Mohs micrographic surgery has become the standard of care for the treatment of cutaneous malignancies. Reconstructing cutaneous defects of the nose can be challenging, as form and function must be respected to the greatest extent possible. A wide range of reconstructive techniques are used. Secondary intent, primary closure, skin grafts, local flaps, and the interpolated workhorse flaps represent the spectrum of options, each with specific advantages and disadvantages. Vigilant postoperative care, including judicious use of adjunctive procedures, can improve outcomes. A subunit approach to reconstruction aids with surgical planning in order to achieve the best possible results.
Key points
- •
The paranasal region permits several flap designs based on the well-established pattern of anastomoses between the major vessels of the central face.
- •
Defect characteristics, such as size and location, as well as the principles of subunit reconstruction as outlined by Burget and Menick guide the surgeon in choosing the most appropriate type of reconstruction.
- •
Full-thickness skin grafts have a valuable place in the management of cutaneous defects of the nose, including the lower third, if applied correctly in appropriate patients.
- •
The nasal ala has unique structural properties that make reconstruction a challenge for even experienced surgeons.
- •
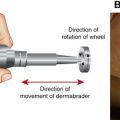
Dermabrasion, steroid injections, and staged debulking or scar revision procedures can be valuable tools in the postoperative period and can greatly improve results.
Introduction
Mohs micrographic surgery has become the standard of care for the treatment of cutaneous malignancies because of its high treatment efficacy with maximal preservation of normal tissue. Successful management includes both a sound oncologic operation as well as meticulous reconstruction.
The nose is the most common subsite of cutaneous malignancies in the head and neck, the vast majority (90%) of which are basal cell carcinomas. Of the remaining cancers, squamous cell carcinomas and melanomas are the most common. The nose is a distinctive facial feature with a complex 3-dimensional shape, a skin envelope that varies in thickness across nasal subunits, and an important functional role as an entry point to the airway. Thus, defects of the nose present unique reconstructive challenges. The surgeon must weigh multiple options across the spectrum of the reconstructive ladder and choose the most appropriate technique for both the defect and patient. Form and function must be respected to the greatest extent possible.
Surgical planning is frequently defined by the aesthetic subunit principle proposed by Burget and Menick, which emphasizes the reconstruction of topographic subunits rather than defects. This especially applies to defects that comprise a significant portion (>50%) of a nasal subunit, where reconstruction within the subunit could result in less favorable outcomes. In this approach, incisions are designed to lie within the junctions between subunits (these include the nasal dorsum, sidewalls, tip, alar lobules, and soft tissue facets) and, thus, remain hidden by the natural demarcations perceived by the human eye. A necessary component of this technique is the resection of normal skin. The surgeon must balance these principles with a defect-only approach to reconstruction, which emphasizes the preservation of native tissue and has also been applied successfully in many circumstances.
The reconstructive ladder for post-Mohs cutaneous defects consists of healing by secondary intention; skin grafting; recruitment of local tissue; and the 2 interpolated workhorse flaps, the forehead flap and the melolabial flap. Cutaneous defects may be accompanied by defects of the nasal framework and/or the internal nasal lining that will need to be reconstructed simultaneously. Preserving or rebuilding structural support should be a primary goal in nasal reconstructive surgery.
Introduction
Mohs micrographic surgery has become the standard of care for the treatment of cutaneous malignancies because of its high treatment efficacy with maximal preservation of normal tissue. Successful management includes both a sound oncologic operation as well as meticulous reconstruction.
The nose is the most common subsite of cutaneous malignancies in the head and neck, the vast majority (90%) of which are basal cell carcinomas. Of the remaining cancers, squamous cell carcinomas and melanomas are the most common. The nose is a distinctive facial feature with a complex 3-dimensional shape, a skin envelope that varies in thickness across nasal subunits, and an important functional role as an entry point to the airway. Thus, defects of the nose present unique reconstructive challenges. The surgeon must weigh multiple options across the spectrum of the reconstructive ladder and choose the most appropriate technique for both the defect and patient. Form and function must be respected to the greatest extent possible.
