- •
Radiofrequency (RF) devices are a recent advancement in noninvasive technology designed to reduce the appearance of fat. Often, they are based on the emission of an electromagnetic field that results in a current running through subcutaneous tissue and causing bulk heating. These innovations are safe with low side effect profiles, and they can be used on all skin types
- •
Ideal patients for most of these procedures are healthy with relatively discrete sites of unwanted fat such as those at the abdomen, ‘love handles’, and thighs. There is no downtime associated with these procedures and they are an alternative to surgical interventions for body contouring
- •
There are multiple variations of the RF technology designed to target subcutaneous tissue. They include, but are not limited to, tripolar and unipolar devices as well as those which are based on the emission of nonionizing radiation
- •
Data remains in its early stages and is limited. However, RF devices targeting subcutaneous tissue are reported to reduce circumference of the abdomen and thighs and in some cases show a decreased thickness in subcutaneous tissue via ultrasound and histopathologic data
Introduction
A decade ago, the only reliable methods by which to reduce fat and its appearance were invasive and included procedures such as abdominoplasty and liposuction. These surgical techniques posed issues of significant downtime and potential side effects related to the procedures themselves and any necessary general anesthesia. Fortunately, within the last decade, multiple noninvasive technologies have been developed to visibly decrease the appearance of fat and, in some cases, show a histologic decrease in subcutaneous volume and a diminution of adipocyte size and integrity. Radiofrequency (RF) is a particularly interesting modality for fat reduction.
Ideal patients for radiofrequency-induced fat reduction are healthy with a normal BMI and discrete areas of unwanted fat such as those located at the abdomen, waist and thighs.
When speaking of cosmetic interventions, the first RF device was Federal Drug Administration (FDA)-approved for wrinkle reduction in 2002 (ThermaCool ® , Thermage ® , Haywood, CA). Currently, RF is applied to a much broader range of treatments including skin rejuvenation, tightening and wrinkle reduction, acne and acne scarring, improved appearance of cellulite, and fat reduction. Its wide array of applications can be explained by a multitude of unique and specific RF technologies that have been developed, several of which are applied for fat reduction.
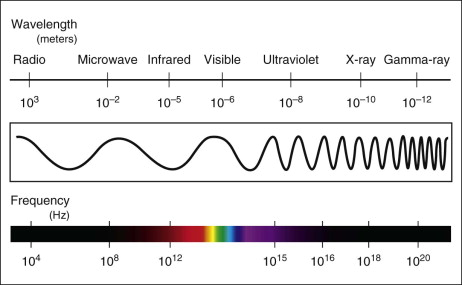
Radiofrequency refers to radiation at the far end of the electromagnetic spectrum, which has a frequency between 3 kHz and 300 MHz ( Fig. 7.1 ). Energy emitted at these frequencies is not strong enough to be ionizing. Unlike laser devices, which emit energy in the form of a unique wavelength of light, RF devices emit energy in the form of electromagnetic waves that induce an alternating current in the targeted tissue. Tissue is composed of individual molecules, which are electrical dipoles. When current or electrons flow through a material, the dipoles align with the current and then change orientation millions of times per second as the current alternates. Each tissue type has a unique resistance to this movement of molecules, otherwise known as impedance. The movement of dipoles against resistance can be thought of as a type of friction that leads to energy in the form of heat, thereby converting electrical energy into thermal energy. By Ohm’s law, energy emitted by an RF device is proportional to the current it produces (I), the specific impedance of a particular tissue (Z) and time (t):
Energy(joules)=I2×Z×t
Importantly, RF devices have some advantages over lasers that allow them to target subcutaneous tissue. Electromagnetic waves lose energy exponentially as they travel across tissue. High frequencies and small wavelengths used by laser light attenuate quickly, while RF energy does not and is therefore able to penetrate deeper fatty tissue. RF is not dissipated by scatter or absorbed by epidermal melanin, and, unlike some forms of laser energy, all skin types may be treated with RF. The effect of laser energy is described by the concept of selective photothermolysis and is relatively pinpointed. Conversely, the fact that RF energy is not localized is important for causing bulk heating, which is a quality necessary to reach adequate treatment temperatures in larger areas. When correct frequencies are chosen, subcutaneous tissue may be particularly targeted for heating.
