Reconstruction of the Penis
J. Joris Hage
INDICATIONS AND REQUIREMENTS
Reconstruction or de novo construction of the penis may be indicated to treat genital ambiguity or severe micropenis, to relieve gender dysphoria in female-to-male transsexuals, or to treat for accidental or (self-) inflicted traumatic loss, oncological amputation, or infection of the penis.
Genital Ambiguity
Although masculinization can be extreme in newborns presenting with ambiguous genitalia, genetic females recognized in the neonatal period should be raised as girls as it is easier to adapt the genitalia toward the female phenotype.1,2 Although feminine assignment is often favored over condemning a male patient to a life with an inadequate phallus, it is no longer necessary to routinely assign the female gender to all male newborns with ambiguous genitalia. Three key issues are to be taken into consideration when deciding on the more appropriate gender for such patients. First, the urologist and reconstructive surgeon assess the urogenital anatomy to define the surgical procedures that would be required to construct functional male external genitalia.1,2 Testosterone may be administered to assess the likelihood of penile growth, thus excluding androgen insensitivity and possibly facilitating genital reconstruction. Second, the pattern of pubertal change that can be expected at the time of adolescence must be considered by an endocrinologist. A male role is especially preferable if a male infant has an enzymatic error preventing synthesis of testosterone, because testicular architecture is usually normal. Third, a behavioral scientist assesses the social and cultural background of the newborn and the views of the parents on the most appropriate sex for their child. Unbiased sexual orientation is enhanced if the parents show no ambivalence concerning the chosen sex.1
The above considerations apply only to the newborn in whom genital ambiguity poses an emergency situation. When the diagnosis is initially established at a later age, all measures should be directed toward restoring the concordance of the phenotype with the sex of rearing.2 Moreover, there are those patients in whom no (complete) surgical correction was undertaken even though a proper diagnosis had been made early in life. Complete endocrinologic and urogenital assessment is routine prior to the initiation of reconstructive surgery for such disorders, whether they appear in pediatric, adolescent, or adult cases. Therefore, treatment of genital ambiguity disorders should be restricted to multidisciplinary teams capable of well-balanced individualized recommendations for each patient.
Gender Dysphoria
The same principles apply to the treatment to female-to-male transsexuals. Driven by the persistent and unchangeable need to eliminate the difference between the physical reality of the body and gender of the mind, transsexuals seek to adapt their bodies as optimally as possible to the sex they feel they belong to. The key issue prior to considering gender-confirming surgery is to establish beyond reasonable doubt that the transsexual feeling is genuine. The diagnosis of gender dysphoria and the determination of whether sex reassignment surgery is warranted is primarily the task of a behavioral scientist. In addition, appropriate assessment of medical conditions and the effects of the hormonal treatment on liver and other organ systems should he accomplished preoperatively by an endocrinologist. Hence, all specialists involved to collaborate closely as members of a gender team.3
Penile Loss
In male patients with penile loss as a result of amputation or infection, the remaining penile stump may prove of insufficient length causing poor personal hygiene and scrotal excoriation because of urine, as well as an inability to void when standing.4 Consultation with a behavioral scientist prior to any reconstructive procedures may prevent postoperative disappointment and frustration of phalloplasty or penile enhancement. In cases where the testes were also lost, the input of an endocrinologist is required and in oncologic patients the urologist has to be involved for proper timing of surgery. Therefore, again, a multidisciplinary approach is preferred.
SURGICAL TECHNIQUES
Reconstruction or construction of the penis should ideally aim at: (a) a reproducible one-stage procedure; (b) creation of a competent neourethra to allow urination while standing; (c) preservation or restoration of tactile and erogenous sensibility in the phallus; (d) preservation of erectile function or sufficient bulk to tolerate the insertion of a prosthetic stiffener; and (e) a result that is aesthetically acceptable to the patient. Additionally, the ideal procedure also requires (f) minimal scarring or disfigurement and (g) no functional loss in the donor area.5
Correction of Genital Ambiguity
In cases where a decision for male gender assignment has been reached in a child with a small but complete micropenis, several surgical techniques to mobilize the cavernous corpora from the pubic rami, to accentuate the penoscrotal junction, and to reduce the pubic fat may be chosen in order to make the small phallus appear more prominent.1 Gonadal tissue that is inconsistent with the male sex should be removed.
