| Functional ptosis affecting vision |
| Cosmetically displeasing ptosis |
| Need for levator advancement but without excess dermatochalasis |
| Ptosis affecting prosthesis in anophthalmic socket |
| Ptosis repair in non-Asians when crease fixation is not necessary |
| Prior facial surgery or trauma |
| Dry eye symptoms/lagophthalmos present |
| Quality of Bell’s phenomenon |
| Prior refractive surgery |
| Co-existent eyebrow ptosis |
| Amount of levator function |
| Need to avoid posterior conjunctival ptosis repair (i.e., strabismus, glaucoma filtration surgery/drainage device, cicatricial conjunctival diseases, fornix shortening) |
| Degree of ptosis present |
| Rule out myasthenia gravis |
| Presence of Hering’s reflex |
| Potential for revision/asymmetry |
Introduction
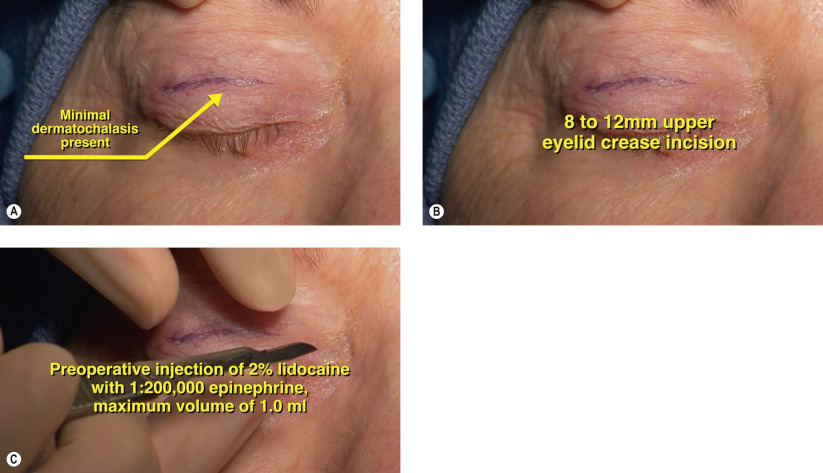
Small incision levator advancement compared to traditional external levator advancement ( Chapter 11 ) is performed through an incision less than 12 mm. The procedure is ideally suited when a levator advancement is needed but when an upper blepharoplasty is not necessary. In patients who have failed posterior approach ptosis repairs, small incision levator advancement may be considered. For the Asian patient who desires a well-defined eyelid crease, the small incision approach may not be suitable, as this does not allow for wide crease fixation across the entire eyelid. Typically only one suture is required for levator advancement with the small incision approach and the lateral and medial horns of the levator are left undisturbed. As with any levator technique, this procedure is performed under local anesthesia with minimal IV sedation to ensure optimal levator function. See Chapter 11 for a more detailed discussion of the preoperative evaluation.
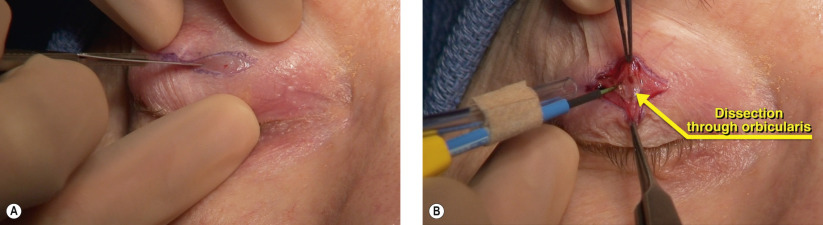
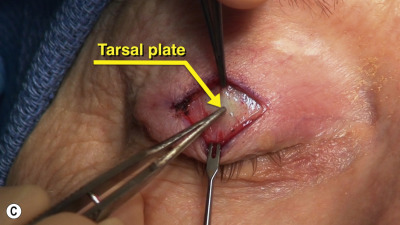
Surgical Technique