Acne and related pilosebaceous disorders rarely cause serious systemic problems, but they are among the diseases that can cause significant psychosocial distress. Most of these disorders are chronic and require long-term therapy with topical and if needed, oral antibiotics. However, there are increasing concerns about the development of bacterial resistance to antibiotics, especially in patients with acne and rosacea who may take antibiotics for several years.1
The prevalence of acne in adolescents has been reported to be as high as 95% with a 20% to 35% prevalence of moderate to severe acne.2 Acne may persist into adulthood in up to 50% of affected individuals.3 Transient acne may occur in newborns and occasionally acne will begin in adulthood.
Quality of life issues are a very important concern for individuals (especially teenagers) with acne. Depression, anxiety, and low self-esteem are more common in patients with acne.4 Interestingly, there is no correlation between acne severity and degree of the mental health symptoms. Most clinicians who regularly treat acne (and parents of teenagers) are aware of the negative emotional impact of even a few “pimples.”
The pathogenesis of acne is complex, but there are several major factors that contribute to the development of an acne lesion.2,3
Hyperproliferation and adhesion of keratinocytes in the distal portion of the hair follicle creates a keratin plug (microcomedone).
Androgenic hormones stimulate increased sebum production.
Propionibacterium acnes (P. acnes), an anaerobic, lipophilic, resident bacteria, proliferates in the sebum-rich environment of the plugged hair follicle.
P. acnes and other factors trigger the release of inflammatory mediators that diffuse through the wall of the follicle into the surrounding dermis resulting in an inflammatory papule or pustule.
The follicular wall ruptures and bacteria, sebum, and other follicular components are released into the dermis creating an inflamed nodule.
Several other factors such as genetics and emotional stress and affect the development and severity of acne.
Acne usually presents at the onset of puberty with comedones on the central face. Inflammatory papules and/or pustules may develop in early to mid-teen years and are usually confined to the face, but the neck and back may be affected. Patients with nodular acne may complain of pain and tenderness. Acne is typically a chronic disorder that does not begin to resolve until the late teens.
Acne typically presents with 4 types of lesions, comedones, inflammatory papules, pustules, and nodules. In the past the term “cystic acne” was used, but acne does not have true cysts with an epithelial lining. However, large fluctuant nodules do have a cystic appearance. Acne typically is categorized according to the predominant type of lesions seen.3
Comedonal acne: Patients present with open comedones (blackheads) with a central dark keratin plugs and/or closed comedones (whiteheads) with no visible keratin plug (Figure 15-1). These are usually the first lesions of acne seen in early adolescence and are typically on the central face.
Papular/pustular acne: Patients present with inflamed, 2- to 5-mm papules and/or pustules (Figure 15-2).
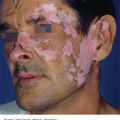
Nodular acne: Patients present with red, firm, or fluctuant nodules (cyst like) that may drain or form sinus tracts (Figure 15-3). These lesions may leave permanent scars. When these lesions are extensive and severe, the term “acne conglobata” is used.



Acne lesions are usually primarily on the face, but can also occur on the neck, upper trunk, and shoulders. Patients may have one or multiple types of acne lesions at any one time. As acne lesions resolve they may leave pink macules that may persist for many weeks or areas of hyperpigmentation that may last for months. These macular lesions are often as cosmetically bothersome to a patient as the active acne lesions. Patients often refer to these lesions as “scars,” but they do eventually resolve. Inflammatory lesions may leave permanent scars that may be indented (ice pick scars), atrophic, or hypertrophic.
Acne may be classified as mild, moderate or severe depending on the number and/or size of the lesions and the extent of the lesions.
Routine laboratory testing is not indicated in most patients with acne.5 However patients with evidence of androgen excess (eg, early puberty, hirsutism, alopecia, and infertility) should have an evaluation that could include serum testosterone, dehydroepiandrosterone sulfate (DHEA-S), and luteinizing hormone/follicle stimulating hormone (LH/FSH) ratio. Bacterial cultures of pustules could be done if gram-negative folliculitis is suspected.5 This presents with multiple pustules in the perinasal and perioral area.
The key diagnostic findings are the presence of comedones and inflammatory papules, pustules or nodules typically on the face, neck, or upper trunk.
✓ Milia: Resemble closed comedones and have the appearance of a tiny, white, firm bead. They are more common in young children and older adults.
✓ Keratosis pilaris: Very common finding in prepubescent children and may persist into adulthood. It presents with 1- to 2-mm keratotic papules typically on the cheeks and upper arms. Inflammatory papules and pustules are usually not seen.
