The lower extremity has a mechanical component and must bear weight. These functional requirements make an effective reconstruction difficult. The mechanism of lower extremity defects includes trauma, diabetes and vascular disease, cancer ablation, and other disease processes. Reconstruction of the lower extremity requires the knowledge of all plastic surgical tools, such as skin grafting, local flaps, perforator flaps, muscle flaps, microvascular free flaps, and arterial, nerve, and bone repair.
LOWER EXTREMITY TRAUMA
Treatment of high-energy lower extremity trauma with softtissue and bone injuries remains a formidable problem. These injuries often occur in the multiply injured trauma patient, making management even more difficult. Initial motor vehicle air bag designs reduced mortality and the incidence of facial fractures, but did not offer adequate protection of the lower extremities. Newer designs with multiple airbags now protect the lower extremities. Pedestrian motor vehicle accidents, falls from heights, and sporting injuries result in open tibial fractures that require the management of complex bone and softtissue injuries and may be associated with vascular and nerve injuries.
The management of lower extremity trauma has evolved to the point that many extremities, except for severely mangled extremities, are now routinely salvaged. Treatment requires a team approach consisting of orthopedic, vascular, and plastic surgeons. Fracture management utilizes techniques of external fixation, intermedullary rodding, and internal plating. Bone grafting now includes vascularized bone grafts, Ilizarov bone lengthening, artificial bone matrix and bone growth factors, and nonvascularized bone grafts. Soft-tissue management includes microvascular free tissue transfers, local muscle flaps, fasciocutaneous and perforator flaps, and skin grafts. Techniques of vascular and nerve repair have been further refined.
The goal in the treatment of open tibial fractures and lower extremity salvage is to preserve a limb that will be more functional than if it were amputated. If the extremity cannot be salvaged, the goal is to maintain the maximum functional length. The management of these injuries is a topic of debate in the literature. A severely mangled extremity may require multiple operative procedures and it may be months to years before it can be used for weight bearing and the patient can return to employment.
In a review of 72 patients with Gustilo grade IIIB open tibial fractures, Francel et al. found that despite a 93% successful limb salvage rate, a majority of patients had problems with ankle motion or leg edema. Only 28% returned to work after 42 months of mean follow-up compared with 68% of patients who had a below-knee amputation.1 Similarly, Georgiadis et al. compared 27 patients who had attempted limb salvage with 18 patients who had primary below-knee amputation. They found that patients who had limb salvage took longer to achieve full weight bearing, were less willing to return to work, and had higher hospital charges than those who had primary amputation.2
Other reviews have shown more successful outcomes with extremity salvage. Laughlin et al. reviewed the functional outcome in eight patients with grade IIIB and six with grade IIIC injuries. He found that despite a long recovery period, eight of nine patients returned to work.3 In a series of 128 patients treated at Bellevue Hospital for open tibial fractures, 66 were available for follow-up for at least 5 years. More than 60% of the patients returned to work after extremity salvage. For some patients, the delay in returning to work was as long as 10 years after the original injury. A significant cause for the delay to return to work was social factors, such as pending litigation. No patients required further reconstruction more than 5 years after their microvascular free tissue transfer. All but three patients were satisfied with their reconstructions and would do it again if they had the chance. Of the three who were dissatisfied, none were willing to convert the reconstruction to an amputation.4 In a series of 42 patients, Rodriguez et al found that of 42 patients who had lower extremity salvage with free flaps, 93% of the patients would go through the limb salvage process again to avoid amputation.5
These results appear to be favorable compared with average return to work rates of 66% for patients after lower limb amputation, with only 22% to 67% of these returning to the same occupation and the remainder changing their occupation as reported in the literature in a review by Burger et al.6 Although McKenzie et al. found that outcomes based on the Sickness Impact Profile (SIP) was equivalent at 2 and 7 years for amputees versus salvage patients,7,8 20% of patients with lower extremity fractures, not extremity salvage procedures, were not working at 30 months post injury despite low SIP scores.9 This indicates that return to work rates and SIP scores are not accurate in determining the value of lower extremity salvage. Objective functional studies need to be done to compare outcomes.
Extremity salvage is a long, complicated process. Patients must be made aware of the expected course and the anticipated functional outcome. Patient selection is an important variable in evaluating the final outcome. Although normal function is rarely achieved, most patients are grateful for their salvaged limb.
History
Amputation was practiced early in the history of man. One of the earliest writings is that of Hippocrates (460-370 BC), who described amputation as the method of last resort when faced with ischemic gangrene.
