Head and neck cancers account for 3% to 5% of all cancers in the United States, with an annual cancer mortality of around 2%. They are most common in men and in people over the age of 50 years and are more prevalent in the African American population. Over the past few decades, survival has generally improved for head and neck cancers. The improved survival is due to early detection and early therapy. However, these survival curves have plateaued in recent years. Cancers in the oral cavity, which are easily detected by physical examination, have historically had the best outcomes. However, improved imaging using magnetic resonance imaging, positron emission tomography, and fiberoptic endoscopy has led to earlier detection of previously difficult to evaluate areas such as the posterior pharynx.
Ninety percent of all head and neck cancers are squamous cell in origin. Common etiologic factors include tobacco and alcohol, which seem to have a synergistic effect. Regional causative agents may include betel quid in Asia and mate, a hot tea-like beverage, in South America. Over the past decade, the incidence of head and neck tumors in younger patients has increased. This has been linked with human papilloma virus (HPV) infections and is thought to be associated with exposure through oral sex. Fortunately, these tumors are more responsive to therapies and generally portend a better prognosis. The use of HPV vaccinations, which are effective in preventing cervical cancer, may also be effective against these tumors as they are also caused by HPV serotypes 16, 18, and 31.
Cutting-edge advances in reconstruction following extirpative procedures include the use of robotics to inset microsurgical flaps and virtual planning. Although the indications and operative techniques utilizing these advances are still evolving, early reports are promising and have shown decreased operative morbidity and possibly improved outcomes.
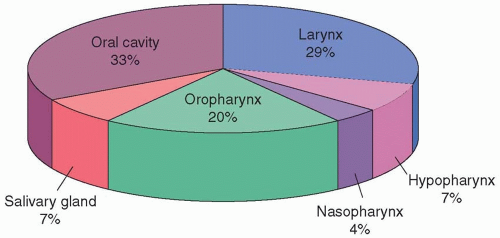
Small tumors in most head and neck regions have a 90% cure rate when treated by radiation or surgical resection. These survival figures decrease significantly with moderately advanced tumors, resulting in average 5-year survival rates of approximately 50%. The use of neoadjuvant therapy has also been an advance and has increased the potential for surgical resection of previously unresectable tumors. Overall survival based on stage is listed in Table 30.1. The distribution of these cancers based on anatomic subsite is displayed in Figure 30.1.1 Reconstruction of head and neck defects is critically dependent on a number of factors including anatomy, physiology, pathology of head and neck tumors, staging, and adjuvant therapy. This chapter will discuss the pertinent details of head and neck cancer and salivary gland cancer with the relevant anatomy.
HEAD AND NECK ANATOMY AND STAGING
A standardized approach to head and neck anatomy facilitates discussion and treatment among medical professionals. The primary site/subsite approach currently used for head and neck cancer reflects both unique regional tumor behavior and specific treatment-related considerations. This section of the chapter focuses on sites with the greatest incidence of pathology and on subsites with specific reconstructive challenges. Primary tumor sites include the oral cavity, nasopharynx, oropharynx, hypopharynx, and larynx (Tables 30.2, 30.3, 30.4, 30.5, 30.6 and 30.7).