✓ Table 15-1 has additional diseases in the differential diagnosis.
| Disease | Clinical Findings | Notes |
|---|---|---|
| Acne | Comedones, inflammatory papules, and/or pustules or nodules typically on the face. May also occur on neck and upper trunk | Onset after puberty, but may persist into adulthood |
| Rosacea | Erythema, telangiectasia, inflammatory papules, and/or pustules on central face. No comedones | Onset usually after age 30. Chronic course |
| Perioral dermatitis | Perioral erythema with or without scale with papules and/or pustules | Most common in females, ages 20-45. May recur |
| Folliculitis | Perifollicular inflammatory papules or pustules in hair-bearing areas | Onset after puberty. May recur intermittently or be chronic |
| Hidradenitis suppurativa | Inflammatory papules and abscesses in axillae and inguinal areas. Sinus tracts and scarring may be present | Onset in early 20s. Chronic course |
There are many factors to consider in the treatment of acne including the following.
Type, severity, and extent of the acne lesions.
Efficacy of mediations.
Adverse reactions, risks, and contraindications of medications.
Age, gender, and risk of pregnancy during treatment.
Adherence/compliance issues.
Cost of medications and office visits. In general generic dermatologic medications are much more affordable than branded medications.6
Patient’s (and parent’s) level of distress with acne and their concerns about potential side effects of medications.
Several topical and oral medications are available for the treatment of acne. Table 15-2 lists formulations and brand names of several of the more commonly used topical medications.
| Generic Name | Brand Names Examples | Formulation Examples | Notes |
|---|---|---|---|
| Retinoids | |||
| Tretinoin* | Retin-A, Avita, Refissa, Tretin-X | Cream, 0.025%, 0.05%, and 0.1% Gel, 0.01%, 0.025%, 0.04%, 0.1% | Start treatment with lower concentrations apply nightly. May be drying. Pregnancy category C |
| Adapalene* | Differin | Cream, 0.1% Gel, 0.1%, 0.3% Lotion, 0.1% | May be better tolerated than tretinoin. Apply nightly. Pregnancy category C |
| Tazarotene | Tazorac | Cream, 0.1% Gel, 0.1% | More effective, but more irritating than other retinoids. Apply nightly. Teratogenic. Pregnancy category X |
| Antibiotics and medications with antimicrobial effects | |||
| Benzoyl peroxide* | Benzac, Brevoxyl, Clearasil, Panoxyl | Cream, 5%,10% Gel, 2.5%, 4%, 5%, 8%, 10% Wash 2.5% | May reduce bacterial resistance to antibiotics. Apply daily. May cause irritant or allergic contact dermatitis. Pregnancy category C |
| Clindamycin* | Cleocin T, Clindagel, Evoclin | Gel, lotion, foam, pledget, 1% | Most effective of the topical antibiotics. Apply twice daily. Pregnancy category B |
| Dapsone | Aczone | Gel, 5% | Apply twice daily. May turn skin orange if used with benzoyl peroxide. Pregnancy category C |
| Erythromycin* | Several generics | Gel, ointment, solution, 2% | Antibiotic resistance may develop. Apply twice daily. Pregnancy category B |
| Azelaic acid | Azelex | Cream 20% | Has comedolytic effect. Apply twice daily. Pregnancy category B |
| Sodium sulfacetamide* | Klaron | Lotion 10% | May be drying. Apply twice daily. Pregnancy category C |
| Sodium sulfacetamide with sulfur* | Clenia Rosula | Cream, 10% sodium sulfacetamide, and 5% sulfur Foam, 10% sodium sulfacetamide, and 4% sulfur | Has antibacterial and keratolytic effects. Apply twice daily. May have a sulfur odor. Pregnancy category C |
| Combination medications | |||
| Tretinoin + clindamycin | Ziana | Gel, tretinoin 0.025% + clindamycin 1.2% | Apply nightly. Effective for papular/pustular acne. Pregnancy category C |
| Adapalene + benzoyl peroxide | Epiduo | Gel, adapalene 0.1% + benzoyl peroxide 2.5% | Apply daily. Effective for papular/pustular acne. Pregnancy category C |
| Benzoyl peroxide + clindamycin* | Duac Benzaclin | Gel, benzoyl peroxide 5% + clindamycin 1% | Apply twice daily. Effective for papular/pustular acne. Pregnancy category C |
| Benzoyl peroxide + erythromycin* | Benzamycin Gel Pak | Gel, benzoyl peroxide 5% + erythromycin 1% | Apply twice daily. Effective for papular/pustular acne. Pregnancy category C |
| Benzoyl Peroxide + hydrocortisone | Vanoxide HC | Lotion, benzoyl peroxide 5% + hydrocortisone 0.5% | May be helpful in patients who cannot tolerate benzoyl peroxide without hydrocortisone. Apply 1 to 3 times daily. Pregnancy category C |
Table 15-3 lists dosage, dosing, and some of the adverse effects of oral antibiotics that are commonly used as first-line treatment for acne when oral antibiotics are indicated.
