Abstract
Psychocutaneous diseases are commonly encountered in the practice of dermatology, and many affected individuals lack insight into their condition or refuse a psychiatric referral. With a systematic approach to evaluation and treatment, such patients can be successfully managed by dermatologists. Psychodermatologic disorders can be conceptualized in two ways: (1) by the type of psychodermatologic condition – primary psychiatric disorder, secondary psychiatric disorder, psychogenic pruritus and dysesthesia, or psychophysiologic disorder; or (2) by the symptom complex and diagnostic pattern of the underlying psychopathology – anxiety, depression, psychosis, and/or obsession–compulsion. Treatment utilizing psychopharmacologic agents and non-pharmacologic therapies can be directed by the underlying psychopathology. This chapter reviews selected primary and secondary psychiatric conditions that are frequently seen by dermatologists.
Keywords
psychocutaneous, psychodermatology, delusions of parasitosis, body dysmorphic disorder, trichotillomania, excoriation (skin-picking) disorder, acne excoriée, dermatitis artefacta, body-focused repetitive behavior, nonsuicidal self-injury, psychopharmacology
Introduction
“Psychodermatology” refers to any aspect of dermatology in which psychological factors play a significant role. At least a third of patients seen in dermatology practices require consideration of associated emotional and psychosocial factors for effective management of their skin condition .
Many patients with psychodermatologic problems resist referral to a mental health professional, and some become upset if such a referral is suggested. Ironically, the individuals who are the most psychologically “ill” often have the least insight into the psychogenic nature of their condition and frequently refuse a psychiatric referral. The dermatologist is then faced with two choices. The first is to try to address the psychological condition. If a dermatologist decides to take this route, it is necessary to be familiar with the approach to diagnosis, therapeutic options (both pharmacologic and non-pharmacologic, including potential side effects of medications), and limitations of what can be accomplished in a dermatology practice. The other option is to disregard the psychological problem and allow this component of the patient’s disorder to remain untreated, which is not optimal. Dermatologists can learn to effectively handle psychodermatologic issues within the limits of their training and practice setting. Although less comprehensive than treatment delivered in collaboration with a psychiatrist, in the authors’ opinion, management of these issues by a dermatologist is better than no treatment at all.
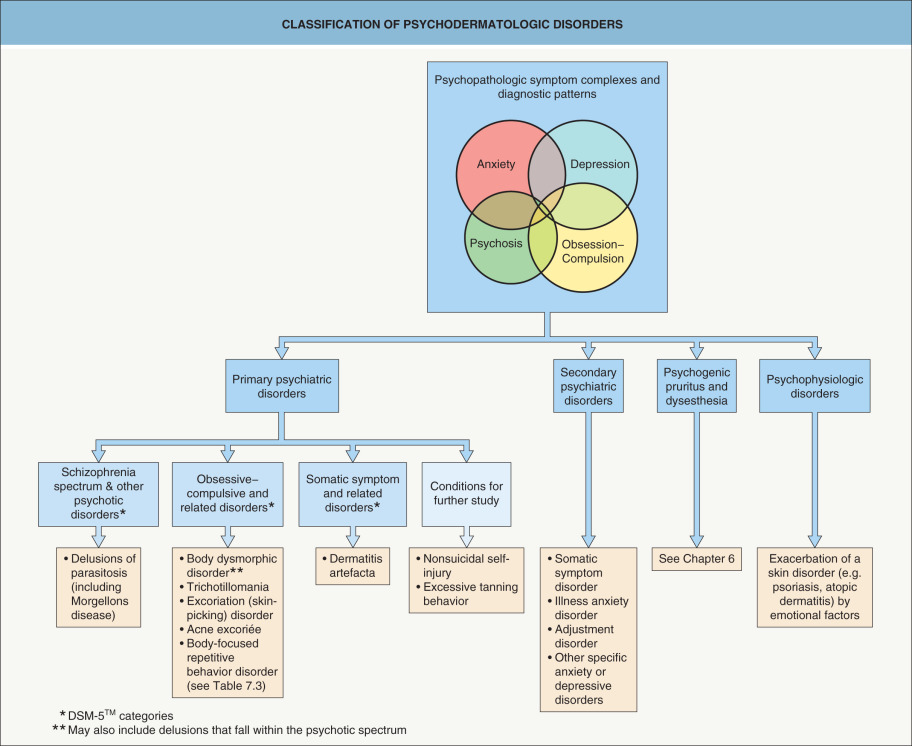
Clinically useful methods of conceptualizing and classifying psychodermatologic disorders are presented in Fig. 7.1 . This incorporates updates from the fifth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5™) . Selected primary and secondary psychiatric conditions that are commonly encountered in a dermatologic practice are discussed in this chapter. Strategies for the evaluation and management of patients with these disorders are reviewed, including pharmacologic and non-pharmacologic treatments. Disorders characterized by pruritus and dysesthesia are covered in Chapter 6 .
