuvers associated with harvesting, purification, and placement. It is difficult to predict the exact percentage of tissue that will be lost in these steps. Even under ideal circumstances a small portion of transplanted fat will die, but certain conditions increase the likelihood of fat necrosis. Ischemia represents the major cause4 (Fig. 19.1). It is essential to avoid creating a bolus, which induces necrosis of the central portion of the transplanted adipocytes. Death of adipocytes and progenitors causes fibrosis, calcifications, and oil cyst formation.5 On the contrary, placement of minimal aliquots of fat maximizes the contact and favors the successful take of the graft. Forcing too much tissue into a limited recipient site such as the nose, or placing the grafted fat in too thick a layer (e.g., to fill a deep sternal defect) can result in necrosis, because the grafted tissue does not receive adequate nutrition or respiration, as well as the development of long-term tissue atrophy, oil cyst formation, and progressive calcification4 (Fig. 19.2). Fig. 19.1 The importance of avoiding creation of a bolus in structural fat grafting. Placement of an excessive amount of fat as a bolus isolates the transplanted cells in the center of the lump from the blood supply. Without nutrition and respiration, the cells of the central lump may die indiscriminately. The end result is the formation of an oil cyst and fibrosis. (Reproduced from Coleman SR. Structural Fat Grafting. New York: Thieme Medical; 2004.) Fig. 19.2 (a,b) Many early authorities on fat grafting advocated molding of the fatty tissue after placement to create the desired shapes, to distribute the fatty tissue evenly, and to smooth out any surface irregularities. After placement of as much as 1 or 2 cc of fat at each pass, these surgeons recommend using digital pressure to redistribute the fatty tissues. Unfortunately, this type of maneuver affords little control over the subdermal configurations of the manipulated volume, and the fat may even squirt in many directions to form irregular pools of tissue. (c,d) Unequal access to nutrition and respiration can cause irregular survival of the fat, which results in surface irregularities. If a cyst or clump forms accidentally, digital manipulation can sometimes flatten such minor irregularities. However, the tissue should never be placed with the idea that digital pressure can change the shape after placement. The edema that is created by fat placement and subsequent manipulation creates the illusion that because the swollen skin surface initially appears smooth, the underlying graft has been placed in a smooth layer. If the fat were all to survive, the surface would remain smooth; however, a portion of fat often dies. (Reproduced from Coleman SR. Structural Fat Grafting. New York: Thieme Medical; 2004.) Postprocedure edema is the most common problem associated with structural fat grafting. Patients need to be well prepared in advance for their postoperative appearance so they are not unduly alarmed by the degree of swelling that occurs. It is also important to warn patients that this adverse situation will continue to increase for up to 3 days after the procedure so they do not panic when they notice this happening. The injection of local anesthetic into the tissues can swell and “pump” the tissues full of solution. The amount of local anesthetic should be minimized to the smallest volume that will numb the area and obtain vasoconstriction with a minimum of distortion. Use of electrotherapy devices for 5 to 7 days has been successful for reducing swelling after rhytidectomy, liposculpture, and facial fat grafting.6 Forcing a blunt cannula through living tissue will immediately provoke edema. To separate the tiny parcels of fat from one another, hundreds of passes are made with a blunt cannula; the end result is a significant amount of edema4 (Fig. 19.3). This edema obscures the visual clues that might be helpful for determining an end point. Also, because of individual patient variations, it can be difficult to predict how a given patient’s body will react during and immediately after the injection of fatty tissue. The swelling will vary from patient to patient, from area to area, and even from side to side in the same patient. This three-dimensional technique of placing refined fat into the recipient sites creates the shape, volume, and structural changes defined in the operative plan. The fatty tissue should be deposited in the desired location, shape, and volume with each pass of the infiltrating cannula. Because the visual clues seen during infiltration of fat can be deceptive, the intraoperative appearance of the infiltrated site should not be used as the sole criterion to determine the amount of