Abstract
Psoriasis is a common inflammatory disease of the skin. It results from a polygenic predisposition combined with environmental triggers, e.g. trauma, infections, psychological stress, medications. Susceptibility genes point to the involvement of the innate and the adaptive immune systems as well as aberrant epidermal differentiation. The underlying pathophysiology involves various classes of T cells and their interactions with dendritic cells and cells involved in innate immunity, including neutrophils and keratinocytes.
Psoriasis is characterized by sharply demarcated, scaly, erythematous plaques; less often, sterile pustules are seen. Common sites of involvement are the scalp, intergluteal fold, elbows and knees, followed by the nails, hands, feet and trunk. Psoriasis may affect other major body folds and the genitalia. Typical histologic findings include acanthosis with elongated rete ridges, hypogranulosis, hyper- and parakeratosis, dilated blood vessels, and a perivascular infiltrate of lymphocytes. A pathognomonic feature of psoriasis is the accumulation of neutrophils as spongiform pustules within the epidermis.
Psoriatic arthritis is the major associated systemic manifestation, and the most common presentation is asymmetric oligoarthritis of the small joints of the hands and feet. Other comorbidities include depression, metabolic syndrome, and cardiovascular disease, primarily in patients with moderate to severe disease.
A spectrum of treatments is available. Patients with mild disease are usually treated with topical corticosteroids and vitamin D derivatives. Other topical therapies include tar-based preparations, anthralin, calcineurin inhibitors and tazarotene. In patients with more widespread disease, traditional approaches such as photo(chemo)therapy (UVB or PUVA), methotrexate, cyclosporine, or acitretin may be required. Alternatively, targeted immunomodulators (“biologic” therapies) that are highly specific (e.g. targeting TNF-α, IL-12/23, IL-17) are increasingly being used, albeit at a greater cost than conventional approaches.
Because psoriasis is a chronic disease, it requires a long-term treatment strategy, which takes into account potential medication side effects and individual needs. Treatment strategies are often divided into a clearing phase and a maintenance phase. This chapter discusses the range of therapies available to patients with psoriasis.
Keywords
psoriasis, psoriatic arthritis, plaque psoriasis, pustular psoriasis, guttate psoriasis, inverse psoriasis, pustulosis palmaris et plantaris, targeted immunomodulators, biologic therapies, reactive arthritis, Sneddon–Wilkinson disease, subcorneal pustular dermatosis, nail psoriasis, PASI score, methotrexate
- ▪
Psoriasis is a chronic, immune-mediated disorder that results from a polygenic predisposition combined with environmental triggers, e.g. trauma, infections, medications, psychological stress
- ▪
The underlying pathophysiology involves various classes of T cells and their interactions with dendritic cells and cells involved in innate immunity, including neutrophils and keratinocytes
- ▪
Identification of susceptibility genes has pointed to a major role for the innate and adaptive immune systems as well as altered epidermal differentiation
- ▪
Sharply demarcated, scaly, erythematous plaques characterize the most common form of psoriasis; occasionally, sterile pustules are seen
- ▪
The most common sites of involvement are the scalp, elbows and knees, followed by the nails, hands, feet and trunk (including the intergluteal fold)
- ▪
Typical histologic findings include acanthosis with elongated rete ridges, hypogranulosis, hyper- and parakeratosis, dilated blood vessels, and a perivascular infiltrate of lymphocytes with neutrophils singly or within aggregates in the epidermis
- ▪
Psoriatic arthritis is the major associated systemic manifestation and the most common presentation is asymmetric oligoarthritis of the small joints of the hands and feet; other comorbidities include depression, metabolic syndrome, and cardiovascular disease in patients with moderate to severe disease
- ▪
Topical therapy is used to treat limited disease, whereas phototherapy, methotrexate, cyclosporine and targeted immuno-modulators (“biologic” therapies) that target key immune effector cells and cytokines lead to significant clinical improvement of moderate to severe psoriasis
Introduction
Psoriasis is an immune-mediated polygenic skin disorder . Various environmental triggering factors, e.g. trauma, infections, medications, may elicit disease in predisposed individuals . The characteristic lesion is a sharply demarcated erythematous plaque with micaceous scale, and the plaques may be localized or widespread in distribution. Histologically, hyperkeratosis, parakeratosis, acanthosis of the epidermis, tortuous and dilated vessels, and an inflammatory infiltrate composed predominantly of lymphocytes are observed.
Psoriasis is a systemic disease process in which up to 20–30% of patients have or will develop psoriatic arthritis. In addition, in patients with moderate to severe psoriasis, there is an increased relative risk for metabolic syndrome and atherosclerotic cardiovascular disease. Psoriasis also has a significant impact on patients’ quality of life , and in surveys, patients feel that the current treatments, although often effective, do not provide a satisfactory long-term solution.
History
Hippocrates and his school (460–377 BC) provided meticulous descriptions of many skin disorders. In their classification, dry scaly eruptions were grouped together under the heading “lopoi”. This group probably included psoriasis and leprosy.
Between 129 and 99 BC, the word “psora” (meaning a desquamative condition) was first used by Galen to describe a skin disorder characterized by a scaliness of the eyelids, corners of the eyes, and scrotum. The condition was pruritic and excoriations were present. Although called psoriasis, this affliction was probably a type of eczema.
It was not until the nineteenth century that psoriasis was recognized as an entity distinct from leprosy. Although Robert Willan (1809) was the first to give an accurate description of psoriasis, it would be another 30 years before Hebra (in 1841) definitively separated the clinical features of psoriasis from those of leprosy. In 1879, Heinrich Koebner described the development of psoriatic plaques at sites of skin injury.
Epidemiology and Genetics
In most reviews, the prevalence of psoriasis is said to be 2% of the world’s population. However, in the US and Canada, prevalences as high as 4.6% and 4.7% have been reported, respectively. This contrasts with frequencies in Africans, African-Americans, Norwegian Lapps or Asians of between 0.4% and 0.7%. One population-based study noted that 73% of affected individuals had mild to moderate psoriasis, while 27% suffered from more severe involvement . In one large group of patients with psoriasis ( n = 1728), 79% had nail changes . Psoriatic arthritis has been found to affect 5–30% of patients with cutaneous psoriasis, depending upon the series .