Surgical planning is frequently defined by the aesthetic subunit principle proposed by Burget and Menick, which emphasizes the reconstruction of topographic subunits rather than defects. This especially applies to defects that comprise a significant portion (>50%) of a nasal subunit, where reconstruction within the subunit could result in less favorable outcomes. In this approach, incisions are designed to lie within the junctions between subunits (these include the nasal dorsum, sidewalls, tip, alar lobules, and soft tissue facets) and, thus, remain hidden by the natural demarcations perceived by the human eye. A necessary component of this technique is the resection of normal skin. The surgeon must balance these principles with a defect-only approach to reconstruction, which emphasizes the preservation of native tissue and has also been applied successfully in many circumstances.
The reconstructive ladder for post-Mohs cutaneous defects consists of healing by secondary intention; skin grafting; recruitment of local tissue; and the 2 interpolated workhorse flaps, the forehead flap and the melolabial flap. Cutaneous defects may be accompanied by defects of the nasal framework and/or the internal nasal lining that will need to be reconstructed simultaneously. Preserving or rebuilding structural support should be a primary goal in nasal reconstructive surgery.
Secondary intent and primary closure
Allowing cutaneous wounds to heal by secondary intent is the simplest method of reconstruction. This technique is most effective for very small (<5 mm) defects on the concave surfaces of the nose. Along with skin grafting, healing by secondary intent may serve a role when aggressive tumor characteristics warrant surveillance of the wound rather than immediate reconstruction. Small defects in the medial canthal area, the anatomy of which is easily distorted by local tissue rearrangement, are best suited to this technique. In aesthetically prominent regions of the nose, the relatively large amount of contracture can lead to poor scarring as well as alar notching or retraction. These distorting forces increase with increasing size and depth of the defect. The concavities of the alar groove, alar-facial sulcus, and naso-facial sulcus may occasionally tolerate scars from small, very superficial defects allowed to heal by secondary intention; however, these important contours can be irrevocably lost if webbing occurs across a defect that is too large or too deep. The scars themselves are less favorable, often healing with a smooth, shiny surface that is visually distracting. Overall this technique is limited and is reserved for very carefully selected patients.
Primary closure of cutaneous defects can be effective for small wounds typically less than 1 cm, although the technique is fundamentally limited by the poor mobility and stiffness of the nasal skin. Consequently, primary closure is more feasible in elderly patients who have additional skin laxity. Additionally, fusiform excisions with primary closure result in linear scars, which can have poor cosmesis depending on their location relative to the nasal subunits and relaxed skin tension lines. In the distal third, cephalocaudad vectors of tension may result in a cosmetically unfavorable distortion of the normal alar contour. This option is most effective on the nasal dorsum and sidewalls. It is appropriate in select patients but has limited applicability.
Skin grafting
Skin grafting serves an important role in nasal cutaneous reconstruction, but whether it is aesthetically comparable with local skin flaps is a matter of debate. In general skin grafts are a viable option for defects less than 2 cm in size. Full-thickness skin grafts are preferred as split-thickness grafts tend to have excessive contraction and poor recipient site match. Initial skin graft survival depends on stable contact with a vascularized defect bed, and the use of bolster dressings is required. A common criticism of skin grafting for nasal reconstruction is that it can result in discrepancies in thickness and color that may provide a poor match to the recipient site. This criticism is in contrast to local repair techniques, which are conversely more affected by centripetal forces of contraction that lead to pincushion deformities. The common donor sites for full-thickness skin grafts used in nasal reconstruction include preauricular, supraclavicular, forehead, and postauricular full-thickness skin.
