Reconstruction of the Perineum
Paul H. Tran
Valerie Lemaine
INTRODUCTION
The goals of reconstructive surgery are restoration of both form and function, and this is especially important when dealing with reconstruction of the perineum. This area presents complex challenges to the plastic surgeon due to the close proximity of several key functional systems, namely the urinary, gynecologic, and gastrointestinal tracts.
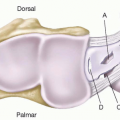
The perineum can be conceptualized as a diamond-shaped space forming the outlet of the pelvis. It is confined within the following boundaries: (1) anterolaterally, by the inferior margin of the pubic symphysis and the borders of the ischiopubic rami; (2) posterolaterally, by the coccyx and the sacrotuberous ligaments (covered by the gluteus maximus muscles); and (3) laterally, by the two ischial tuberosities. It can be subdivided into two triangles, the urogenital triangle anteriorly and the anal triangle posteriorly. The perineum is highly vascular in both males and females. The superficial and deep external pudendal arteries arise from the femoral artery and provide the main blood supply to the skin and fascia of the anterior triangle. They divide into abdominal and perineal branches approximately 4 to 6 cm from the pubic symphysis. The main pedicle of the posterior triangle is the internal pudendal artery, a branch of the internal iliac artery. It gives rise to the penile (or clitoral) branch and the superficial perineal artery. The superficial perineal artery divides into medial and lateral branches and continues into its terminal branches, the posterior scrotal (or labial) artery. There is also a rich supraaponeurotic vascular plexus supplying the labia majora in women and scrotum in men and surrounding perineal skin and soft tissue.
Reconstruction of the perineum can be complicated by prior surgeries and incisions, absent or inadequate musculature, impaired wound healing from radiation therapy, or from altered bloody supply. Factors such as smoking, diabetes, immunosuppression, atherosclerosis, prior surgeries, or advanced age are taken into consideration to avoid errors in flap selection and to maximize the outcome of the reconstruction.
GENERAL PRINCIPLES
Etiology of Defects
Perineal reconstruction may be indicated for congenital or acquired defects. Congenital perineal defects result from Müllerian or Wolffian aplasia, producing urogenital disorders such as imperforate anus, bladder exstrophy, and vaginal agenesis or atresia. Acquired perineal defects most commonly occur following surgical excision of primary or recurrent colorectal, gynecologic, or urologic malignancies. In this setting, perineal reconstruction frequently requires concomitant pelvic reconstruction by transferring well-vascularized tissue of sufficient bulk. Other less common causes of perineal and genital defects include traumatic injuries and infectious processes. Fournier’s gangrene is a rare but potentially fatal necrotizing fasciitis of the perineum and abdominal wall, along with the scrotum and penis in men and the vulva in women. Fournier’s gangrene is a surgical emergency. Skin loss can be incapacitating, difficult to repair, and may involve a combination of several techniques to achieve wound closure.
Preoperative Assessment and Surgical Planning
The preoperative evaluation of patients with present or expected perineal defects includes a comprehensive assessment of the patient’s comorbidities and the degree and nature of the anticipated perineal wound. Communication with the ablative surgeon is essential in case adjuvant therapies are planned that may influence the surgical plan. The anticipated defect of the external genitalia, the perineal skin, and, in the female patient, the vagina is evaluated. If partial or total perineal proctectomy is performed with the surrounding skin, it is essential to anticipate the amount of skin that will be removed. If a pelvic exenteration is planned, vascularization of the pelvic floor musculature may be disrupted. If a cystectomy is planned, preoperative discussion with the urologist for planning an ileal conduit is essential.
RECONSTRUCTION OF THE PERINEUM
Perineal reconstruction will ideally result in a healed wound in a single-stage procedure, with restoration of normal or near-normal function and minimal associated morbidity. Reconstruction is usually performed with local or regional flaps from the lower extremity and abdomen, and rarely requires free tissue transfer. Extensive perineal defects may require reconstruction with a combination of flaps. A useful start is the reconstructive ladder, which organizes options by complexity.