Overview
Psychodermatologic disorders can be conceptualized in two ways: (1) by the specific psychodermatologic condition; or (2) by the symptom complex and diagnostic pattern of the underlying psychopathology, including anxiety, depression, psychosis, and obsession–compulsion. The latter approach is useful because knowledge of the psychopathologic manifestations enables the clinician to choose the most appropriate psychopharmacologic agent ( Table 7.1 ). For example, if the underlying psychopathology involves obsessions and/or compulsions, a selective serotonin reuptake inhibitor (SSRI; e.g. fluoxetine) would be a logical choice of therapy .
| PSYCHOPATHOLOGIC PATTERNS AND PSYCHOTROPIC MEDICATIONS USED IN DERMATOLOGY | ||
|---|---|---|
| Underlying psychopathology and symptom complex | Possible pharmacologic treatment | Comments and precautions |
| Anxiety | ||
| Acute anxiety: Benzodiazepines
|
|
Chronic anxiety: Non-benzodiazepines – start low and titrate slowly
|
| |
| Depression | ||
|
|
|
|
| |
| Psychosis | ||
|
|
|
|
| |
| Obsessive–compulsive disorder (OCD) | ||
|
|
|
|
| |
|
| |
In the classification method based on psychodermatologic conditions, most patients can be grouped into one of four categories (see Fig. 7.1 ):
- •
primary psychiatric disorders , in which the patient has no primary skin disease and all of the cutaneous findings are self-induced, as in delusions of parasitosis
- •
secondary psychiatric disorders , in which the patient develops psychological problems as a result of a skin disease
- •
psychogenic pruritus and dysesthesia , in which the patient presents with a purely sensory complaint (e.g. pruritus, burning, stinging) without evidence of a primary skin disease or underlying medical condition (see Ch. 6 )
- •
psychophysiologic disorders , in which a primary skin disorder (e.g. atopic dermatitis) is exacerbated by emotional factors (e.g. anxiety)
Primary Psychiatric Disorders With Dermatologic Manifestations
Delusions of Parasitosis
▪ Delusional parasitosis ▪ Delusional infestation ▪ Ekbom syndrome
- ▪
Fixed, false belief that the skin is infested with parasites
- ▪
May experience sensations of biting, crawling, or stinging
- ▪
Need to distinguish from substance-induced formication
- ▪
Requires treatment with an antipsychotic medication
Introduction
Delusions of parasitosis is classified as a somatic type of delusional disorder (previously referred to as monosymptomatic hypochondriacal psychosis) within the broad group of schizophrenia spectrum and other psychotic disorders . Delusions are defined as fixed beliefs that are not amenable to change despite conflicting evidence, and somatic delusions are focused on bodily functions or sensations. Individuals with delusions of parasitosis have the isolated, fixed belief that their skin is infested by parasites, in the absence of any objective evidence of infestation .