Psoriasis can first appear at any age, from infancy to the eighth decade of life. Two peaks in age of onset have been reported: one at 20–30 years of age and a second peak at 50–60 years. In ~75% of patients, the onset is before the age of 40 years , and in 35–50%, it is before the age of 20 years. Although the age of onset is earlier in women than in men, the natural history is similar – chronic with intermittent remissions. In one epidemiologic study, 39% of the patients stated they had experienced remissions of 1–54 years .
In Europe, the overall prevalence rate for juvenile psoriasis was found to be ~0.7%, with an increase from 0.37–0.55% in those 0 to 9 years of age to 1.01–1.37% in those 10–19 years of age . Plaque psoriasis is the most frequent form of the disease in children, followed by guttate psoriasis.
Genetic Factors
Depending upon the series, a positive family history has been reported by 35% to 90% of patients with psoriasis. Based on a large survey-based study in Germany, if both parents had psoriasis, the risk of their child developing psoriasis was 41%, whereas if only one parent were affected, the risk was 14%; the risk was 6% if just one sibling had psoriasis .
Analysis of concordance rates among monozygotic and dizygotic twins is another method for examining the influence of genetic factors on a disease. One literature review found that of 141 monozygotic twin pairs, 82 were concordant for psoriasis and 59 were discordant; of 155 dizygotic twin pairs, only 31 were concordant and 124 were discordant for psoriasis . Thus, there is a two- to threefold increased risk of psoriasis in monozygotic twins as compared to dizygotic twins, implying that genetic factors are important. The distribution of the lesions, the severity, and the age of onset were similar in the monozygotic twin pairs, whereas these features differed in the dizygotic twin pairs. This observation suggested that genetic factors also play a role in the clinical course of psoriasis.
HLA studies
Histocompatibility antigens (HLA) are surface antigens on human cells, and the corresponding chromosomal region is called the major histocompatibility complex (MHC). It is situated on the short arm (p) of chromosome 6. Psoriasis is associated with HLA-Cw6, with the presence of HLA-Cw6 conferring a relative risk of 13 for developing psoriasis in the Caucasian population and 25 in the Japanese.
HLA-Cw6 is strongly linked to the age of onset of psoriasis. In one series, HLA-Cw6 was expressed in 90% of the patients with early-onset psoriasis, in 50% of those with late-onset psoriasis, and only in 7% of a control population. A specific MHC class II antigen (DRB1*0701/2) also appeared to be associated with early-onset psoriasis, and the psoriasis-associated HLA alleles were often in an extended haplotype: Cw6-B57-DRB1*0701-DQA1*0201-DQB1*0303. Individuals carrying this haplotype were found to have a 26-fold increased risk of developing early-onset psoriasis . As a result, some clinicians have designated patients with early-onset psoriasis, a positive family history of psoriasis, and expression of HLA-Cw6 as having type I psoriasis and those with late-onset disease, no family history, and a lack of expression of HLA-Cw6 as having type II psoriasis . Other HLA alleles may be associated with different psoriasis variants and related conditions. For example, the HLA-B27 allele is a marker for sacroiliitis-associated psoriasis and reactive arthritis (see below).
Genome-wide association studies
Classic genome-wide linkage analysis has identified at least nine psoriasis susceptibility regions (PSORS1–9) in different chromosomal locations . By far the most important genetic region is PSORS1 (on chromosome 6p), which is estimated to account for up to 50% of psoriasis risk. PSORS1 contains genes such as HLA-C (with the HLA-Cw6 risk allele; see above) and corneodesmosin ( CDSN ). Due to high linkage disequilibrium in PSORS1 (i.e. genes within this region are inherited as a block), it has been challenging to determine which gene(s) within PSORS1 contribute to psoriasis pathogenesis. Use of genome-wide association studies (GWAS) has recently provided new insights into the genetic basis of psoriasis. In GWAS, hundreds of thousands of s ingle n ucleotide p olymorphisms (SNPs) across the entire human genome are examined in thousands of patients (see Ch. 54 ). Genes that have been associated with psoriasis through utilization of this and other methods are summarized in Table 8.1 .
| PSORIASIS SUSCEPTIBILITY GENES | |||||
|---|---|---|---|---|---|
| Class | Gene(s) | Pathway | Protein function | OR | Disease overlap |
| Skin specific | LCE3B/3C/3D | Skin barrier formation | KC structural protein | 1.26 | |
| KLF4 | Skin barrier formation IL-17 signaling | Transcription factor | 1.12 | ||
| ETSl | Unknown | Transcription factor | 1.12 | ||
| Innate immunity | IL-28RA | IFN signaling | IL-29 receptor subunit | 1.21 | |
| IFIHl | IFN signaling | Innate antiviral receptor | 1.27 | ||
| RNF114 | IFN signaling | E3 ubiquitin ligase | 1.16 | ||
| ELMOI | IFN signaling | Involved in TLR-mediated IFN-α signaling | 1.11 | ||
| DDX58 | IFN signaling | Innate antiviral receptor | 1.11 | ||
| NOS2 | Inflammation | Induced nitric oxide synthase | 1.22 | ||
| REL | NF-κB signaling | NF-κB subunit | 1.17 | RA | |
| TNlP1 | NF-κB signaling | Inhibitor of TNF-induced NF-κB activation | 1.59 | ||
| TNFAIP3 | NF-κB signaling | Inhibitor of TNF-induced NF-κB activation | 1.23 | ||
| NFKBIA | NF-κB signaling | Inhibitor of NF-κB activation | 1.16 | ||
| FBXL19 | NF-κB signaling | Putative inhibitor of NF-κB activation | 1.16 | ||
| CARDI4 | NF-κB signaling | Activator of NF-κB pathway | 1.11 | ||
| CARMI * | NF-κB signaling | Transcriptional coactivator of NF-κB | 1.17 | ||