fat to be placed, which is why it is important to estimate the volume to be infiltrated before the procedure begins. Fig. 19.3 Because the transplanted fat is often located at an inconsistent distance from a blood supply, it will die in an irregular fashion. As the tissue necroses and resorbs, irregularities emerge. This may happen as late as 4 or more months after the procedure, when swelling subsides. Placement of a lump of tissue with the intent to mold it into a specific shape commonly results in irregularities. (Reproduced from Coleman SR. Structural Fat Grafting. New York: Thieme Medical; 2004.) One of the most distressing and common negative outcomes of grafting fat is visible and palpable irregularities and lumps. They are mainly the result of necrosis of the grafted material, which induces fibrosis, calcifications, and oil cyst formation. Kato et al7 demonstrated that although a single dead adipocyte can be completely absorbed, the extruded oil droplets are replaced by a cicatrization phenomenon (collagen matrix formation), with chronic inflammation. If numerous tiny droplets (smaller than 1 mm) occur, the consequence is the development of palpable surface irregularities. If the necrosis is more consistent (larger than 10 mm), an oil cyst typically forms, again with chronic inflammation.8 Once established, oil cysts are permanent, with no tendency to reduce in size or to reabsorb9 (Figs. 19.4 and 19.5). Fig. 19.4 (a,b) This patient had fat grafting that included 7 cc of adipocytes placed in multiple tunnels to correct facial asymmetry. A left unilateral fibrotic cyst was noticed on her jawline 1 month after surgery. (c,d) The cyst still had not reduced after 1 year. (Reproduced from Coleman S, Mazzola RF. Fat Injection: From Filling to Regeneration. 2nd ed. New York: Thieme Medical; 2017.) Fig. 19.5 Bilateral fibrotic cysts resulting from fat grafting to correct tear trough deformity. A 19-gauge blunt-tipped cannula was used to place 0.5 cc of refined less-dense fat per side. To prevent a depression ensuing from the cyst’s excision, a midface lift was performed. (Reproduced from Coleman S, Mazzola RF. Fat Injection: From Filling to Regeneration. 2nd ed. New York: Thieme Medical; 2017.) In critical areas, like the breast, the formation of oil cysts and calcifications may induce diagnostic problems with breast cancer.10 However, calcifications of fat necrosis origin are substantially different from those induced by breast cancer. An expert radiologist can recognize the difference. Fat necrosis after grafting basically depends on the technique. Oil cysts are most common after large volume trans fer or bolus injection, and they occur mainly in the breast and buttocks, where larger cannulas (16 to 18 gauge) are used. They seldom occur on the face. According to Kato et al,7 the sequence is as follows: The death of adipocytes gives rise to oil droplets, followed by the formation of necrotic, calcified tissue that eventually develops an oil cyst with a tendency to grow. The solid wall around the cyst prevents absorption of new oil within the cyst itself, the size and configuration of which remains stable.8 Placement of fatty tissue so it creates a smooth fullness is imperative for a successful result. However, smooth placement demands that the physician have technical ability as well as experience. This is especially true in recipient areas with thin skin, as in the eyelid (see Fig. 19.3). Use of thin cannulas (e.g., 21 gauge), less-dense fat, a spaghetti-like technique, and painstaking molding of the grafted material can potentially help reduce the chance of fat necrosis and the resultant unpleasant irregularities and oil cyst formation. Fat migration occurs most often in areas where muscle motion is particularly evident, such as at the insertion of the glabella into the midbrow skin above the eyebrow. After the surgeon has infiltrated the midbrow with fatty tissue, the skin surface appears relatively smooth, because the corrugator muscles are not contracting at that point. However, once the patient is awake, depressions will develop when the muscles move, such as when the patient grimaces. The photographs may look great, but the forehead has distressing irregularities upon motion. In these patients, continued botulinum toxin (Botox [Allergan]) injections may be warranted. Botulinum toxin should be used judiciously before infiltration of fat into the glabella, nasion, and forehead. For deep creases that are not relieved completely with the botulinum toxin injection, the paralysis can be helpful by stenting the mobility of the crease to create a predictable, stable correction of the creases. For shallow creases that are obliterated by the induced paralysis, botulinum toxin should not be