Arthropods have always feasted on humans and humans have tried countless strategies to keep them from doing so. The societal burden of biting and sucking bugs is significant, costing millions of dollars, tremendous discomfort, and immeasurable emotional distress. They bite, we itch, we scratch, and these facts seem destined to endure.
Scabies is a common parasitic infection caused by the mite Sarcoptes scabiei var hominis. Transmission is primarily person-to-person by direct contact and although anyone is susceptible, situations that result in more skin-to-skin contact, such as parents with small children, sexual activity, overcrowding, and institutional settings, increase the incidence of infestation. Although the scabies mite has not been shown to transmit any significant pathogens, the intense itching associated with the infestation, the risk of superinfection of excoriated skin, and the fact that up to 300 million people may be affected worldwide annually make scabies a significant public health problem.1
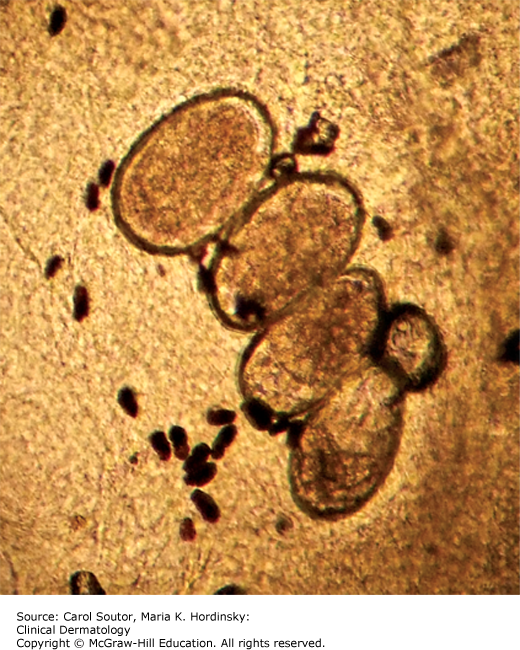
Sarcoptes scabiei is an obligate human parasite that completes its entire 30-day life cycle within the epidermis. The fertilized female weaves through the epidermis and leaves a trail of 60 to 90 eggs and feces (scybala), in her burrow (Figure 13-1). The eggs hatch into larvae that then mature into nymphs and adults. The rash and pruritus of scabies is a result of a hypersensitivity reaction to the mite and its detritus. The incubation period from infestation to pruritus can range from days to months. The first time an individual is infested, it typically takes 2 to 6 weeks to become sensitized and develop symptoms, but in subsequent infestations, the previously hypersensitized individual can begin itching in as little as 1 to 3 days. Some infested individuals never develop hypersensitivity to the mite and never experience symptoms, but can still transmit the infection; these are asymptomatic “carriers.”

Intense pruritus is the main presenting complaint, although very young children who cannot verbalize itching are often irritable and eat and sleep poorly. Adults often complain that the pruritus is worse at night. Family members and close contacts frequently report similar symptoms.
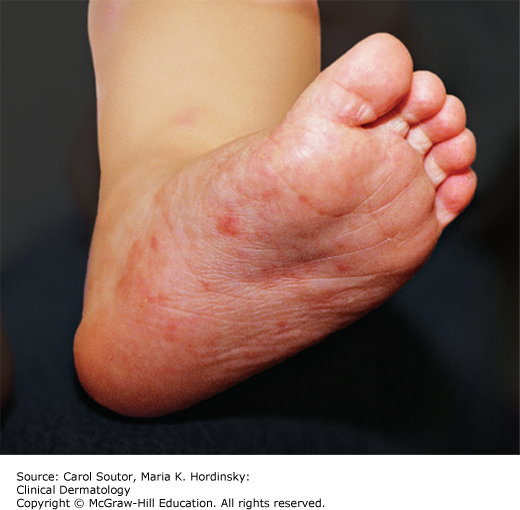
The patient presenting with scabies usually has a nondescript, excoriated, papular dermatitis. The most common physical findings are papules, vesicles, pustules, or nodules. These typically occur on the trunk, arms, hands (Figures 13-2 and 13-3), and genitals in adults and may also involve the head, neck, and feet in infants and young children (Figures 13-4 and 13-5). The burrow, a short, wavy line, is pathognomic of scabies and is typically seen on the wrists, finger webs, and penis (Figures 13-1 and 13-3).



Less common presentations include nodular, bullous, and crusted scabies.2
Nodular scabies: This typically presents with a few salmon-colored pruritic nodules usually seen in the axillae, groin, and male genitalia. Nodular scabies is a hypersensitivity reaction that typically occurs after a successfully treated scabies infestation and does not necessarily indicate active infection.