| UBE2L3 * | NF-κB signaling | Ubiquitin-conjugating enzyme | 1.13 | Cel, RA, Cro | |
| At the interface between innate and adaptive immunity | TRAF31P3 | IL-23/IL-17 axis NF-κB signaling | Adaptor molecule mediating IL-17-induced NF-κB activation | 1.52 | |
| IL-12B | IL-23/lL-17 axis | Shared subunit of IL-12/IL-23 | 1.58 | ||
| IL-23A | IL-23/IL-17 axis | Unique subunit of IL-23 | 1.39 | ||
| TYK2 | IL-23/lL-17 axis IFN signaling | Tyrosine kinase associated with cytokines receptors | 1.88 | ||
| HLA-C | Antigen presentation | MHC class 1 antigen | 4.32 | ||
| ERAPl | Antigen presentation | Enzyme processing MHC class 1 ligands | 1.2 | AS | |
| Adaptive immunity | IL-23R | IL-23/IL-17 axis | Unique subunit of IL-23 receptor complex | 1.52 | AS, UC, Cro |
| STAT3 * | IL-23/IL-17 axis | Transcription factor | 1.15 | ||
| IRF4 * | IL-17 signaling | Transcription factor | 1.12 | ||
| RUNX3 | T-bet pathway | Transcription factor | 1.13 | AS, Cel | |
| IL-4/IL-13 | IL-4/IL-13 signaling | IL-4 and IL-13 cytokines | 1.18 | ||
| TNFRSF9 * | T-cell differentiation | Adaptor molecule | 1.13 | ||
| TAGAP | T-cell activation | Rho GTPase-activating protein | 1.12 | RA | |
| ZMIZl | TGF-β signaling | Protein inhibitor of activated STAT (PIAS) family of proteins | 1.1 | MS | |
| SOCSl | Type II IFN signaling | Suppressor of cytokine signaling | 1.13 | ||
| Other | PRDX5 | Intracellular redox signaling | Antioxidant enzyme | 1.09 | |
| B3GNT2 | Carbohydrate metabolism | Enzyme | 1.12 | AS | |
| MBD2 * | Unknown | Transcriptional repressor | 1.12 | ||
| ZC3H12C | Unknown | Zinc finger protein with putative RNase function | 1.14 | ||
Several conclusions regarding the genetic factors in psoriasis can be drawn from recent GWAS . First, most of the genes that have been implicated have immune-related functions, underscoring the importance of the innate and adaptive immune systems in the pathogenesis of psoriasis; in contrast, relatively few genes that encode skin-specific proteins have been associated with psoriasis. Second, thus far surprisingly few interactions among the genetic variants have been identified (with the exception of HLA-Cw6 and ERAP-1; see below). Third, associated genes encode proteins with roles in particular immunologic and signaling pathways, especially those involving tumor necrosis factor (TNF), NF-κB, interferons (IFN), and interleukin (IL)-23/Th17 cells (see Table 8.1 ) . Lastly, ERAP1 , which encodes an aminopeptidase involved in MHC class I antigen processing, interacts synergistically with the HLA-Cw6 risk allele, providing another argument for the role of an MHC-restricted antigen and its presentation through HLA-C in the pathogenesis of psoriasis .
Functional genomic studies
Microarray technology has been utilized to obtain a comprehensive picture of the genes expressed in psoriatic skin . More than 1300 genes were found to be differentially expressed when compared to normal human skin. This group of genes included known markers of psoriasis in the skin, but it also contained numerous genes not known to be expressed in the skin. These analyses confirmed (on a genomic scale) the involvement of T cells and dendritic cells (DCs) and also implicated a role for comorbidity-associated genes involved in atherosclerosis signaling and fatty acid metabolism.
Another important gene family differentially expressed in psoriatic epidermis encodes antimicrobial peptides. These peptides are expressed at high levels in psoriatic skin but at low levels in skin affected by atopic dermatitis .
Pathogenesis
Because it primarily affects the interfollicular epidermis, psoriasis was long regarded as an epidermal disease in which the fundamental biochemical or cellular defect resided within the keratinocyte. Accordingly, prior to the early 1980s , a number of biochemical mediators, enzymes and pathways involved in epidermal function were incriminated as being abnormal in psoriasis, including cyclic AMP, eicosanoids, protein kinase C, phospholipase C, polyamines, and transforming growth factor (TGF)-α. Although associated immunologic abnormalities were reported in the late 1970s , a major paradigm shift occurred when T-cell suppressive agents such as cyclosporine were found to result in dramatic improvement of psoriasis . Over the past three decades, psoriasis has been regarded as a T-cell-driven disease . The role of lymphocyte subsets as well as cytokines involved in chemotaxis, homing and activation of inflammatory cells has been extensively investigated, culminating in the development of novel therapeutic approaches . Although some regard psoriasis as an autoimmune disease, to date no true autoantigen has been definitively identified.
Immunopathogenesis
Role of T cells and dendritic cells
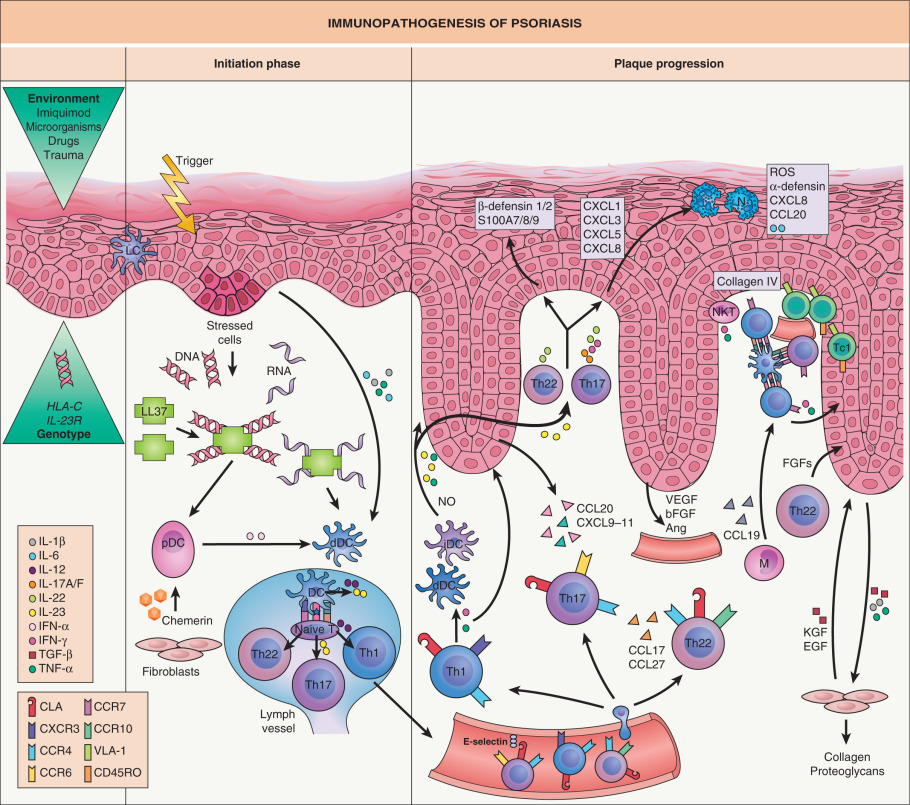
A pathogenic role for antigen-presenting cells and T cells is strongly suggested by the association of psoriasis with particular MHC alleles, e.g. HLA-Cw6 , as well as (in individuals who carry such alleles) variants in ERAP1 , which encodes an aminopeptidase involved in antigen processing. The presence of specific T-cell subsets within the epidermis and dermis of lesional skin is well documented ( Fig. 8.1 ). Also, a number of compounds that affect T-cell function (e.g. by targeting the IL-2 receptor, CD2, CD11a and CD4) were found to result in clinical improvement of psoriasis . Another argument supporting involvement of the adaptive immune system is the disappearance or development of psoriasis following hematopoietic stem cell transplantation . In addition, analysis of lesional T cells has shown oligoclonality, indicating potential antigen-specific expansion of T-cell subpopulations, possibly triggered by exogenous microbial or viral antigens or cross-reacting autoantigens, e.g. keratins .