used, because localization of the problem areas is difficult. Superficial layering of fatty tissue into the submucosal plane and immediately deep to the vermilion gives greater stability to the transplanted fat. Placement into the lip for eversion should reduce the effects of the powerful contractions of the orbicularis oris muscle. The use of frozen fat exposes patients to the risk of severe infections, because it is composed of dead tissue.11,12 Results with frozen fat are variable, and most often the grafted material resorbs almost completely. The use of autologous banked fat should be strongly discouraged because of the significant potential for clerical error. Incorrect documentation could result in the inadvertent transmission of viruses such as HIV or hepatitis or the stimulation of an auto-transfusion-type reaction. Physicians who intend to inject stored autologous fat should be aware that specific safety requirements are needed, and that both state and federal government agencies have stringent guidelines concerning tissue banking for autotransplantation. However, the proposed strategies for cryopreservation of harvested tissue show great promise. Cryoprotective agents are added to the tissue, which is cooled at a controlled rate to a low storage temperature. Studies have shown remarkable maintenance of lipoaspirate viability when a careful thawing protocol is followed. This may become an attractive option for patients to have their tissue banked for future fat grafting, as long as the fat is properly preserved and remains sterile and viable. Fig. 19.6 Pinching of the abdominal skin is necessary to harvest fat from thin patients or in the presence of an abdominal hernia to avoid the risk of gut and internal organ perforation. (Reproduced from Coleman S, Mazzola RF. Fat Injection: From Filling to Regeneration. 2nd ed. New York: Thieme Medical; 2017.) Removal of subcutaneous fatty tissue reduces support and can result in irregularities, increased wrinkling, and depressions at the donor site. For this reason, fat must be suctioned with a 2- or 3-mm cannula; the surgeon should extend the movements of the cannula in different directions to avoid aspirating fat from only a single specific area, which inevitably results in an unpleasant depression that is difficult to correct. For facial applications, fat is usually harvested from the lower abdomen, which is typically the best site for obtaining the necessary volume of lipoaspirate. In slender patients, the inner thigh or inner knee offer alternative sources of fat. If a large volume of fat is to be grafted, other donor site areas may be selected, such as the dorsum, flanks, peritrochanteric region, and others. However, if fat is harvested from the flanks or peritrochanteric region, it is essential to aspirate it bilaterally to maintain symmetry and to prevent the donor area from having a different contour than the contralateral side. Care should be taken to choose concealed zones such as the umbilical fold, suprapubic area, or inguinal fold for the cannula’s entry point to avoid visible scars that might become hypertrophic.9 When harvesting fat from the abdomen, it is essential to pinch up the skin to avoid perforating the gut or internal organs with the cannula. This is more likely to occur in slender patients or in those with an abdominal hernia (Fig. 19.6).13,14 Patients undergoing structural fat grafting should be treated with the same care as with any surgical procedure to avoid the potential risk of infection. Although the procedure is considered relatively simple, adherence to key principles of sterile technique is critical to avoid adverse outcomes.15 As a preventive measure, it is advisable to use a chlorhexidine scrub and to prep the donor and recipient sites with a povidone-iodine solution. Intraoperative antibiotics are recommended in potentially contaminated areas such as the lips, genital areas, and oral cavity (Fig. 19.7). In cases of delayed infection, a high index of suspicion should be maintained for mycobacterial or other unusual infections.4 Fig. 19.7 This patient had fat grafting first into the lips and then later into the glabella. Four days later, she presented with a purulent infection that required open drainage from her lips and glabella. Her oral mucosa was likely perforated during the lip infiltration with a contaminated cannula. (Reproduced from Coleman SR. Structural Fat Grafting. New York: Thieme Medical; 2004.) The following guidelines are applicable and should be followed when dealing with potentially contaminated areas: 1. Patients should gargle with a chlorhexidine gluconate 0.2% oral rinse immediately before any procedure on the face. 2. The lips are always infiltrated last to avoid inoculating other areas with bacteria. 