Ambroise Pare (1509-1590) described the basic rules of amputation still followed today. He recommended amputation through viable tissue and closure of amputation stumps to fit prostheses. He went on to describe phantom pain and stump revision.
The concept of immobilization was introduced by Ollier (1825-1900), who introduced the plaster cast. During the U.S. Civil War, the mortality of lower extremity injuries was 50%, secondary to sepsis. The advent of antiseptics and antibiotics decreased this mortality rate through World War I.
The “closed plaster technique” for open tibial fractures was introduced by Orr. It was further advanced during the Spanish Civil War by Trueta, who performed surgical debridement prior to placement in plaster.
During World War II, no new techniques were developed. However, improvement in aseptic technique and antibiotics decreased the mortality of wound complications from 8% in World War I to 4.5% in World War II. Nonetheless, the increased destructive capacity of military equipment in World War II resulted in a 5.3% amputation rate compared with 2% in World War I. The incidence of postfracture osteomyelitis decreased from 80% in World War I to 25% in World War II.
The next major advance in lower extremity salvage came during the Korean conflict. Lower extremity injuries during this war involved injuries to the major arteries in 59% of the cases. The concept of artery repair as opposed to artery ligation was introduced. This practice decreased the amputation rate from 62% at the beginning of the war to 13% at the end of the war, with wound mortality dropping to 2.5%.
In the late 1960s, plastic surgeons discovered the transfer of regional flaps to cover soft-tissue defects of the lower extremity. With the advent of microsurgery in the 1970s, improved techniques of bone coverage with soft tissue and of nerve repair further advanced the ability to salvage traumatic lower extremity injuries. Rates of osteomyelitis have been decreased by up to 95% in most series. The free fibular flap also solved the problem of bone gaps in these devastating injuries. The concept of bone lengthening was discovered by Codivilla much earlier and advanced by Ilizarov. It was popularized in the Western world only in the 1980s. This concept provided additional techniques to solve both bone and softtissue deficiencies.
The concept of negative pressure dressings was introduced in the 1990s by Argenta et al.10 It was found that negative pressure on a wound would decrease edema, decrease bacterial count, promote contraction of the wound, and, with the help of a sponge dressing, promote granulation.
Perforator flaps have become more effective in covering many defects of the lower extremity which once required microvascular free flaps. Many wounds that were difficult to manage now were easier to manage and enabled simpler reconstructions. Management of many lower extremity wounds requires careful evaluation to use the simplest and most effective methods.
Anatomy
The leg has several characteristics that make it unique. Humans are bipedal, thus full weight bearing in the erect position is on the two lower extremities. The full force of the weight of the body is transmitted through the legs. The muscles of the leg provide ankle function with plantarflexion, dorsiflexion, eversion, and inversion. Additional leg muscle functions include toe flexion, knee extension, and knee flexion. If the ankle were fused, the functional needs of the leg muscles are greatly unnecessary. Therefore, significant muscle loss of the leg can be tolerated with maintenance of bipedal ambulation. Consequently, muscle loss of the leg is not a contraindication to reconstruction and salvage.
The hydrostatic pressures imposed on the leg increase the incidence of edema, deep venous thrombosis, and venous stasis problems. These problems are rare in the upper extremity, but common in the lower extremity. The lower extremity is also much more commonly afflicted with atherosclerosis than the upper extremity. Therefore, both venous and arterial problems are more common in the lower extremity and must be considered when developing a reconstructive plan.
The anteromedial portion of the tibia is covered by the skin and subcutaneous fat only. This relatively unprotected anatomy leads to many instances of bone exposure, which require specialized soft-tissue coverage.
Because the full force of the body is transmitted to the feet, sensibility on the plantar aspect of the foot is necessary for normal ambulation. Normal sensibility is required for tactile sensation, position sensation, and protection of the vulnerable pressure-bearing portion of the body. Loss of the tibial nerve, with loss of sensibility on the plantar aspect of the foot, is a relative contraindication for lower extremity salvage. However, many patients with peripheral neuropathy are able to ambulate. They must remain cognizant of the potential problems; motivated patients can reasonably enjoy normal ambulation without soft-tissue breakdown. Thus, in selected patients, loss of sensation of the plantar aspect of the foot may not be an absolute contraindication for lower extremity salvage.
Bones
The bones of the leg are the tibia and the fibula. The tibia provides 85% of the weight-bearing capacity of the leg, whereas the fibula serves as a structure for muscle and fascial attachments and as a significant structural portion of the ankle joint.