Animal models for psoriasis have also demonstrated the importance of T cells. In xenograft models in which uninvolved psoriatic skin was transplanted onto immunodeficient mice, donor immune cells (in particular resident T cells) were capable of expanding and inducing the complete lesional phenotype . Induction of psoriatic lesions in these models was also shown to be dependent on TNF-α and on IFN-α derived from plasmacytoid DCs (pDCs) . These experiments demonstrated that T cells can trigger psoriasis in a suitable patient-derived environment.
In humans, several cell types have been implicated in the initiation and maintenance of psoriatic lesions (see Fig. 8.1 ). Most of the epidermal T cells are CD8 + , whereas the dermal infiltrate is a mixture of CD4 + and CD8 + cells. The majority of the cells in both locations are memory T cells that express cutaneous lymphocyte antigen (CLA; the skin homing receptor) and chemokine receptors such as CCR4. Expression of α 1 β 1 integrin (VLA-1) on psoriatic T cells, which allows their interaction with basement membrane collagen IV, is key for the entrance of these cells into psoriatic epidermis and establishment of the psoriatic epithelial phenotype . Unconventional T cells also contribute to the pathogenesis of psoriasis via secretion of proinflammatory cytokines and chemokines. These include natural killer (NK) T cells, gamma delta (γδ) T cells, and innate lymphoid cells (ILCs) .
DCs are present in both uninvolved and lesional psoriatic skin, and because of their potent immunostimulatory capacity, they are likely to be involved in its pathogenesis. There is an increased number of dermal DCs in psoriatic skin, and they have an enhanced ability to activate T cells when compared to DCs from normal skin . DC phenotype and function are quite plastic, with the ability to differentiate into potent proinflammatory DCs that produce inducible nitric oxide synthase (iNOS) and TNF-α (referred to as TIP [ T NF/ i NOS- p roducing] DCs) . The role of DCs in psoriasis has been validated by the presence of a prominent genomic DC signature and the decrease of DCs during effective targeted therapy .
Based upon studies in humans and a xenograft model, another type of DC, the pDC, was shown to initiate psoriasis via the production of IFN-α . Complexes of self DNA or RNA (from keratinocytes) plus antimicrobial peptide LL37 trigger IFN-α release by pDCs via a Toll-like receptor 9 (TLR9)-dependent mechanism (see Fig. 8.1 ). This leads to a breaking of tolerance to self nucleic acids and potentially explains the start of the inflammatory cascade in psoriasis .
The presence of neutrophils in the epidermis, either in spongiform pustules of Kogoj or in microabscesses of Munro, is a typical histopathologic feature of psoriasis, especially acute or pustular forms. Neutrophils are typically prominent in active lesions and in the marginal zone of expanding plaques, but, in contrast to T cells, they are not a consistent feature of lesional skin. Although activated neutrophils could contribute to its pathogenesis, they are not considered to be the primary cause of psoriasis.
Prominent angiogenesis is observed within plaques of psoriasis. There is increased expression of vascular endothelial growth factor (VEGF) , and anti-VEGF therapy leads to improvement in mouse models of psoriatic inflammation .
Cytokines and chemokines
Psoriasis is considered to be a disease with prominent involvement of T-helper-cell subsets and their secreted cytokines . Increased amounts of Th1 cytokines (IFN-γ and IL-2) are observed, whereas levels of the anti-inflammatory cytokine IL-10 are reduced. Based on animal studies and measurements in lesional skin, IL-12, IL-23 and IL-15 are likely to contribute to the disease. The striking response of psoriasis to ustekinumab, a human monoclonal antibody against the p40 subunit of IL-12 and IL-23, provides additional evidence for the role of cytokines. It is thought that IL-23 (produced by DCs) stimulates Th17 cells to release IL-17 and IL-22; the concerted action of these cytokines leads to proliferation of keratinocytes and dermal inflammation (see Fig. 8.1 ) . Of note, circulating levels of IL-22 correlate with disease severity. It has also been proposed that there is a distinct subset of IL-22-producing T helper cells (Th22 cells) that contribute to the pathogenesis of psoriasis . The IL-17-producing T cells in psoriatic epidermis might have a cytotoxic phenotype, qualifying them as Tc17 cells .
IFN-γ is released by activated T cells and NK T cells within the epidermis, and it activates members of the STAT transcription factor family, which drive the expression of a large number of immune-related genes that have roles in psoriasis pathogenesis. The IFN-γ-activated pathway is a key feature of psoriasis and explains several phenotypic alterations such as vasodilation (by the induction of iNOS) and accumulation of T cells (via the expression of various chemokines).
The innate immune cytokines IL-1, IL-6 and TNF-α are upregulated in psoriatic skin. TNF-α is a particularly relevant cytokine and its importance is underscored by the therapeutic efficacy of TNF-α inhibitors (see Treatment ).
Chemokines are important mediators in the trafficking of leukocytes, and the increase in several chemokines and their cognate receptors within psoriatic lesions has been extensively documented. CXCL8 is thought to mediate the often-prominent infiltration by neutrophils. CCL17, CCL20, CCL27, and CXCL9–11 are implicated in attracting T cells to the psoriatic plaque. A pDC-attracting chemokine, chemerin, is increased in psoriatic skin and might contribute to the early recruitment of pDCs into psoriatic lesions .