Clinical features
Patients with delusions of parasitosis do not meet criteria for a diagnosis of schizophrenia. However, they should fulfill the DSM-5™ diagnostic criteria for a delusional disorder which are: (1) the delusion must be present for ≥1 month; (2) the patient does not exhibit impaired functioning or bizarre behavior apart from the impact of the delusion; and (3) the delusion cannot be attributable to the effects of a substance, medication, medical condition, or other psychiatric disorder . The delusional belief is “encapsulated”, i.e. there is a narrow and specific focus on skin infestation. Patients may be able to state that others view their beliefs as irrational (“factual insight”), but they lack the true insight necessary to personally accept the valid explanation.
Individuals with delusions of parasitosis typically present with a history of symptoms for months or even years. They have often already been evaluated by many physicians and have tried to eradicate their alleged “parasites” by methods such as using pesticides, hiring exterminators, or changing their residence. Patients frequently bring in bits of skin, lint, and other samples that they believe represent “parasites”, which is referred to as the “matchbox sign” ( Fig. 7.2 ). They may report cutaneous sensations of crawling, biting, or stinging.

Skin findings in delusions of parasitosis range from none to excoriations, lichenification, prurigo nodularis, and ulcerations (see Fig. 7.2 ). All of these are self-induced, usually resulting from the patient’s efforts to dig out “parasites”.
One intriguing aspect of this disorder is the potential for a shared delusional system whereby the patient’s close contacts come to believe in the delusion as well. Folie à deux (“craziness for two”) is the term used to describe two people who share the same delusion. Occasionally, larger numbers of people harbor the same delusion, which may include the patient’s parent(s) and children .
Morgellons disease is a controversial condition with manifestations that fall within the spectrum of delusions of parasitosis . A hallmark of this disorder is that patients claim to observe “ fibers ” exuding from their skin, and it has received widespread media and Internet coverage. Multiple articles in the medical literature and investigation by the Centers for Disease Control and Prevention support the categorization of Morgellons disease as a form of delusions of parasitosis .
Epidemiology
The average age of onset is 55–60 years . Among individuals over 50 years of age, women experience the disorder twice as often as men; however, prior to age 50, men and women are equally affected. Younger patients with this disorder are usually of a lower socio-economic status and may have a history of substance abuse, while older patients are frequently of a higher socio-economic status.
Differential diagnosis
Delusions of parasitosis is distinct from formication , which represents a tactile hallucination involving the sensation of “bugs” crawling within or biting the skin. Formication does not involve a fixed, false belief that the sensations are caused by a skin infestation. Formication and/or delusions of skin infestation can result from use of drugs, especially amphetamines and cocaine (see Ch. 89 ). As noted above, patients with delusions due to the effects of a substance, medication, medical condition (e.g. true skin infestation, neurologic disorder), or other psychiatric disorder (e.g. schizophrenia, depression with psychotic features) are excluded from diagnosis of delusions of parasitosis.
Management
One of the most challenging aspects of management is getting patients with delusions of parasitosis to agree to take an antipsychotic medication. The first step is to establish rapport and address their concerns seriously without challenging their beliefs, making sure to do a thorough dermatologic examination. When discussing the diagnosis with the patient, communicate it in a matter-of-fact manner and refrain from making any statements that may be misinterpreted by the patient as supporting his/her delusional ideation. Often, it is more feasible to present the antipsychotic medication as one that may work empirically for symptoms of formication and agitation rather than to confront the individual about psychiatric issues. If the medication is presented in an objective and pragmatic manner, the patient may have less difficulty accepting it as a therapy.
The treatment of choice for delusions of parasitosis has traditionally been pimozide ( Tables 7.1 and 7.2 ). As part of the discussion on therapy, the dermatologist should explain to the patient that he or she does not have Tourette syndrome (the FDA-approved indication for pimozide) or schizophrenia. There have been multiple reports of successful treatment of delusions of parasitosis with atypical antipsychotic medications (e.g. risperidone, olanzapine, aripiprazole), which have more favorable side-effect profiles (see Tables 7.1 and 7.2 ). Patients with delusions of parasitosis can often be successfully tapered off medication after 2–6 months of therapy.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