The tibia is the second longest bone in the body. It articulates with the femur at the knee joint on two condyles and joins the fibula to articulate with the talus to form the ankle joint. It articulates with the fibula proximally at the tibiofibular joint and distally at the tibiofibular syndesmosis. The tibia is connected to the fibula in its midportion with the interosseous membrane. It is a classic long bone with a diaphyseal shaft with a thick cortical bone surrounding a marrow cavity. The tibia is wide proximally where it articulates with the femur and narrows to the shaft. The diaphyseal portion is usually described as three surfaces: medial, lateral, and posterior. The medial border is subcutaneous, and thus most prone to exposure during injury. The lateral surface is one of the origins of the tibialis anterior muscle and is protected by the anterior compartment muscles. The posterior surface is well protected by the soleus and gastrocnemius muscles.
The fibula is the smaller bone of the leg. It originates slightly posterior and distal to the tibia and it articulates with the posterolateral tibia. The shaft of the fibula serves as the origin of many of the muscles of the leg. Distally, it articulates with the talus and forms the lateral malleolus. Because the fibula is not weight bearing and is in a relatively protected position, it is of less concern in trauma, except when the lateral malleolus is involved. Only the proximal and distal portions of the fibula are required, and because of an independent blood supply from the peroneal artery, the central portion of fibula is an excellent source of vascularized long bone and can be sacrificed readily.
Compartments
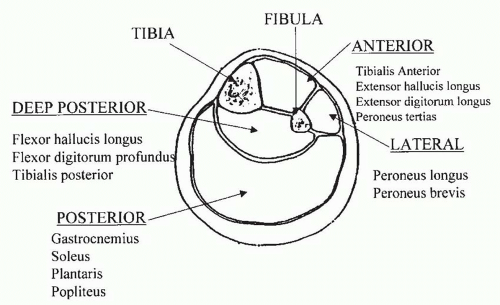
The anatomy of the leg is best understood by dividing it into its four muscle compartments: anterior, lateral, posterior, and deep posterior. The deep fascia of the leg forms discrete areas or compartments (Table 94.1 and Figure 94.1).
The anterior compartment is comprised of four muscles: the tibialis anterior, the extensor hallucis longus, the extensor digitorum longus, and the peroneus tertius. All four muscles dorsiflex the foot, but the primary dorsiflexor is the tibialis anterior, which also inverts the foot. The extensor hallucis longus primarily extends the great toe; further contraction causes foot dorsiflexion. The extensor digitorum longus extends the phalanges of the lateral four toes and dorsiflexes the foot. The peroneus tertius dorsiflexes and everts the foot. All four muscles are innervated by the deep peroneal nerve, and their blood supply is from muscular branches of the anterior tibial artery.
The lateral compartment is comprised of the peroneus longus and peroneus brevis muscles. Both muscles plantarflex and evert the foot. They are both innervated by the peroneal nerve. The vascular supply of the peroneus longus is the muscular branches of the anterior tibial and peroneal arteries. The vascular supply of the peroneus brevis is muscular branches from the peroneal artery.
The superficial posterior compartment is comprised of the gastrocnemius, soleus, plantaris, and popliteus muscles. They are all innervated by the tibial nerve. The gastrocnemius muscle plantarflexes the foot and flexes the knee. Its blood supply is from sural branches of the popliteal artery. The soleus muscle plantarflexes the foot and is supplied by the muscular branches of the posterior tibial, peroneal, and sural branches of the popliteal artery. The plantaris muscle plantarflexes the foot and is supplied by the sural branches of the popliteal. The popliteus flexes the knee and rotates the tibia and is supplied by genicular branches of the popliteal.
TABLE 94.1 COMPARTMENTS OF THE LEG
▪
COMPARTMENT
▪
MUSCLE FUNCTION
▪
NERVE
▪
ARTERY
Anterior tibialis anterior
Dorsiflex foot, invert foot
Deep peroneal nerve
Anterior tibial artery
Extensor hallucis longus
Extend great toe, dorsiflex foot
Deep peroneal nerve
Anterior tibial artery
Extensor digitorum longus
Extend toes II-V, dorsiflex foot
Deep peroneal nerve
Anterior tibial artery
Peroneus tertius
Dorsiflex foot, evert foot
Deep peroneal nerve
Anterior tibial artery
Lateral peroneus longus
Plantarflex and evert foot
Superficial peroneal nerve
Anterior tibial and peroneal artery
Peroneus brevis
Plantarflex and evert foot
Superficial peroneal nerve
Peroneal artery
Superficial posterior Gastrocnemius
Plantarflex foot, flex knee
Tibial nerve
Popliteal artery, sural branches
Soleus
Plantarflex foot
Tibial nerve
Posterior tibial, peroneal, sural
Plantaris
Plantarflex foot
Tibial nerve
Sural
Popliteus
Flex knee, rotate tibia
Tibial nerve
Popliteal, genicular branches
Deep posterior Flexor hallucis longus
Flex great toe, flex foot
Tibial nerve
Peroneal artery
Flexor digitorum profundus
Flex toes II-V, flex foot
Tibial nerve
Posterior tibial artery
Tibialis posterior
Plantarflex, invert foot
Tibial nerve
Peroneal artery
The deep posterior compartment is comprised of the flexor hallucis longus, flexor digitorum longus, and tibialis posterior muscles. They are all innervated by the tibial nerve. The flexor hallucis longus flexes the great toe and aids in plantarflexion of the foot. It is supplied by muscular branches of the peroneal artery. The flexor digitorum longus flexes the phalanges of the lateral four toes and aids in plantarflexion of the foot. It is supplied by the branches of the posterior tibial artery. The tibialis posterior plantarflexes and inverts the foot. It is supplied by muscular branches from the peroneal artery.