Innate immunity and role of keratinocytes
In the skin, various cell types are involved in innate (non-adaptive) immune response pathways. These include DCs (myeloid DCs and pDCs), NK T cells, γδT cells, ILCs, and neutrophils (see above), as well as epidermal keratinocytes. For example, keratinocytes constitutively express antimicrobial proteins such as β-defensin-1 (hBD1) and secretory leukocyte protease inhibitor (SLPI), which have direct antimicrobial activity against a broad spectrum of pathogens. In addition, keratinocytes can be stimulated to express a wide variety of other inducible antimicrobials such as hBD2, the cathelicidin LL37, and SKALP/elafin . In addition to these effector molecules, keratinocytes express TLRs and secrete signaling molecules such as IL-1, IL-6, IL-8, and TNF-α. Interestingly, the antimicrobial effector protein hBD2 was also shown to have chemotactic activity via CCR6 and to bind to TLR4. Since most of these proteins are highly expressed in lesional psoriatic skin, it is likely that they are involved in the initiation or control of the inflammatory process; however, their precise roles remain to be determined.
Any model of the pathogenesis of psoriasis also has to account for the dramatically increased proliferation rate of keratinocytes. The cytokines and chemokines found in lesional skin are generally not mitogenic for keratinocytes. For example, IFN-γ, a prominent Th1 cytokine, is itself antiproliferative, but it was found to be a crucial factor in supernatants of lesion-derived T-cell clones that could drive keratinocyte stem cell proliferation .
Keratinocytes within psoriatic plaques express STAT3, suggesting that this transcription factor might be of pathogenetic importance. In a transgenic animal model, epidermal expression of STAT3 (in cooperation with T cells) was found to induce psoriasis-like lesions in mice . STAT3 induced the upregulation of a number of genes relevant for psoriasis, such as those encoding ICAM-1 and TGF-α; the latter has been shown to stimulate proliferation of keratinocytes in psoriasis via an autocrine loop. As STAT3 is activated by a variety of cytokines including IL-22 as well as IL-6, IL-20 and IFN-γ, this could represent a link between keratinocyte activation and immune cells in the development of the psoriatic lesion.
Triggering Factors
Triggering factors, both external (directly interacting with the skin) and systemic, can elicit psoriasis in genetically predisposed individuals.
External triggering factors
The Koebner or isomorphic phenomenon, i.e. the elicitation of psoriatic lesions by injury to the skin, is observed in ~25% of patients with psoriasis. A particular patient may be “Koebner-negative” at one point in time and later become “Koebner-positive”. The Koebner phenomenon suggests that psoriasis is a generalized skin disease that can be triggered locally. Psoriatic lesions can also be induced by other forms of cutaneous injury, e.g. sunburn, morbilliform drug eruption, viral exanthem. The lag time between the trauma and the appearance of skin lesions is usually 2–6 weeks.
Systemic triggering factors
Infections
Infections, particularly bacterial infections, may induce or aggravate psoriasis. Provoking infections have been observed in up to 45% of psoriatic patients. Streptococcal infections, especially pharyngitis, are the most common offenders. In the palatine tonsils of psoriasis patients, immune responses have been shown to be dysregulated, with elevated expression of CLA and the IL-23 receptor . Streptococci can also be isolated from other sites of infection, e.g. dental abscesses, perianal cellulitis, impetigo.
HIV
HIV infection has also been shown to aggravate psoriasis (see Ch. 78 ).
Endocrine factors
Hypocalcemia has been reported to be a triggering factor for generalized pustular psoriasis. Although active vitamin D 3 analogues improve psoriasis, abnormal vitamin D 3 levels have not been shown to induce psoriasis. Pregnancy may alter disease activity, e.g. 50% of the patients in one series reported improvement. However, pregnant women may develop pustular psoriasis, also referred to as impetigo herpetiformis (see below), sometimes in association with hypocalcemia.
Psychogenic stress
Psychogenic stress is a well-established systemic triggering factor in psoriasis, with a heightened cortisol response to stress having been demonstrated in affected patients . Stress is associated with initial presentations of the disease as well as flares of pre-existing psoriasis. In a prospective study, cognitive and behavioral patterns of worrying and scratching were both independently related to an increase in disease severity and pruritus 4 weeks later .
Drugs
Several drugs have been incriminated as inducers of psoriasis, in particular lithium, IFNs, β-blockers, and antimalarials. Rapid taper of systemic corticosteroids can induce pustular psoriasis as well as flares of plaque psoriasis.
Alcohol consumption, smoking and obesity
Obesity, increased alcohol consumption, and smoking have all been associated with psoriasis. In one analysis, smoking appeared to have a role in the onset of psoriasis, while obesity appeared to be a consequence of psoriasis. However, other studies have suggested that weight gain often precedes the development of psoriasis. Some studies have found that the prevalence of psoriasis in a population of individuals who stop smoking or who lose weight eventually reverts to background levels.
Clinical Features
Chronic plaque psoriasis, the most common variant of psoriasis vulgaris, is characterized by sharply demarcated and erythematous papulosquamous lesions. Less often, nearly all of the body surface is involved ( erythrodermic psoriasis ) or numerous, small, widely disseminated papules and plaques are seen ( guttate psoriasis ). Occasionally, there are obvious macroscopic pustules, as in generalized pustular psoriasis or pustulosis of the palms and soles.
From a clinical perspective, psoriasis can present with a spectrum of cutaneous manifestations. At any one point in time, different variants may coexist in a particular individual, but the skin lesions all share the same important hallmarks: erythema, thickening, and scale. As noted in the section on Epidemiology and Genetics , there is also significant interindividual variability. For example, in patients with chronic plaque psoriasis, those with type I disease (HLA-Cw6 + ) have an earlier onset, more widespread disease and frequent recurrences, compared to those with type II psoriasis.
Although the size of a lesion may vary from a pinpoint papule to over 20 cm in diameter, the outline of the lesion is usually circular, oval or polycyclic (the latter indicating that the lesion is derived from several smaller units). The configuration of psoriatic lesions due to the Koebner phenomenon reflects the etiology of the trauma. In addition to their highly characteristic sharp demarcation, psoriatic lesions are sometimes surrounded by a pale blanching ring, which is referred to as Woronoff’s ring .
The classic findings of erythema, thickening and scale are reflections of the histologic findings of elongated dilated capillaries that are close to the skin surface, epidermal acanthosis plus cellular infiltrates, and abnormal keratinization, respectively. If the superficial silvery white (micaceous) scales are removed, then a wet surface is seen with characteristic pinpoint bleeding. This finding, called Auspitz sign, is the clinical reflection of elongated vessels in the dermal papillae together with thinning of the suprapapillary epidermis.