Bullous scabies: While blisters commonly occur on the palms and soles of infants infested with scabies, bullous scabies is a more extensive bullous eruption, most commonly seen in elderly adults. It is often confused with bullous pemphigoid.
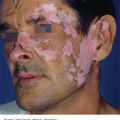
Crusted (Norwegian) scabies: This presents with thick, crusted or scaly plaques and is often confused with psoriasis. Crusted scabies typically affects the immunocompromised, elderly, disabled, or debilitated individuals. These patients often do not exhibit typical pruritus and scratching and are often infested with thousands of mites. They are highly contagious.
Table 4-3 has instructions for collection and examination of a scabies preparation. The presence of a mite, eggs, or scybala in a scabies preparation confirms the diagnosis (Figures 13-6 and 13-7). Scraping the skin for a scabies specimen is not always easy to do without injuring the patient, particularly if that patient is a squirming child; therefore, other identification techniques have been suggested. Dermoscopy has shown to be a sensitive tool for mite identification.3 Another method is to firmly apply adhesive tape to a burrow, pull it off rapidly and then transfer the tape to a slide for microscopic identification. This has also been shown to be an inexpensive, easy and relatively sensitive way to identify burrow contents.3

The key diagnostic features of scabies are intensely pruritic papules, vesicles or burrows in the finger webs, wrists, breast, axillae, abdomen, or genitals. In children, the lesions can be in any location including the head, neck, or feet.
Scabies should be considered in the differential diagnosis of any patient who presents with an intensely pruritic, eczematous rash of recent onset, especially if family members and other close contacts have similar complaints. Scabies is often misdiagnosed as the following diseases.
✓ Atopic dermatitis: Presents with scaly, often crusted, pruritic papules and plaques on the face, and flexural areas in patients with a personal or family history of atopy. Scabies may be difficult to diagnose in patients who have moderate to severe atopic dermatitis.
✓ Body and pubic lice: Presents with pruritus and lice on the body or clothing.
✓ Other arthropod bites: There are no burrows present.
✓ Dermatitis herpetiformis: Presents with lesions very similar to scabies on the elbows, knees, and lower back. The genitals are not affected.
✓ Other: Fiberglass dermatitis, tinea corporis, drug rash, lichen planus, contact dermatitis, dyshidrotic dermatitis, prurigo, delusions of parasitosis, acropustulosis of infancy.
Scabies is usually a clinical diagnosis. A patient can be treated based on a suspicious history and clinical presentation. Prescription scabicides are necessary to treat scabies. No over the counter medications are approved for scabies treatment. Table 13-1 outlines scabies treatment options. Permethrin 5% cream is the most effective treatment, according to the Cochrane Review which has the largest review of interventions for treating scabies.4 The cream should be applied at bedtime and spread thoroughly from neck to soles, including under the fingernails and toenails. In children under two, permethrin cream should also be applied to the head and neck and mittens or socks should be placed on the hands to avoid rubbing the cream into the eyes. Patients should remove the cream after 8 to 14 hours by showering or bathing. Oral ivermectin, although not approved by the Federal Food and Drug Administration (FDA) for the treatment of scabies, is easier to use and may result in improved treatment compliance. Two doses of ivermectin are required to achieve cure rates equivalent to one application of permethrin cream.5 Crusted scabies requires a more aggressive approach, with a combination of 5% permethrin every 2 to 3 days for up to 2 weeks and oral ivermectin in 3 to 7 doses over approximately 1 to 4 weeks, depending on the severity of infection.5
Medications for treatment of scabies.