When contemplating skin graft resurfacing of a cutaneous nasal defect, thickness of the nasal skin is an essential consideration that is both highly patient and defect specific. Defects in the upper two-thirds of the nose are particularly amenable to skin grafting because of the flat-to-concave contours of these regions and the relative thinness of the nasal skin. In the lower third, increased skin thickness and convexity of the nasal tip contours make successful utilization of full-thickness skin grafts a more challenging problem. Ethnicity also has a profound influence on skin thickness and sebaceous quality. Where a large discrepancy between graft and donor site exists, the tendency is to heal with an obvious depression at the reconstructed site. Careful patient selection and operative technique can help ameliorate these difficulties and allow for successful reconstruction of these areas with skin grafts.
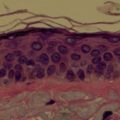
The authors’ experience with full-thickness skin graft reconstruction of cutaneous nasal defects challenges the notion that local flaps are superior to skin grafts. The senior author (DMT) conducted a retrospective study of 103 nasal cutaneous reconstructions comparing 39 patients with full-thickness skin graft reconstruction with 64 patients undergoing local reconstruction. Outcomes were assessed on visual analog scales by independent observers blinded to reconstructive technique. By this method, skin grafts were found to have equivalent cosmetic outcomes and required significantly fewer postoperative triamcinolone injections than the local flap group. In contrast, rates of postoperative dermabrasion were not statistically different. This technique represents a good option for single-stage reconstruction with potentially fewer postoperative interventions. The keys to the successful use of skin grafting likely include the use of preauricular skin as a donor site and certain patient characteristics, such as thin, less sebaceous skin and Fitzpatrick I or II skin type. Additionally, thickness discrepancies in the nasal tip were managed with the inclusion of cartilage grafts in the defect deep to the skin graft with preservation of a layer of vascularized tissue in between. Using these techniques, defects of the dorsum, sidewalls, tip, and ala were all reconstructed successfully. The thoughtful application of full-thickness skin grafting in appropriate patients can be an important tool for reconstructing cutaneous nasal defects, including defects of the lower third ( Fig. 1 ).
Local flaps
Bilobed Flap
There have been countless local flap designs described throughout the literature for the purpose of cutaneous nasal reconstruction; however, the bilobed double transposition flap is the most well established and widely used. These flaps can be used effectively for defects of the sidewalls, dorsum, and lower third less than 1.5 cm in diameter and a safe distance (>5 mm) from the alar margin. Thin nasal skin is preferable for this type of reconstruction, as thick sebaceous skin is more prone to pincushion deformities.
The flap is designed as a random-pattern double transposition flap rotated over an arc of 90° to 180° that recruits full-thickness cephalic skin into a more caudally positioned defect. Skin is, thus, rotated into the defect from an area of relative laxity. The double flap design allows greater dispersion of tension compared with a single transposition flap, such as a rhombic or note flap. The original description of this flap described tissue transposition over two 90° arcs. This description has subsequently been modified, most significantly by Zitelli, who demonstrated the utility of limiting the arc of rotation to a total arc length of 90° to 100° with individual arcs of 45° between the two flaps. Burget and Menick described the flap as a musculocutaneous flap incorporating the underlying muscle layer further increasing the flaps blood supply and survivability. The authors think the incorporation of the muscle layer significantly improves the vascularity of the flap and allows closure of larger defects.
Bilobed flaps are most useful for defects of the lower two-thirds of the nose. As the defect site is moved cephalically into the upper third of the nose, necessary recruitment of donor skin from the medial canthal or glabellar region begins to limit the applicability of the flap. Defects of the lateral ala also deserve caution when considering bilobed flaps, as important facial contours are lost when a flap traverses the alar crease or alar-facial sulcus. The lobes of the bilobed flap (Burget design) are based on a musculocutaneous blood supply and are preferably based laterally, but a medial base can be appropriate given the generally robust vascular supply of the nasal skin-soft tissue-muscle envelope. A laterally based flap design additionally allows for placement of the standing cutaneous deformity within or parallel to the alar groove for optimal cosmesis.