During exacerbations, psoriatic lesions often itch. Pinpoint papules surrounding existing psoriatic plaques indicate that the patient is in an unstable phase of the disease. In addition, expanding psoriatic lesions are characterized by an active edge with a more intense erythema. Inflamed lesions may be slightly tender. The involution of a lesion usually starts in its center, resulting in annular psoriatic lesions ( Fig. 8.2 ).

Chronic Plaque Psoriasis
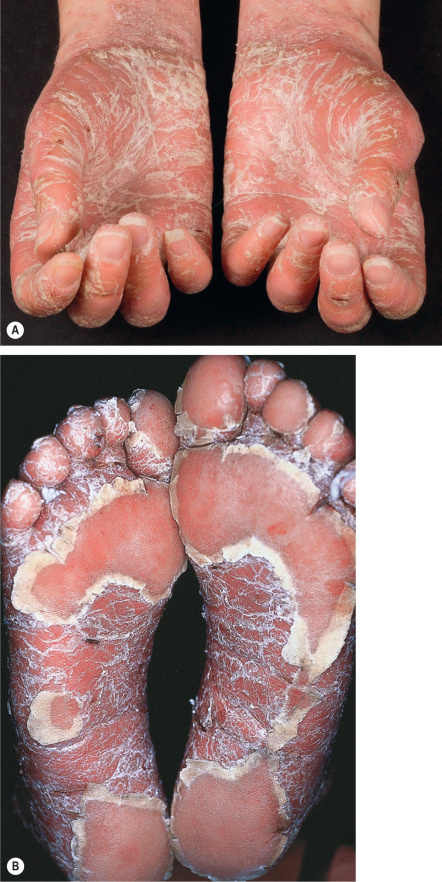
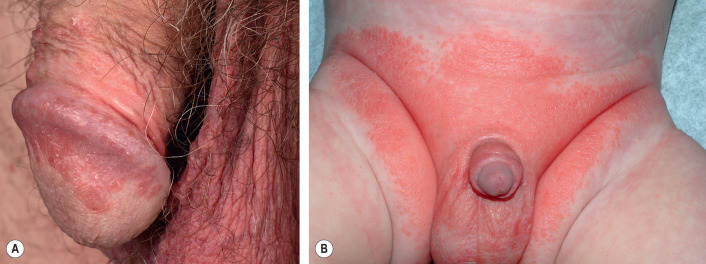
In chronic plaque psoriasis, there is a relatively symmetric distribution of sharply defined, erythematous, scaly plaques ( Figs 8.3 & 8.4 ). The degree of body surface area involvement can vary, from limited to extensive. The scalp, elbows, knees and lumbosacral area are sites of predilection, as are the hands and feet ( Fig. 8.5 ). The genitalia are involved in up to 45% of patients ( Fig. 8.6 ; see Ch. 73 ). Plaques may persist for months to years at the same locations. Although the course of this disease is chronic, periods of complete remission do occur and remissions of 5 years have been reported in ~15% of patients.


Because the percentage of body surface area involved does not reflect the severity of the individual lesions with respect to erythema, induration and scaling, the Psoriasis Area and Severity Index (PASI) was formulated ( Table 8.2 ). This is a single calculated score that is based on the body surface area involved (in each of four anatomic areas – head, upper extremities, trunk and lower extremities) and clinical grading of lesional erythema, induration and scaling. The PASI is a cumbersome calculation and is more commonly utilized for clinical trials than for the routine management of patients with psoriasis.
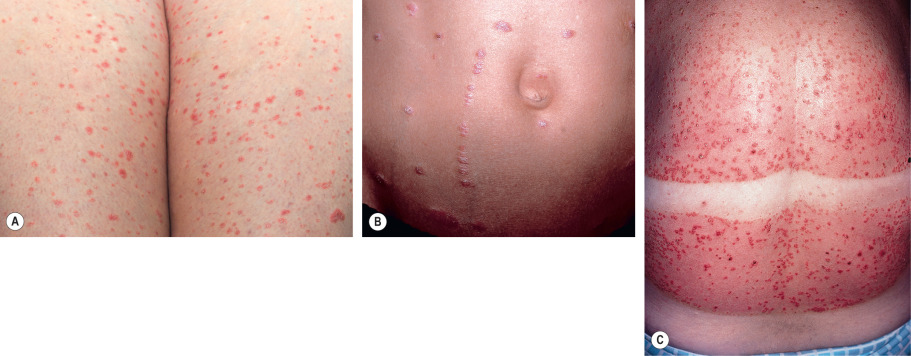
Guttate Psoriasis
Guttate psoriasis is more commonly seen in children and adolescents and is frequently preceded by an upper respiratory tract infection ( Fig. 8.7 ). In over half of the patients, an elevated antistreptolysin O, anti-DNase B or streptozyme titer is found, indicating a recent streptococcal infection (see previous section).
Erythrodermic Psoriasis
This variant of psoriasis is characterized by generalized erythema and scaling, and its onset can be gradual or acute. Although there are many causes of erythroderma (see Ch. 10 ), clues to the diagnosis of psoriatic erythroderma include previous plaques in classic locations, characteristic nail changes, and central facial sparing.
Pustular Variants
Generalized pustular psoriasis
In generalized pustular psoriasis, infiltration of neutrophils dominates the histologic picture, explaining the bright erythema and sterile pustules ( Fig. 8.8 ). It is an unusual manifestation of psoriasis, and triggering factors include pregnancy, rapid tapering of corticosteroids (or other systemic therapies), hypocalcemia, infections, and, in the case of the localized pattern, topical irritants. Generalized pustular psoriasis during pregnancy is also referred to as impetigo herpetiformis . Of note, the clinical presentation of several inherited autoinflammatory disorders (e.g. DIRA, DITRA, CARD14-mediated pustular psoriasis, ADAM17 deletion) resembles generalized pustular psoriasis (see Table 45.7 ) .

Four distinct patterns of generalized pustular psoriasis can be seen:
- •
von Zumbusch pattern . This is a generalized eruption starting abruptly with erythema and pustulation (see Fig. 8.8 ). The skin is painful during this phase, and the patient has a fever and feels ill. After several days, the pustules usually resolve and extensive scaling is observed. Sometimes, chronic plaques of psoriasis, if present, can resolve. In the original case report by von Zumbusch (1910), nine episodes of pustulation occurred over a period of 10 years.
- •
Annular pattern . The eruption is characterized by annular lesions, consisting of erythema and scaling with pustulation at the advancing edge ( Fig. 8.9 ). The lesions enlarge by centrifugal expansion over a period of hours to days, while healing occurs centrally.
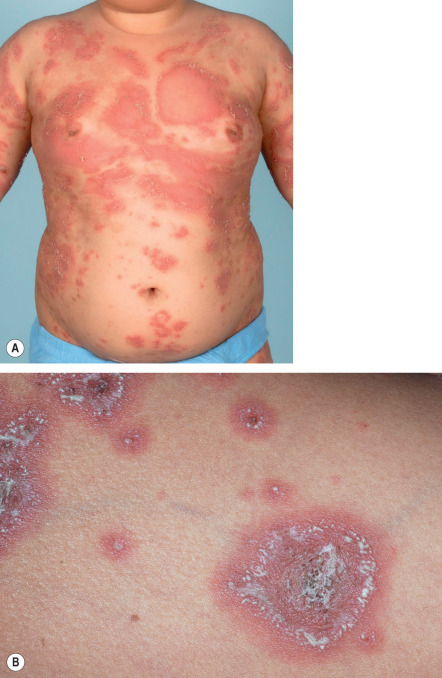
Fig. 8.9
Annular pustular psoriasis.
A,B Multiple annular inflammatory plaques whose active borders are studded with pustules followed by desquamation. As these lesions enlarge, there is central clearing. The intensity of erythema can vary and the color is influenced by the skin phototype.
A, Courtesy, Marieke M B Seyger, MD, PhD; B, Courtesy, Julie V Schaffer, MD.
- •
Exanthematic type . This is an acute eruption of small pustules, abruptly appearing and disappearing over a few days. It usually follows an infection or may occur as a result of administration of specific medications, e.g. lithium. Systemic symptoms usually do not occur. There is overlap between this form of pustular psoriasis and pustular drug eruptions, also referred to as acute generalized exanthematous pustulosis (AGEP; see Ch. 21 ).
- •
“Localized” pattern . Sometimes pustules appear within or at the edge of existing psoriatic plaques. This can be seen during the unstable phase of chronic plaque psoriasis and following the application of irritants, e.g. tars, anthralin.
Pustulosis of the palms and soles
Pustulosis of the palms and soles is characterized by “sterile” pustules of the palmoplantar surfaces admixed with yellow–brown macules ( Fig. 8.10 ); scaly erythematous plaques may also be seen. A minority of patients have chronic plaque psoriasis elsewhere. In contrast to the natural history of generalized pustular psoriasis, the pustules remain localized to the palmoplantar surfaces and the course of this disease is chronic. Focal infections and stress have been reported as triggering factors and smoking may aggravate the condition. Pustulosis of the palms and soles is one of the entities most commonly associated with sterile inflammatory bone lesions within the context of SAPHO syndrome, which consists of s ynovitis, a cne, p ustulosis, h yperostosis and o steitis. Several neutrophilic dermatoses are associated with SAPHO (see Table 26.18 ).

Acrodermatitis continua of Hallopeau
This is a rare manifestation of psoriasis. Clinically, pustules are seen on the distal portions of the fingers ( Fig. 8.11 ) and sometimes the toes. Pustulation is often followed by scaling and crust formation. Pustules may also form in the nail bed (beneath the nail plate), and there may be shedding of nail plates. Transition into other forms of psoriasis can occur and acrodermatitis continua may be accompanied by annulus migrans of the tongue (see below).

Special Locations
Scalp psoriasis
The scalp is one of the most common sites for psoriasis. Unless there is complete confluence, the individual lesions are discrete, in contrast to the less well-defined areas of involvement in seborrheic dermatitis. At times, however, it is not possible to distinguish seborrheic dermatitis from psoriasis, and the two disorders may coexist. The lesions of psoriasis often advance onto the periphery of the face, the retroauricular areas and the posterior upper neck ( Fig. 8.12 ). The scales sometimes have an asbestos-like appearance and can adhere to hair shafts in clumps (pityriasis amiantacea). Although pityriasis amiantacea can also be seen in patients with seborrheic dermatitis, secondarily infected atopic dermatitis and tinea capitis, psoriasis is the most common cause. Alopecia occasionally develops within involved areas, including in the setting of TNF inhibitor-induced psoriasis (see Ch. 69 ). In addition, patients with dermatomyositis involving the scalp may have lesions that resemble psoriasis.

Flexural psoriasis
Flexural lesions are characterized by shiny, pink to red, sharply demarcated thin plaques ( Fig. 8.13 ). There is much less scale than in untreated chronic plaque psoriasis. Often a central fissure is seen. The most common sites of involvement are the retroauricular fold, intergluteal cleft, inguinal crease, axilla, and inframammary region. When flexural areas are the only sites of involvement, the term “inverse” psoriasis is sometimes used. Localized dermatophyte, candidal or bacterial infections can be a trigger for flexural psoriasis.

Oral mucosa
Migratory annular erythematous lesions with hydrated white scale (annulus migrans) have been observed in patients with acrodermatitis continua of Hallopeau and generalized pustular psoriasis. The most common location is the tongue, and the clinical (and histologic) appearance is similar to geographic tongue. Occasionally, lesions are observed on the buccal mucosa.
Nail psoriasis
Nail involvement has been reported in 10–80% of psoriatic patients, depending upon the series. The fingernails are more often affected than the toenails ( Fig. 8.14 ). In a survey from the Netherlands, 79% of patients reported involvement of their nails, with 52% experiencing associated pain and 14% major restrictions in daily life due to the nail changes. Patients with nail involvement appear to have an increased incidence of psoriatic arthritis.

Psoriasis affects the nail matrix, nail bed, and hyponychium. Small parakeratotic foci in the proximal portion of the nail matrix lead to pits in the nails (see Ch. 71 ). Leukonychia and loss of transparency (less common findings) are due to involvement of the midportion of the matrix. If the entire nail matrix is involved, a whitish, crumbly, poorly adherent “nail” is seen. Psoriatic changes of the nail bed result in the “oil drop” or “salmon patch” phenomenon, which reflects exocytosis of leukocytes beneath the nail plate. Splinter hemorrhages are the result of increased capillary fragility, and subungual hyperkeratosis and distal onycholysis are due to parakeratosis of the distal nail bed. Vigorous removal of distal subungual debris may be an exacerbating factor.