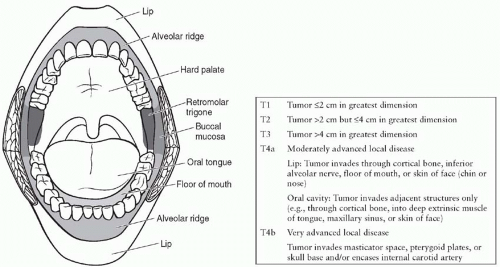
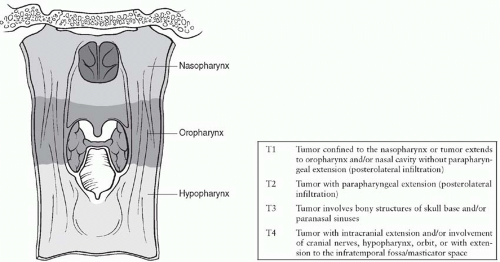
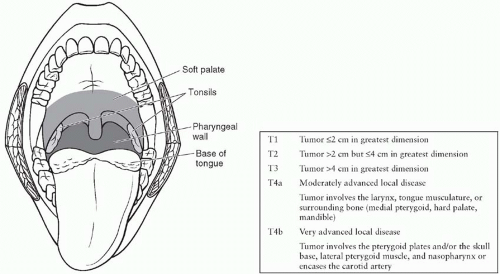
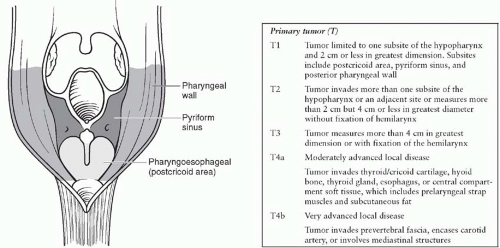
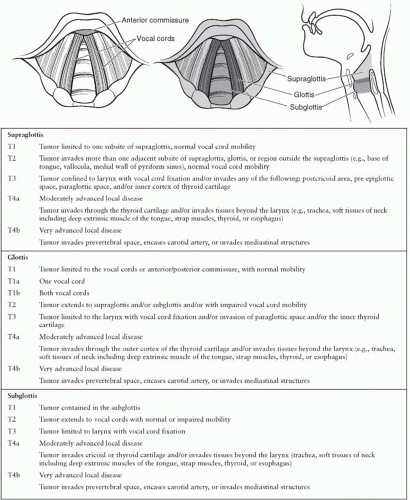
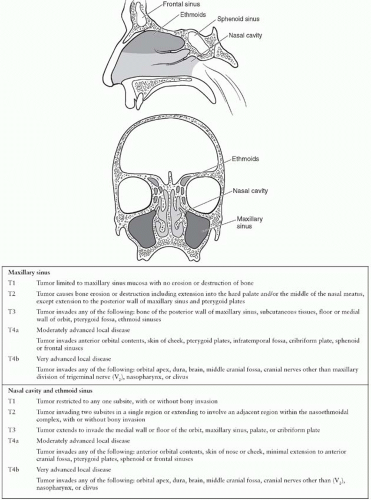
Figures 30.2 to 30.10 present the relevant anatomy and T staging of each region and the anatomy of the neck. The tumor, node, metastases (TNM) classification developed by the American Joint Committee on Cancer (AJCC) in 2010 is the standard system used to establish stage grouping and to facilitate determination of both prognosis and treatment.2 Because T stage definitions vary depending on the primary site location, these definitions are included with the primary site figures. Changes in the new edition of the AJCC for head and neck cancer reflect the aggressive nature of surgical resection. The monikers “unresectable and resectable” were changed to “very advanced and moderately advanced.” This differentiation leads to stage IV disease being split into IVa “moderately advanced local/regional disease,” IVb “very advanced local/regional disease,” and IVc “distant metastatic disease.” Neither nonepithelial tumors (lymphoid tissue, soft tissue, bone, and cartilage) nor mucosal melanomas are included in this classification system. Melanomas are discussed in Chapter 14, and thyroid cancers, which rarely lead to reconstructive procedures, will not be discussed.
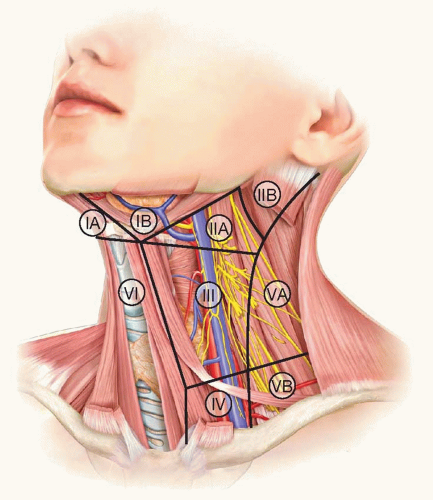
The cervical lymph nodes are a primary site of metastasis for most head and neck cancers. As such, lymph node dissection, when appropriate, is important for tumor staging. Table 30.83 defines the primary site locations of the neck. Figure 30.8 demonstrates the anatomy and regional lymph node groups of the neck. To facilitate and standardize discussion of neck metastases and neck dissection, the neck has been divided into nodal group levels.