3. If the oral or nasal mucosa is perforated during infiltration near these areas, the cannula should immediately be removed off the sterile field. 4. Patients should receive a prophylactic intravenous injection of cephalosporin or other appropriate antibiotics before incisions are made at a site in which contamination from a mucosal surface is possible. 5. For nasal, vaginal, or anal areas the same prophylactic methods should be considered. 6. In cases of delayed infection, a high index of suspicion should be maintained for mycobacterial or other unusual infections. Fig. 19.8 Care should be taken to avoid introducing cotton fibers along with the grafted fat. (Reproduced from Coleman SR. Structural Fat Grafting. New York: Thieme Medical; 2004.) Care should be taken to avoid inadvertently introducing a foreign body into the harvested fat. This is most likely to occur during the process of refining the fatty tissue4 (Fig. 19.8). Woven cotton nasal packing or woven sponges are sources of such contamination. Nonadherent gauze pads and other wicking devices may be an alternative, although most of them can release loose fibers after being cut into the appropriate sizes. Obviously, fibers of cotton or other substances placed with the grafted fatty tissue can result in inflammation and scarring when they are transferred into the donor site. Codman pads, commonly used by neurosurgeons, are recommended for wicking the oil from the fatty tissue; they seem to unravel or release fibers the least. Sensory and motor nerve injuries that have occurred with fat grafting as an isolated procedure have been related to the use of a sharp needle or a pointed cannula to release a scar or adhesion. Several patients have experienced transient sensation loss, presumably from placement with a sharp needle near the supraorbital or infraorbital nerve. It is these temporary sensory deficits that prompted me (S.C.) to design the blunt-tipped cannulas now in use. With blunt cannulas alone, permanent motor nerve injuries are rare and only minimal sensory nerve symptoms may occur, most of them transient. Fig. 19.9 Permanent mandibular branch injury after an attempt to remove an oil cyst on the jawline that resulted from fat grafting to correct facial asymmetry (see Fig. 19.3). (Reproduced from Coleman S, Mazzola RF. Fat Injection: From Filling to Regeneration. 2nd ed. New York: Thieme Medical; 2017.) In our series of patients, four injuries of the facial nerve have occurred: two transient marginal mandibular injuries (S.C.) and one permanent (R.M.) and one transient frontal branch injury (S.C.). The first may happen when sharp needles are used. I (S.C.) use sharp needles very superficially to avoid intravascular injection and to minimize damage to the nerves. I do not place the injections deep. In the second case, a 2.1-mm suction cannula was used to remove tissue from a jowl at the same time that fat was placed along the anterior mandibular border. The action that precipitated the injury most likely resulted from the aperture of the suction cannula applying negative pressure during tissue removal. The third case took place in an attempt to excise an adherent oily cyst located along the course of the marginal mandibular branch, a sequelae of previous fat grafting. A 19-gauge blunt cannula was used to remove the cyst, but the movements of the cannula may have been responsible for damaging the nerve. At 2 years postoperatively, the situation remained unchanged. A temporary injury to the frontal branch of the facial nerve happened after placement of tissue in the temple and preauricular regions. It resolved spontaneously within 4 weeks9 (Fig. 19.9). Violation of muscle fibers of the face or body with needles or cannulas can injure the muscle and cause restricted or impaired motion. Great attention should be made not to damage mimic and masticatory muscles.
19
Fat Grafting for Facial Rejuvenation
Avoiding and Managing Unfavorable Results and Complications in Fat Grafting
 Embolization
Embolization
 Stroke
Stroke
 Blindness
Blindness
 Central retinal artery occlusion
Central retinal artery occlusion
 Skin necrosis
Skin necrosis
 Death
Death
Common Aesthetic Complications
Insufficient Volume
Resorption
Obtaining Pure Fat
Reducing Trauma
Preserving Viability
Placing Minimal Aliquots of Fat

Swelling
How Swelling Occurs
Irregularities, Lumps, Calcifications, and Oil Cysts

How Irregularities Occur
Preventing Irregularities
Fat Migration
Use of Frozen Fat

Donor Site Complications
Major Complications
Infection

Avoiding Contamination
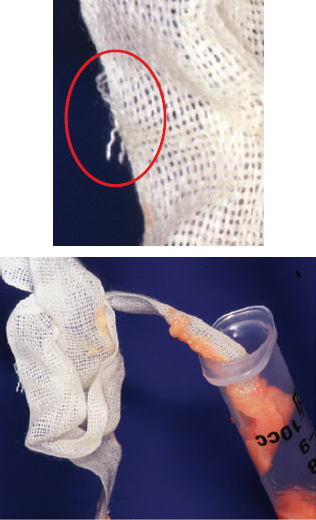
Avoiding the Introduction of Foreign Bodies
Damage to Underlying Structures
Nerve Injury

Muscle Injury
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine