Psoriasis, seborrheic dermatitis, pityriasis rosea, and lichen planus are diseases that present with papulosquamous lesions (scaly papules and plaques). Although these diseases may have a similar morphology, their underlying etiologies vary. Secondary syphilis, cutaneous T-cell lymphomas, and connective tissue disease may also present with papulosquamous lesions and should be included in the differential diagnosis.
Psoriasis is a common, chronic, inflammatory disease that can result in decreased quality of life. Clinicians have long been vexed by this ancient affliction. Although most medical literature prior to Willan (1757-1812) lumped psoriasis, leprosy, eczema, and other inflammatory dermatoses into a confusing menagerie, Celsus gave a convincing account of psoriasis vulgaris almost 2000 years ago. His description included many of the morphologic features that physicians today utilize to diagnose psoriasis, including the “ruddy” or salmon-colored plaques with silvery scales that often are associated with punctate hemorrhage or “erosions” when removed.1
More than 7.5 million adults (2.1% of the population) in the United States are affected and 30% of these individuals will develop psoriatic arthritis.2 About 1.5 million of them are considered to have moderate to severe disease. Psoriasis may have a significant negative impact on a patient’s quality of life. Patient often are self-conscious, depressed, or frustrated over the appearance of their skin.
Psoriasis spans all socioeconomic groups, and its prevalence varies by geographic location. Historically, the disease is more common in the northern latitudes. The rate of psoriatic disease is lower in African Americans compared with that in European Americans.2
The primary cause of psoriasis is a dysregulation of the cell-mediated, adaptive immune response. This dysregulation is likely triggered by hyperactivity of the innate immunological surveillance system to environmental antigens. In genetically predisposed individuals, the Th1 pathway response is overstimulated. This overproduction of Th1-related cytokines along with IL-12, 17, and 23 causes hyperproliferation of epidermal keratinocytes. These events lead to the formation of the psoriatic plaques.3
Environmental factors and disease states that interact with polygenic inheritance patterns most likely account for the variable expression of psoriatic disease. These include streptococcal pharyngitis (guttate psoriasis), stressful life events, low humidity, human immunodeficiency virus (HIV), trauma, medications, cold, and obesity. Diets high in fish oils seem to be protective against the development of psoriasis.2,4
Most patients with mild to moderate psoriasis are asymptomatic, but pruritus is common in severe or widespread disease. Patients may also give a history of joint pain and swelling, especially in the fingers and toes.
Psoriasis can vary in appearance and distribution. However, there are clues in the physical examination that allow the clinician to properly diagnose psoriasis and identify its subtypes.
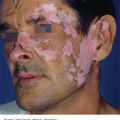
Plaque-type psoriasis vulgaris accounts for 90% of all cases. The primary lesion is a scaly, red- to salmon-pink-colored papule that expands centrifugally to form a similarly colored plaque (Figure 9-1). It is usually covered by a white or silvery scale that, when removed, may show pinpoint bleeding (Auspitz sign). Its border may be red and with time central clearing may occur, with the plaques taking on an annular or arcuate configuration. Plaque-type psoriasis is classically an extensor disease often involving the knees, elbows (Figure 9-2), gluteal cleft, lumbosacral region, and the umbilicus. Psoriasis may involve the scalp (Figure 9-3). Psoriatic plaques may occur in an area after trauma, pressure, or injury. This is known as the Koebner phenomenon.
Inverse psoriasis presents with thin pink plaques with minimal scale in the axillae (Figure 9-4), inguinal and inframammary area, and body folds of the trunk. It may occur in conjunction with typical plaque psoriasis or it may be the only manifestation of psoriasis.
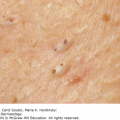
Guttate psoriasis occurs in less than 2% of cases, but it is a common psoriatic subtype in young adults. It is characterized by small “droplet-like” thin pink to salmon-colored papules and plaques surmounted by a fine white scale (Figure 9-5). The distribution is often similar to that of classic pityriasis rosea, favoring the trunk, abdomen, and upper thighs and fading toward the acral surfaces and sparing the palms and soles.
Pustular psoriasis (von Zumbusch) is an acute variant of the disease that presents with small, monomorphic sterile pustules surmounting painful, inflamed, erythematous papules. Fever, systemic symptoms, and an elevated white blood cell count often accompany generalized pustular psoriasis. Acral pustules, usually without systemic symptoms, characterize palmoplantar pustulosis (Figure 9-6), which is a milder, but more common presentation of pustular psoriasis.
Erythrodermic psoriasis is a skin reaction pattern of total body redness and desquamation of the skin. There are many causes of erythroderma and it is not specific to psoriasis. The massive shedding of skin that occurs during an erythrodermic flare of psoriasis can result in infection, hypothermia, protein loss, hypoalbuminuria, dehydration, and electrolyte disturbances.4
Psoriatic nails can be seen in up to 50% of patients with psoriasis. It may be the only manifestation of psoriasis. It is recognized that nail disease is more closely linked with psoriatic joint disease. Up to 90% of patients with psoriatic arthritis have nail disease.4 Nail dystrophies associated with psoriasis include pitting, onycholysis (nail plate separation), oil spots (yellow-orange subungual discoloration), thickening, and subungual debris (Figure 20-3). Splinter hemorrhages may also be present.