EPIDEMIOLOGY
Although head and neck cancers are a devastating group of diseases, site- and stage-specific survival reveals that many invasive tumors exhibit a 5-year survival of over 60% (Table 30.9).4 In addition, the overall mortality for most subsets has fallen from 1997 to 2002 in almost every subsite, and most dramatically in those locations that are not readily palpable (Table 30.10).5 The incidence of squamous cell carcinoma of the head and neck has been decreasing in the United States, from 18 per 100,000 in 1974 to 14 per 100,000 in 2007,6 possibly paralleling a decrease in smoking rates. Cumulative DNA alterations caused by the synergistic effects of cigarette smoking and alcohol use are thought to underlie a majority of mucosally derived head and neck squamous cell carcinomas.
Over the past decade, there has been a spike in the incidence of head and neck tumors in younger patients. The etiology of these tumors is thought to be related to HPV virus infection, with the majority of tumors demonstrating the same serotypes (16, 18, and 31) associated with cervical cancer, a finding that is thought to be due to increased rates of oral sex. This association is most prominent in women between the ages of 15 and 34 years and occurs in the salivary glands and tongue.7,8 Fortunately, the cure rate from these cancers is higher than the typical squamous cell cancers, and recent evidence suggests that the use of the HPV vaccination for cervical cancer may also be beneficial in preventing HPV-induced head and neck cancers.
TABLE 30.1 CANCER OF THE HEAD AND NECK: 5-YEAR RELATIVE SURVIVAL RATES (%) BY AJCC STAGE (5TH EDITION) AND SITE, AGES 20+, 12 SEER AREAS, 1988-2001
▪
SITE/AJCC STAGE
▪
STAGE I
▪
STAGE II
▪
STAGE III
▪
STAGE IV
▪
UNSTAGED
Lip
96.3
82.7
75.6
48.1
88.3
Tongue
70.7
58.6
47.3
36.7
41.7
Floor of mouth
72.5
60.1
35.8
29.7
41.4
Gum and other mouth
80.9
62.2
45.1
40
49.3
Oropharynx and tonsil
56
58.3
55.4
43.4
43.8
Hypopharnyx
48.7
38.6
34.1
23.2
26.3
Salivary gland
95.7
76.7
72.6
37.2
74.1
Nasopharynx
78.4
63.7
59.5
46.7
57.8
Other oral cavity and pharynx
40.8
46.2
23.2
22.3
39.3
FIGURE 30.1. Distribution of head and neck cancer in the United States.1
TABLE 30.2 PRIMARY SITE LOCATIONS OF THE ORAL CAVITY
Lip
Skin-vermilion junction to oral mucosa and including the commissures.
Buccal mucosa
Mucosal lining extending from the pterygomandibular raphe forward. The Stensen (parotid) duct arises next to second maxillary molar.
Alveolar ridge
Gingival mucosa anterior to retromolar trigone.
Retromolar trigone
Mucosa behind the last mandibular molar tooth extending superiorly to the maxillary tuberosity.
Hard palate
Bounded by the superior alveolar ridge and the junction of the soft palate.
Floor of mouth
Bounded by the inferior alveolar ridges and the tongue. Wharton (submandibular) ducts arise in the midline.
Anterior (two-thirds) tongue (oral tongue)
Extends anteriorly from the circumvallate papillae and bounded by the floor of mouth. Motor innervation of the tongue is via the hypoglossal nerve (cranial nerve [CN] XII), whereas sensory innervation is via the lingual nerve (branch of CN V3).
TABLE 30.3 PRIMARY SITE LOCATIONS OF THE NASOPHARYNX
Hollow cavity delimited by oropharynx, hard palate, skull base, spine, and nasal cavity.
TABLE 30.4 PRIMARY SITE LOCATIONS OF THE OROPHARYNX
Soft palate
Extends from the hard palate junction to the uvula posteriorly and anterior tonsillar pillars laterally.
Tonsil
Bounded by the tonsillar pillars (faucial arch).
Lateral pharyngeal wall
Extends from posterior tonsillar pillar to posterior pharyngeal wall. The internal carotid artery, internal jugular vein, vagus and sympathetic nerves, and cranial nerves IX to XII are located in the parapharyngeal space, which is immediately lateral to the lateral pharyngeal wall.
Posterior pharyngeal wall
Bounded by lateral pharyngeal walls and extending from the level of the hard palate superiorly and the hyoid bone inferiorly.
Posterior (one-third) tongue (base of tongue)
From circumvallate papillae to epiglottis (vallecula).
TABLE 30.5 PRIMARY SITE LOCATIONS OF THE HYPOPHARYNX AND CERVICAL ESOPHAGUS
Hypopharynx
Arbitrarily divided into three anatomically contiguous regions.
Postcricoid region
Extends from the arytenoids superiorly to the cricoid cartilage inferiorly.
Posterior pharyngeal wall
Anterior to retropharyngeal space and extends from the level of the epiglottis to the level of the cricoid cartilage.
Pyriform sinus
Pyramidal in shape with a base superiorly and an apex inferiorly. Extends from the oropharynx superiorly to the laryngeal ventricles inferiorly. The medial border is the lateral cricoid cartilage while the lateral border is the medial thyroid cartilage. The posterior border is bounded by both the lateral and posterior pharyngeal walls.
Cervical esophagus
Extends from the cricoid level to the sternal notch.
TABLE 30.6 PRIMARY SITE LOCATIONS OF THE NASOPHARYNX
Consists of the supraglottis, glottis, and subglottis.
Supraglottis
Includes the epiglottis, arytenoids, aryepiglottic folds, and false cords.
Glottis
Consists of the true vocal cords, the anterior commissure, and the posterior commissure.
Subglottis
Region below the glottis extending to the inferior margin of the cricoid cartilage.
TABLE 30.7 NASAL CAVITY AND PARANASAL SINUSES
Nasal cavity
Extends superiorly from the walls of the ethmoid sinus anteriorly and the sphenoid sinus posteriorly down to the hard palate anteriorly and nasopharynx posteriorly. Lateral margins are the medial walls of the maxillary sinus and the nasal cavity is bisected sagittally by the septum.
Four paired sinuses
Maxillary sinus
Bounded superiorly by the orbital floor, inferiorly by the hard palate, posteriorly by the pterygoid plates and pterygopalatine fossa, and laterally by the pterygoid muscles and mandibular ramus.
Frontal sinus
Above and along the anterior aspect of the ethmoid sinus.
Ethmoid sinus
Between medial orbits, superior to nasal cavity.
Sphenoid sinus
Skull base, posterior to ethmoid sinus.
FIGURE 30.2. Anatomy and T staging of the oral cavity.2
FIGURE 30.3. Anatomy and T staging of the nasopharynx.2
FIGURE 30.4. Anatomy and T staging of the oropharynx.2
FIGURE 30.5. Anatomy and T staging of the hypopharynx and cervical esophagus.2
FIGURE 30.6. Anatomy and T staging of the larynx.2
FIGURE 30.7. Anatomy and T staging of the nasal cavity and paranasal sinuses.2
FIGURE 30.8. Nodal levels of the neck. 1A Submental, 1B Submandibular, II Jugulodigastric, III Middle jugular IV Low jugular, V Posterior triangle, VI pre-laryngeal/tracheal
As a result of “field cancerization,”9 the entire upper aerodigestive tract mucosa is at risk for both synchronous (5%) and metachronous (5% to 15%) second primary malignancies. Lymph node dissections are generally performed when clinically positive nodes are noted. Consideration of tracheostomy and/or gastrointestinal feeding tube should be part of the preoperative plan of any extensive resection/reconstruction of the head and neck. The surgical treatment of other oral malignancies is generally similar to squamous cell carcinoma and is outlined below.
Only gold members can continue reading. Log In or Register to continue