Technology and mechanism of action
Crucially, RF results in heating when applied to tissue. In ex vivo analysis, when adipocytes are heated, their viability decreases. To illustrate this, Franco and colleagues demonstrated that 3 days after cultured adipocytes are heated to 45 °C and 50 °C, there is only 89% and 20% viability of cells, respectively. Cells heated to 45 °C for 3 minutes show only 40% viability. At least one group has demonstrated that heating secondary to RF causes cell-mediated death or apoptosis. RF technology makes use of this adipocyte instability in order to reduce its appearance and/or volume.
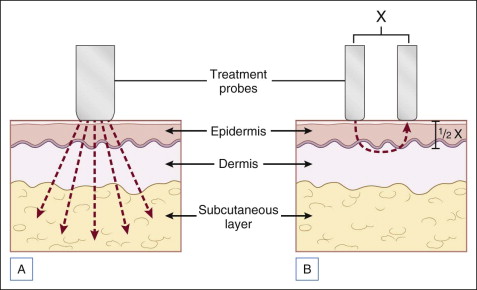
Historically speaking, RF devices were either monopolar or bipolar. Monopolar describes a system in which the electric current is dispelled by a handpiece into the skin and exits the body through a grounding pad. This allows for deep penetration and was initially utilized in electrosurgery. Safety concerns and high pain levels may be associated with this type of device. Bipolar describes a system in which electric current moves between two electrodes at the surface of an intended treatment site. Compared with monopolar systems, they are more limited in the depth they can achieve, which is approximately half the distance between two electrodes ( Fig. 7.2 ).
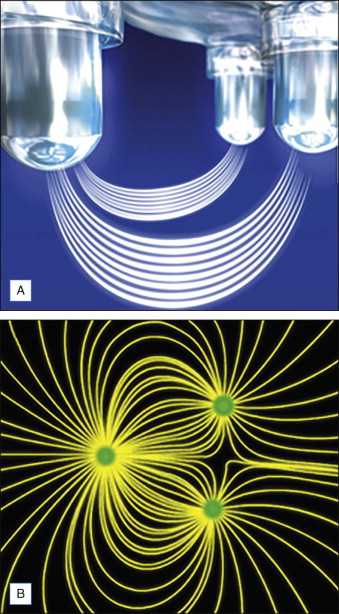
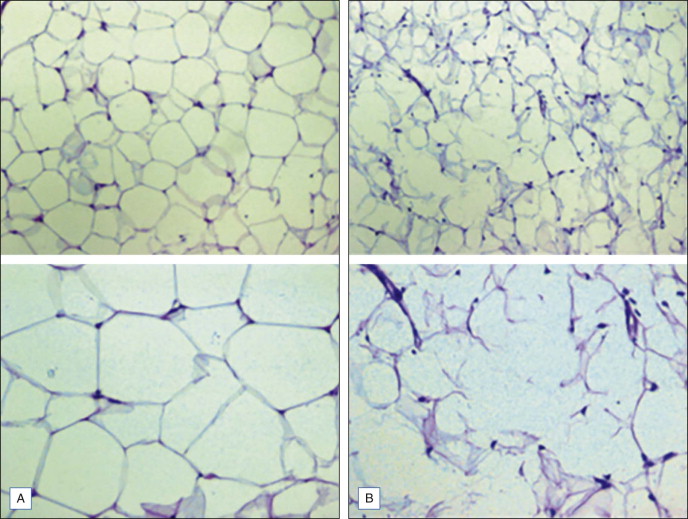
Groups that have marketed RF devices for fat reduction have taken technology several steps further. Pollogen ® Ltd (Tel Aviv, Israel) has developed a line of RF devices with three electrodes, referred to as TriPollar ® technology. In this design, current flows from one positive to two independent negative electrodes ( Fig. 7.3 ) to produce uniform but relatively deep heating. Both the Regen XL™ and Apollo™ devices emit a frequency of 1 MHz at 30 to 50 W and have been shown to have destructive effects on adipocytes. Boisnic and Branchet performed an ex vivo study on 12 skin samples from eight abdominoplasty patients treated locally with the Apollo™ device (50 W). They reported an increased glycerol level from the hypodermis of treated skin (5610.2 nm/g) compared to untreated skin (2549.4 nm/g) suggesting increased lipolysis in treated skin. Of the skin samples they evaluated histologically, two of four showed inhomogeneity of adipocyte membranes, which were elongated and irregular at some sectors with partial rupture of cell walls. One sample showed a necrotic area of adipocytes. These results suggest direct effects of RF on adipocyte membrane integrity ( Fig. 7.4 ). In a second trial, an at-home tripolar device showed similar increased glycerol release in eight skin samples compared with controls: 4180.8 nM/g vs 2301.8 nM/g. In the same study, 34% of adipocytes were modified in shape with inhomogeneity, elongation, irregularity and membrane changes including partial rupture. Unfortunately, the study was limited in that it did not report the percentage of change in untreated tissue. Finally, Kaplan and Gat demonstrated similar changes to adipocytes in a patient treated with the Regen™ device (30 W). This patient consented to histologic analysis following seven weekly treatments. Dermal thickness increased by 49% compared with untreated skin, though thickness of the subcutaneous layer appeared unchanged between treated and untreated skin.