The pivot point is set at a distance of one radius away from the margin of the defect at the desired location, accounting for the standing cutaneous deformity that occurs at this point. Often this is placed within or parallel to the alar groove. Two arcs centered on the previously determined pivot point are then drawn out from the center and periphery of the defect. The distance between these two arcs helps configure the shape and size of the transposition flaps. Each lobe should be nearly the same width of the defect given the relatively inelastic nature of the nasal skin. The first lobe is designed between the greater and lesser arcs, with its linear axis 45° from that of the defect. The second lobe is placed 45° to the axis of the primary lobe and often extends in a triangular fashion beyond the path defined by the arcs to a distance that is twice the height of the primary lobe. This placement serves to facilitate adequate closure of the secondary donor site. The length of the secondary lobe can be modified based on flap location and elasticity of the skin.
Full-thickness incisions are carried out as designed. Dissection is then performed below the nasal superficial musculoaponeurotic system (SMAS) to protect the vascularity of the flap. The flaps can be thinned as required, taking care to preserve the subdermal vascular plexus and as much of the underlying muscle layer as possible. Wide undermining of the surrounding skin soft tissue envelope is then performed to facilitate closure and reduce centripetal contraction. Closure is then performed in layers starting with the point of maximal tension. The order typically followed is closure of the secondary lobe donor site followed by closure of the primary defect. The standing cutaneous deformity at the pivot point is excised, and the excess skin at the tip of the secondary lobe is trimmed during inset into the primary lobe donor site ( Fig. 2 ).
Despite the effectiveness of the bilobed flap and its widespread use, a few pitfalls should be kept in mind when mobilizing local tissue for reconstruction. The underlying structure of the nose deserves some consideration. For example, excessive tension near the alar margin can lead to retraction or notching, particularly if the supporting lower lateral cartilages are thin, cephalically positioned, or weak. Distortion of soft tissues under tension in this region may also occasionally contribute to nasal valve problems in patients with weak underlying structure. To help minimize functional compromise, the authors frequently place alar batten grafts or other sidewall grafts to provide extra lateral wall support and prevent airway compromise. Pincushion deformities may develop and should be anticipated and managed with subcutaneous debulking or a secondary procedure. In patients with thicker sebaceous skin, the authors perform primary multiple Z-plasties incorporated into the flap design to lessen the postoperative pincushioning. Scarring at incisional interfaces or changes in thickness after tissue rearrangement can be managed with dermabrasion in the postoperative period. Additionally, scars tend to be long and do not necessarily fall within relaxed skin tension lines or aesthetic subunit junctions. Planning for these factors in advance and balancing them against alternative options such as full thickness skin grafting may help achieve optimal outcomes.
Dorsal Nasal Flap
The dorsal nasal flap as popularized by Rieger was designed as a random-pattern rotation-advancement extension of the glabellar flap, which could be used to cover large defects of the nose in a single-stage reconstruction. Marchac and Toth redesigned Rieger’s flap as an axial flap based on a branch of the angular artery. Many variations of the dorsal nasal and glabellar flaps are possible that take advantage of the rich anastomotic blood supply in this region, which has been extensively described and elaborated by multiple dedicated vascular studies. It is this robust anastomotic network that provides the foundation for nasal reconstruction.
By the design of this flap, glabellar and dorsal nasal skin are recruited to close relatively large defects by mobilizing a large segment of tissue. The upper size limit for defects is 2.5 cm, a limitation set by the degree of skin laxity in the glabellar region. The flap is useful for resurfacing defects of the lower third of the nose in a single stage, but there should be at least 5 mm of native tissue between the defect and the free alar margin to help prevent postoperative retraction. An inverted-V incision is typically placed within the glabellar skin below the height of the medial brow and then is extended inferiorly either ipsilateral or contralateral to the side of the lesion. It is helpful to try to place the incisions in glabellar frown lines superiorly and within the aesthetic boundary at the naso-facial junction to aid in scar camouflage. The flap is elevated in the subcutaneous plane in the glabellar region but transitions to the submuscular plane over the nasal dorsum to preserve the random blood supply to the flap. Wide undermining is usually required. The flap is then rotated into the defect and closed ( Fig. 3 ).