Blood work is generally not necessary to make a diagnosis of psoriasis. Pustular flares of psoriasis during pregnancy may be associated with hypocalcemia. A biopsy is often helpful if the diagnosis is unclear. A punch biopsy of a plaque or pustule often supports the diagnosis. A biopsy is warranted in any patient not responding as expected to traditional therapy. The microscopic findings of common plaque-type psoriasis are epidermal hyperplasia, parakeratosis, thinning of the granular layer, epidermal infiltration of neutrophils, and occasional “Munro abscesses” (intraepithelial collections of neutrophils).
The key diagnostic clinical features of psoriasis are red to pink plaques with silvery white scale on the elbows, knees, scalp, and lower back and legs.
| Diseases | Clinical Presentation |
|---|---|
| Psoriasis | Asymptomatic or mildly pruritic, pink-red plaques with white scale on scalp and extensor extremities. Bimodal age of onset at 22 and 55 years |
| Seborrheic dermatitis | Asymptomatic or mildly pruritic pink patches with fine greasy white scale on the scalp, eyebrows, ears, nasolabial folds, and central chest. More common in infants or after age 40 |
| Pityriasis rosea | Asymptomatic 1-2 cm oval thin plaques with a fine central scale, a larger 2-10 cm “herald patch” may precede rash. Lasts 6-8 weeks. More common in teens and young adults |
| Nummular dermatitis | Pruritic well-defined pink scaly plaques on extremities but not necessarily on elbows and knees |
| Lichen planus | Pruritic violaceous flat-topped papules on volar wrists, forearms, ankles, and lower back |
| Subacute cutaneous lupus | Annular erythematous scaly plaques in sun-exposed areas and on trunk |
| Tinea corporis | Asymptomatic or mildly pruritic pink scaly plaques with a scaly border and central clearing |
| Secondary syphilis | Asymptomatic scaly papules or plaques on palms, soles, and trunk. History of preceding genital ulcer |
| Cutaneous T-cell lymphoma (mycosis fungoides) | Asymptomatic or mildly pruritic scaly well-defined plaques with random distribution. Lesions may also be annular or arcuate and are chronic and persist in the same location. Typically presents after age 50 |
Topical steroids are the first-line treatment of mild to moderate psoriasis. They act as a foundation on which to build a therapeutic regimen for more severe disease. While topical regimens demonstrate efficacy in clinical trials, the response to these agents in everyday practice is often variable. Frequently, this is a result of poor compliance. Ointments are the most effective vehicles for psoriasis, but they stain clothing and bedding. Creams are better patient-accepted vehicles for the face, neck, and hands. Solutions and foams are appropriate for the scalp. Table 9-2 contains commonly used topical medications for psoriasis.
| Generic Name | Trade Name Examples | Formulations | Uses |
|---|---|---|---|
| Topical steroids | |||
Clobetasol Betamethasone dipropionate Fluocinonide | Temovate Diprosone Lidex | Cream, gel, ointment, solution, foam, shampoo 0.05% Cream, gel, ointment, solution 0.05% Cream, ointment 0.05% | Super to high-potency steroids for use on localized areas of thick plaques on extremities and trunk BID initially for 2-4 weeks and then alternate with calcipotriene or calcitriol. Use solutions and foams and/or shampoos for scalp |
| Triamcinolone | Cream, ointment 0.1% | Medium-potency steroid for chronic use to widespread plaques on extremities and trunk BID | |
Desonide Hydrocortisone | DesOwen Hytone | Cream, ointment 0.05% Cream, ointment 2.5%, 1% | Low-potency steroids for use on psoriasis face, groin, axillae in adults or psoriasis in children BID |
| Topical calcineurin inhibitors | |||
Tacrolimus Pimecrolimus | Protopic Elidel | Ointment 0.03%, 0.1% Cream 1% | Psoriasis on face, axillae, groin, and genitals BID |
| Topical vitamin D3 analogues | |||
Calcipotriol (calcipotriene) Calcitriol | Dovonex Vectical | Cream, solution 0.005% Ointment | Typically used in combination therapy with topical steroids in adults. Weekly dose should not exceed 100 g |
| Calcipotriene + betamethasone dipropionate | Taclonex | Ointment, suspension, spray | For use in adults >18 years old for up to 4 weeks. Should not be used on face, axillae, or groin. Weekly dose should not exceed 100 g |
| Topical retinoid | |||
| Tazarotene | Tazorac | Cream, gel 0.05%, 0.1% | For use in thick plaques in adults in combination with topical steroids. Pregnancy category X |
| Topical salicylic acid | |||
| Salicylic acid | Kerlalyt Scalpicin | Gel 3%, 6%; solution 3%, shampoo 3% | For use in thick plaques in combination with topical steroids |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