Histologic changes in adipocytes have been reported with additional RF technologies. Trelles et al. employed an automatic multi-frequency and low impedance RF device (ThermaLipo™, Thermamedic Ltd, Alicante, Spain), which emits at a lower frequency (0.6 MHz) to target deeper tissues and at higher frequency (2.4 MHz) for more superficial tissue. Thirty women were treated with this device at the buttocks for at least four passes in order to reach a skin temperature of 42 °C maintained for a minimum of 12 minutes. Skin biopsies were taken prior to and 2 hours after RF treatment and stained with H&E and Oil red O separately. In all samples, adipocytes lost their typically round shape and became more polyhedric and rectangular. Degeneration of the cellular membrane was observed as well as vacuolization of fat and decreased fat. Some cells appeared necrotic.
Effective radiofrequency fat reduction requires that the skin is maintained at ≈40–42 °C for several minutes and multiple passes. Since fat is a good insulator, the temperature of the skin may not always be an indicator of fat temperature. A series of treatments may provide improved results.
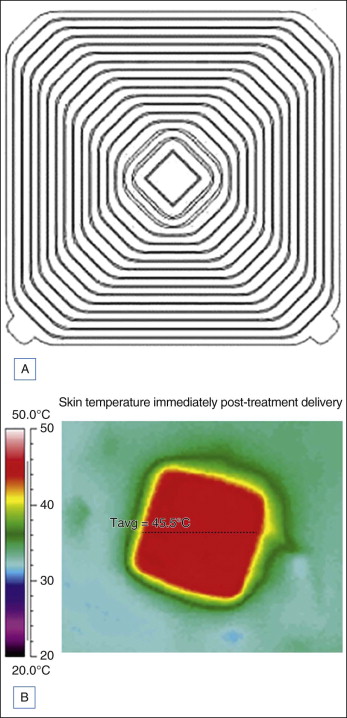
Another recent and unique RF design includes an applicator consisting of a series of tightly spaced concentric rings that are designed to couple energy into tissue across the entire surface of the applicator (truSculpt™, Cutera ® , Brisbane, CA) ( Fig. 7.5 ). The distribution of surface electric potential is controlled by adjusting frequency to create uniform heating at specified volumes. Electric fields are created in a perpendicular manner to the dermal–subcutaneous junction resulting in significant, targeted heating of the fat. This was demonstrated in two subjects in whom temperature probes were inserted at the cutaneous–subcutaneous junction, 7 mm into the subcutaneous tissue, and 12 mm into the subcutaneous tissue during general anesthesia induced for planned abdominoplasty. The truSculpt device was applied for 3 minutes and probes reported that the temperature of the cutaneous–subcutaneous junction remained <30 °C while the temperatures at 7 mm and 12 mm reached 45 °C and 50 °C, respectively. Resulting subcutaneous changes are shown by another phase of the same study in which three patients were treated for 22 minutes prior to abdominoplasty and then underwent biopsies of the treated sites. Epidermal and dermal structures were normal in all biopsies and the subcutaneous tissue appeared normal immediately after the procedure. Yet, beginning at day 4, adipose tissue showed vascular alterations including purpura, congested vessels and increased vascularity. Adipocyte necrosis was noted at day 9 in one patient and at days 17 and 24 in a second patient while increased macrophages and foamy histiocytes were noted on day 10 in a third patient. The authors suggest that fat is disposed of and therefore volumetrically decreased by phagocytosis in a gradual manner that does not lead to hyperlipidemia.