| Generic & Brand Names | Administration | Age Restrictions & Pregnancy Category | Risks | Comments |
|---|---|---|---|---|
| Permethrin cream 5% (Elimite, Acticin) | Apply from neck down (include head and neck in infants and young children). Include skin folds (but not mucous membranes) and under nails. Wash off in 8-14 h | FDA approved for scabies in infants age ≥2 months Pregnancy Category B | Mild transient stinging or burning | Considered treatment of choice for scabies. Efficacy of 1 versus 2 applications has not been established. CDC and others recommend repeat treatment 1 week after the first |
| Lindane lotion or cream 1% (Kwell) | Apply thin layer from neck down, leave on overnight and wash off | FDA approved for scabies. Infants, children, elderly or those who weigh <110 lbs are at greater risk for toxicity Pregnancy Category C | Black box warning for risks for seizures and death with repeated use Contraindicated in patients with sores or inflamed skin in application area | Considered a second or third line therapy2 |
| Crotamiton cream and lotion 10% (Eurax) | Apply for 24 h, rinse off, and then reapply for additional 24 h | FDA approved for scabies in adults Pregnancy Category C | No major safety issues | Frequent treatment failures reported |
| Ivermectin tablet 3 mg (Stromectol) | Single dose 200 mcg/kg orally Appropriate dose for 50 kg patient is 10 mg Take on empty stomach with water. Total of 2 doses at least 7 days apart may be necessary5 | Not FDA approved for scabies Safety in children <15 kg and in pregnant women has not been established Pregnancy Category C | Most reported toxicity seen in treatment of filarial parasites5 | Consider in patients who have failed treatment with or who cannot tolerate FDA-approved topical medications Two doses required to achieve cure rate similar to single application of permethrin5 |
Fomite transmission is not considered a major problem in typical scabies infestations and scabies mites generally do not survive more than 2 to 3 days off human skin. Bedding, clothing, and towels used by infested persons or their close contacts anytime during the 3 days before treatment should be washed in hot water and dried in a hot dryer, dry-cleaned or sealed in a plastic bag for at least 72 hours. Persons who had close contact with an infested individual should be evaluated and treated appropriately.
The pruritus from scabies is a result of patient hypersensitivity and neither the immune response nor the itching resolves immediately after treatment. Patients should be advised that it takes up to 4 weeks for symptoms to resolve despite effective treatment. If pruritus persists beyond a month, the patient should be reexamined and if evidence of active infestation is present, the possibilities of poor treatment compliance, reinfestation, or mite scabicide resistance should be considered and addressed.
If symptoms persist despite two courses of appropriate therapy, consider dermatologic consultation. A number of eczematous and vesiculobullous conditions can mimic the presenting signs and symptoms of scabies and occasionally scabies treatment can cause secondary dermatologic sequelae that require intervention.
Scabies. Centers for Disease Control: www.cdc.gov/parasites/scabies/biology.html
Scabies Tutorial. Medline Plus. National Institutes of Health: www.nlm.nih.gov/medlineplus/tutorials/scabies/htm/index.htm
Scabies. American Academy of Dermatology: www.aad.org/skin-conditions/dermatology-a-to-z/scabies
Human lice are bloodsucking, wingless insects that have been feeding on mankind for thousands of years.2 Head, crab, and body lice remain a bane in modern times, with hundreds of millions of cases of pediculosis worldwide annually.
Head lice are the most common of the three pediculosis and are a ubiquitous nuisance. They are found in people of all age, sex, race, and socioeconomic class. School children ages 3 to 11, especially girls with long hair and a propensity to share hair care tools and accessories, are at greatest risk. African-American children are less commonly affected, perhaps because their hair shape or texture creates a less amenable environment for lice survival and reproduction.6
Crab (pubic) lice are transmitted primarily by sexual contact and the highest incidence is seen in men who have sex with men, ages 15 to 40.
Body lice give all lice a bad name. Not only are they associated with poor hygiene, they serve as disease vectors for epidemic typhus, relapsing fever, trench fever, and bacillary angiomatosis or endocarditis.2,7
All three lice species are obligate human parasites that feed exclusively on human blood and do not survive for long off their human host. They vary in size, shape, and preference for body area location.
The head louse, Pediculosis capitis, as the name suggests, favors scalp hair. It is light tan to medium brown and is about the size of a sesame seed (Figure 13-8). Although it is unable to jump or fly, it moves extremely quickly and thus can be difficult to see. The female louse lives about 30 days and lays 5 to 10 eggs a day. Oval egg capsules or nits are cemented to hair shafts close to the scalp for warmth (Figure 13-9). Transmission is via direct contact or by fomites such as combs, brushes, hats, helmets, headphones; although static electricity and blow dryers have been shown to launch lice into the air, creating another possible mode of transmission.8
Crab lice, Phthirus pubis, are smaller and wider than head lice and resemble tiny crabs. (Figure 13-10). Often referred to as pubic lice, this is a misnomer; as crab lice are adapted to ambulate over the entire body surface. The infestation can involve not only pubic hair, but also the scalp, eyebrows, eyelashes, moustache, beard, axillae, and perianal area.
The body louse, Pediculosis corporis, at 2 to 4 mm long, is slightly larger than the head louse, but otherwise looks similar. It differs from head and crab lice in that while it feeds on humans it does not live on them; it lives in clothing and lays its eggs along the seams (Figure 13-11).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