| Medication | Formulations | Dosing | Notes |
|---|---|---|---|
| Tetracycline* | 250, 500 mg | 500 mg once daily to twice daily | Needs to be taken on empty stomach. Pregnancy category D |
| Doxycycline* | 50, 100 mg | 50-100 mg once daily to twice daily | May cause photosensitivity and dyspepsia. Pregnancy category D |
| Minocycline* | 50, 100 mg | 50-100 mg once daily to twice daily | Can be taken with food. Potential adverse effects include skin discoloration, vertigo and other central nervous system symptoms, hepatitis, and lupus-like syndromes. Pregnancy category D |
| Erythromycin* | 125, 250, 333 mg | 250-500 mg once to twice daily | May cause gastric irritation and diarrhea. Bacterial resistance may occur. Pregnancy category B |
Topical retinoids decrease the cohesiveness of the keratinocytes in the follicular opening, reduce the number of visible comedones, and inhibit formation of microcomedones. They are effective as monotherapy for comedonal acne and in combination with other medications for all other forms of acne. Dryness, redness, and peeling are common side effects with initial use, but these often resolve or improve with continued use. It is best to start with a low concentration of a retinoid and increase as tolerated. Published guidelines recommend the use of retinoids for maintenance therapy.3,5
Benzoyl peroxide has antibacterial properties and it reduces the risk of P. acnes resistance when used in combination with oral or topical antibiotics.1,3,5 Benzoyl peroxide is widely available in many types of vehicles in nonprescription and prescription formulations. As with retinoids, it is best to start with lower concentrations. Benzoyl peroxide may cause irritant or allergic contact dermatitis and it may bleach fabrics.
Salicylic acid is a mildly keratolytic agent that is present in many nonprescription medications.
Topical antibiotics are effective medications for inflammatory acne lesions when they are combined with retinoids and benzoyl peroxide. They are typically not used as a monotherapy for acne.
Azelaic acid has antibacterial and comedolytic effects on acne. It also may decrease postinflammatory hyperpigmentation in acne lesions. It is rated pregnancy category B.
Topical combination acne medications typically contain a retinoid or benzoyl peroxide with an antibiotic or with each other. In general, they are much more expensive than their constituents used separately, but they are easier to use and have better patient acceptance and adherence.3
Oral antibiotics are typically used for moderate to severe papular/pustular or nodular acne. Tetracycline, doxycycline, and minocycline are the most commonly used antibiotics for acne because of their antibacterial and anti-inflammatory effects. These antibiotics should not be used by pregnant or nursing females or by children under age 8. Doxycycline and minocycline are generally recommended in the literature as the antibiotics of first choice.3,5 Erythromycin is an alternative in patients who have a contraindication for the use of the tetracyclines. However bacterial resistance often develops during erythromycin therapy.5 Dosing commonly recommended in textbooks is included in Table 15-3.7 Trimethoprim–sulfamethoxazole (eg, Bactrim, Septra DS) is another alternative, second-line, antibiotic for short-term use that is included in guidelines for acne therapy; however, it has a potential for severe adverse reactions (eg, aplastic anemia, hepatic necrosis, and toxic epidermal necrolysis). Amoxicillin is also occasionally used for patients who have gastrointestinal symptoms with other antibiotics. It is rated pregnancy category B. Candida vaginal infections can occur with chronic use of antibiotics. The development of P. acnes and commensal flora resistance to antibiotics used in the treatment of acne is noted in guidelines as an increasing concern.1,2,3,5 In general, guidelines recommend that oral antibiotics should be discontinued, when possible, once inflammatory lesions have resolved and if chronic antibiotic therapy is needed, benzoyl peroxide gel or wash should be added to decrease the risk of bacterial resistance to antibiotics.
Oral isotretinoin is US Food and Drug Administration (FDA) approved for patients with severe recalcitrant nodular acne who are unresponsive to conventional therapy, including systemic antibiotics. It is typically prescribed for a 20-week course. Isotretinoin is a teratogen with a very high risk for severe birth defects if taken during pregnancy in any amount, even for a short period of time. Isotretinoin can only be prescribed by clinicians who participate in a special restricted distribution program (iPLEDGE). There are several other potential adverse effects (eg, cutaneous, neurological, skeletal, and lipid disorders) associated with isotretinoin. Typically because of the complexity of the iPLEDGE program and the risks of isotretinoin, most primary care clinicians refer patients who are potential candidates for isotretinoin to dermatology. Evidence-based guidelines still recommend the use of isotretinoin in the appropriate patient.2,3,5
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