Compartment Syndrome
Compartment syndrome is an increase in interstitial fluid pressure within an osseofascial compartment of sufficient magnitude to cause a compromise of the microcirculation, leading to myoneural necrosis. Any crush injury to a closed compartment may lead to compartment syndrome. The literature indicates an incidence of compartment syndrome of 6% to 9% in open tibial fractures. It is important to realize that a laceration with an open fracture may not provide adequate decompression to prevent compartment syndrome.
FIGURE 94.1. Cross-sectional anatomy of the leg. Note the paucity of soft tissue over the anteromedial tibia.
The cardinal signs of compartment syndrome are pain disproportionate to the injury, pain on passive flexion or extension, and palpably swollen or tense compartments. Loss of pulses is a late sign and the presence of pulses does not rule out compartment syndrome. The definitive diagnosis is made by measuring the compartment pressure.
Various methods have been used to measure the intercompartmental pressure, including slit catheters and saline injection techniques. Although commercially produced units are available, an 18G needle flushed with saline and connected to a transducer is usually adequate. The threshold for fasciotomy is controversial. Some surgeons consider a pressure >30 mm Hg in any compartment as an indication for fasciotomy. Allen et al. considered fasciotomy when the compartment pressure was >40 mm Hg for 6 hours or was >50 mm Hg for any length of time.11 Four-compartment fasciotomy should be performed when there is any index of suspicion of compartment syndrome, as the morbidity of a fasciotomy is far less than the morbidity of ischemic necrosis of the lower extremity secondary to an untreated compartment syndrome.
Fracture Classification
Classification of open tibial fractures in relation to fracture pattern and soft-tissue injury is useful in describing injuries and prognosis. The most commonly quoted classification for open fractures is that of Gustilo (Table 94.2).
A grade IIIA injury is an open fracture with soft-tissue damage. Because it is classified as having adequate soft-tissue coverage of the fracture, it rarely requires complex plastic surgical procedures. These injuries are usually treated with local wound care, debridements, skin grafts, or simple local flaps. A grade IIIB injury involves an open fracture with periosteal stripping and bone exposure. A grade IIIC injury is an open fracture associated with an arterial injury requiring repair. Although this is the most commonly quoted classification, it remains woefully inadequate to describe the injury or to evaluate the prognosis of an open tibial fracture for which the plastic surgeon is involved. An open tibial fracture with 3 cm of periosteal stripping and exposed bone (Figure 94.2A) is not the same as an open tibial fracture with an 8-cm bone gap, 12 cm of exposed bone, and necrosis of 16 cm in all four-compartment muscles (Figure 94.2B), though they would be both classified as grade IIIB injuries. Similarly, the phrase “arterial injury requiring repair” in the classification of a grade IIIC injury is ambiguous. Some surgeons may believe it is necessary to repair a second vessel in a one-vessel leg, whereas others believe that a single vessel is an adequate blood supply to the foot. In the first case, the injury would be classified as grade IIIC; in the second case, as grade IIIB. The classification does not tale nerve injury into consideration, which is crucial in the assessment of prognosis.
TABLE 94.2 GUSTILO CLASSIFICATION OF OPEN FRACTURES OF THE TIBIA
▪
TYPE
▪
DESCRIPTION
I
Open fracture with a wound <1 cm
II
Open fracture with a wound >1 cm without extensive soft-tissue damage
III
Open fracture with extensive soft-tissue damage
IIIA
III with adequate soft-tissue coverage
IIIB
III with soft-tissue loss with periosteal stripping and bone exposure
IIIB
III with arterial injury requiring repair
Only gold members can continue reading. Log In or Register to continue