Following masculine assignment in a truly intersex patient, genital correction is similar to that of severe hypospadias. Complete cordectomy is performed to mobilize the cavernous corpora and the urethra is lengthened to bring the perineal urethral orifice to the tip of the glans. Moreover, the ventral aspect of the glans is reconstructed to give it a normal appearance. This can often be accomplished in a single stage with the neourethra being constructed proximally from the midportion of a bifid scrotum meeting a distal rotated vascularized skin flap from the hooded foreskin. If necessary, a thick non-hirsute skin graft can be used to bridge a gap of any length. The prepenile, or “shawl,” scrotum that drapes around the base of the penis can be transposed caudally at a later stage and testicular implants may be inserted.1,2
Metaidoioplasty
The techniques mentioned above compare with metaidoioplasty, in which a penile substitution with clitoral enlargement and urethral lengthening is performed in female-to-male transsexuals.6,7,8 The term metaidoioplasty is derived from the Greek with “meta” as the prefix denoting the concept of “after” or “subsequent to.” Aidoio is an archaic combining form
relating to the genitals and -plasty is the suffix derived from plastos (formed, shaped) meaning shaping. Indeed, androgen intake may stimulate the growth of the clitoris to the point where this organ can suffice as a phallus. Although metaidoioplasty is performed according to the principles of hypospadias surgery, the female external genitalia actually provide more tissue for surgical construction of a male phallus than a severe hypospadias patient has available. An overdeveloped clitoris may be distinguished from an underdeveloped penis by the frenulum on the ventral surface of the phallus. In normal males there is only a single midline frenulum, whereas in normal females there are two frenula, each lateral to the midline. Furthermore, the so-called chordae holding down the female clitoris represent the conjoined continuation of both labial spongiosus corpora toward the glans clitoris rather than solely fibrous strands present in severe hypospadias. The major labia are anterior in position to the scrotum and are “transposed” in relation to the penis. The minor labia correspond to the nonfused pendulous urethra and central penis covering, whereas the female urethral orifice is comparable to the perineal hypospadias situation.
relating to the genitals and -plasty is the suffix derived from plastos (formed, shaped) meaning shaping. Indeed, androgen intake may stimulate the growth of the clitoris to the point where this organ can suffice as a phallus. Although metaidoioplasty is performed according to the principles of hypospadias surgery, the female external genitalia actually provide more tissue for surgical construction of a male phallus than a severe hypospadias patient has available. An overdeveloped clitoris may be distinguished from an underdeveloped penis by the frenulum on the ventral surface of the phallus. In normal males there is only a single midline frenulum, whereas in normal females there are two frenula, each lateral to the midline. Furthermore, the so-called chordae holding down the female clitoris represent the conjoined continuation of both labial spongiosus corpora toward the glans clitoris rather than solely fibrous strands present in severe hypospadias. The major labia are anterior in position to the scrotum and are “transposed” in relation to the penis. The minor labia correspond to the nonfused pendulous urethra and central penis covering, whereas the female urethral orifice is comparable to the perineal hypospadias situation.
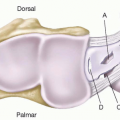
During the single-stage metaidoioplasty, the clitoris is partially released and stretched by resection of the ventral chordae and the urethra is lengthened to the tip of the glans using a pedicled musculomucosal flap raised from the anterior vaginal wall and minor labial skin (Figure 99.1). In most patients the metaidoioplasty is combined with the construction of a bifid scrotum in which testicular prostheses are implanted, hence effecting the dorsal transposition of the major labia by bilateral V-Y advancement. Metaidoioplasty allows the base of the clitoris to be advanced approximately 3 cm anteriorly.6,7,8 If provided with a sufficiently lengthened urethra this clitorispenoid will act as a normal and complete penis, albeit a small one hardly capable of sexual penetration. In female-to-male transsexuals where the clitoris seems to be large enough to provide a phallus that will satisfy the patient, this one-stage procedure is the method of choice.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