Small defects of the perineum can frequently be closed primarily. Moderate-sized, superficial defects are amenable to closure with either healing by secondary intention, skin grafting, or local skin flaps such as a rhomboid flap. Local surveillance in diseases with high recurrence rates, such as Bowen’s disease, may be easier following skin grafting. Skin grafting and local flap techniques may be suboptimal in the setting of urinary or fecal contamination, or with locally irradiated tissues. Regional flaps may be more ideal. Large superficial defects of the perineum (Figure 96.1) may best be downsized by negative pressure wound therapy, followed by flap or skin graft coverage. Large defects following abdominoperineal resections or total pelvic exenterations typically require immediate placement of a vascularized flap into the pelvis and perineum. Non-reconstructed pelvic cavities may become filled with fluid and/or intestinal loops, increasing the risk of prolonged wound drainage, pelvic abscess, perineal wound dehiscence, or bowel obstruction and herniation. The transfer of well-vascularized flaps to the perineum allows wound closure without tension, promotes primary wound healing, decreases postoperative complications, and requires fewer stages. Communication with the oncologic surgeon is essential when designing skin incisions and planning the location of stomas to preserve potential flap donor sites.
Decisions regarding flap selection include the amount of soft tissue needed, the adequacy of local blood supply, the presence of surgical scars at the donor site, patient positioning during surgery, as well as the operative approach used (i.e., laparotomy versus perineal approach). In men, the pelvis is longer and deeper than in women, so this additional length should be factored into the flap design.
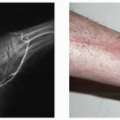
 FIGURE 96.1. A. A 24-year-old male with significant perineum tissue necrosis following infiltration of vasopressors into his left femoral venous catheter. B. After debridement of necrotic tissue. C. A wound vacuum-assisted closure was placed following debridement. D. One month after Split-thickness skin graft. Courtesy of Brian T. Carlsen, M.D. |
The vertical rectus abdominis myocutaneous (VRAM) flap, delivered to the perineum through an intraperitoneal transpelvic route, is a workhorse flap for combined pelvic and perineal defects.1 The VRAM flap is based on the inferior epigastric vessels and can be harvested with or without a skin paddle, depending on the characteristics of the perineal defect. As a myocutaneous flap, it provides a robust skin paddle to the perineum, has a reliable vascular supply, and allows transfer of a large volume of soft tissue to obliterate the pelvic cavity created by tumor excision.2,3 It is extremely versatile, as it can be used for pelvic reconstruction alone, as well as for reconstruction of defects of the anterior or posterior vaginal wall, or for total vaginal reconstruction. In addition to the vertical skin paddle design, transverse and large oblique extended skin paddles have been described for tissue coverage or obliteration of dead space.4 Important considerations include: (1) when the flap is transposed into the pelvis, care must be made to prevent twisting or kinking of the pedicle; (2) the VRAM myocutaneous flap skin paddle may be unreliable in obese patients with thick subcutaneous fat. When compared with thigh flaps, the VRAM flap following abdominoperineal resection and pelvic exenteration is associated with fewer major postoperative complications.5
The pedicled greater omental flap is another available option for reconstruction of the pelvic floor when a patient has undergone a laparotomy. This flap is based on the right or left gastroepiploic vessels and is useful in patients with a narrow pelvis, in obese patients, or when the VRAM flap is unavailable. The greater omental flap is sometimes unavailable for reconstruction due to insufficient size, presence of
adhesions, or previous surgical removal. Once the greater omentum has been dissected off the transverse mesocolon and the greater curvature of stomach, it can be passed to the right or left midline to bring vascularized tissue into a previously irradiated pelvis. This improves pelvic lymphatic drainage and decreases the risk of perineal hernia and bowel obstruction. The pedicled greater omental flap can also be covered with a skin graft for vaginal reconstruction.6
adhesions, or previous surgical removal. Once the greater omentum has been dissected off the transverse mesocolon and the greater curvature of stomach, it can be passed to the right or left midline to bring vascularized tissue into a previously irradiated pelvis. This improves pelvic lymphatic drainage and decreases the risk of perineal hernia and bowel obstruction. The pedicled greater omental flap can also be covered with a skin graft for vaginal reconstruction.6
The gracilis flap is another useful flap for reconstruction of the perineum, due to its versatility and minimal donor site morbidity. Furthermore, it often lies outside of the radiation field and does not require a laparotomy. However, it has a short pedicle and unreliable skin paddle, which can limit its use for coverage of large defects. A skin paddle can be designed over the proximal and middle third of the muscle. The major pedicle, the ascending branch of the medial circumflex femoral vessels, is identified as it courses deep to the adductor longus muscle. During flap harvest, the distal tendon is divided and the muscle is dissected from distal to proximal, dividing any perforating vessels. Extended dissection to the profunda femoris artery provides additional pedicle length. The flap can then be tunneled into the defect or used as a free flap (Figure 96.2).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