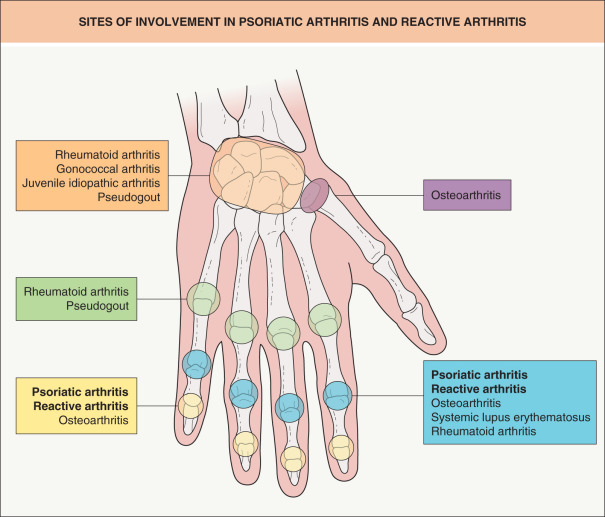
Psoriatic Arthritis
Psoriatic arthritis occurs in 5–30% of patients with cutaneous psoriasis , with some clinical investigators suggesting that classic studies of psoriatic arthritis may have underestimated its prevalence. In a minority of patients (10–15%), the symptoms of psoriatic arthritis appear before involvement of the skin. Currently, there are no specific serologic tests for establishing the diagnosis of psoriatic arthritis, but an important hallmark is erosive change radiographically, which may occur years after the presenting peri-articular inflammation. Psoriatic arthritis is more prevalent among patients with relatively severe psoriasis. Risk factors for a more severe course of the arthritis include: initial presentation at an early age, female gender, polyarticular involvement, genetic predisposition, and radiographic signs of the disease early on. The five major forms of psoriatic arthritis are outlined in Table 8.3 .
| FIVE MAJOR TYPES OF PSORIATIC ARTHRITIS | |
|---|---|
| Type | Clinical findings |
| Mono- and asymmetric oligoarthritis (most common type) |
|
| Arthritis of the distal interphalangeal joints |
|
| Rheumatoid arthritis-like presentation (difficult to distinguish from RA clinically * ) |
|
| Arthritis mutilans ** (least common type) |
|
| Spondylitis and sacroiliitis (also have peripheral joint involvement) |
|
* Whether some seropositive patients have an overlap of the two disorders is possible.

In one study involving 1511 patients with chronic plaque psoriasis, ~20% of the affected individuals had psoriatic arthritis . DIP involvement was observed in ~40% of the patients with arthritis, and 5% suffered from arthritis mutilans . Patients with psoriatic arthritis can have involvement of juxta-articular tendons (tendonitis) and the sites where they insert into bone (enthesitis) as well as swelling of the fingers (dactylitis). Enthesitis and dactylitis have been reported in ~20% and 15–30%, respectively, of patients with “probable” or definite psoriatic arthritis. In patients with psoriasis, nail involvement is a strong predictor of concomitant psoriatic arthritis .
Early diagnosis of psoriatic arthritis is important, as disease progression often results in loss of function and irreversible joint destruction.
Disorders Related to Psoriasis
A few disorders share important clinical and histologic features with psoriasis, but are distinct disease entities based upon genetic, epidemiologic or clinical features.
Inflammatory linear verrucous epidermal nevus (ILVEN)
ILVEN is characterized by linear psoriasiform lesions (i.e. scaling and erythematous plaques) that follow the lines of Blaschko (see Ch. 62 ). Based upon its chronicity and resistance to therapy, ILVEN is thought to be an entity separate from linear psoriasis.
Reactive arthritis (formerly Reiter disease)
This syndrome features urethritis, arthritis, ocular findings and oral ulcers, in addition to psoriasiform skin lesions. The disorder is uncommon in children and occurs more frequently in men than in women. The urethritis may be mild or severe and accompanied by complications such as cystitis, cervicitis, and salpingitis. Chlamydia trachomatis is a major cause of urethritis and may trigger the entire syndrome, as may other infections such as shigellosis. Conjunctivitis is a common eye finding in affected patients, although iritis, uveitis with glaucoma, and keratitis may also occur. Polyarthritis and sacroiliitis are the most frequent joint manifestations. Cutaneous lesions occur in approximately 5% of reactive arthritis patients, with a predilection for the soles, extensor surfaces of the legs, penis, dorsal aspects of the hands, fingers, nails, and scalp ( Fig. 8.17 ). The lesions on the plantar surface usually have thick yellow scale and are often pustular (keratoderma blennorrhagicum). Psoriatic plaques on the penis are referred to as balanitis circinata.

Reactive arthritis has a strong association with HLA-B27. Although the course is often self-limited, lasting weeks to months, some patients have disease that is chronic and disabling. Of note, HIV-infected patients can also develop this disorder and it may be severe.
Sneddon–Wilkinson disease (subcorneal pustular dermatosis)
This disorder is characterized by annular or polycyclic lesions, usually commencing in the flexures ( Fig. 8.18A ). Very superficial (subcorneal) sterile pustules are the hallmark of Sneddon–Wilkinson disease, hence its second name ( Fig. 8.18B ). There may be a gravity-induced demarcation in some vesiculopustules, with clear fluid superiorly and pus inferiorly. This disease has a cyclic course, i.e. as the pustules resolve they are replaced by superficial scaling and then new pustules form again. Some patients with Sneddon–Wilkinson disease have an associated IgA paraproteinemia. Its response to dapsone, combined with subcorneal pustules (in the absence of spongiform pustules), provide support for this condition being a disease entity distinct from pustular psoriasis, although some authors have questioned the existence of Sneddon–Wilkinson disease as a distinct entity. Of note, immunofluorescence studies are required to distinguish the subcorneal pustular dermatosis type of IgA pemphigus from Sneddon–Wilkinson disease.

Associations Between Psoriasis and Other Diseases
Associations with skin diseases
There is a pronounced under-representation of allergic skin diseases in psoriatic patients as compared to age-matched controls without psoriasis. The frequencies of atopic dermatitis, asthma, urticaria and allergic contact dermatitis have been found to be lower in psoriatic patients. For example, in one study atopic dermatitis was seen ~50 times less often in psoriatic compared with non-psoriatic patients . An obvious explanation is the immunologic difference between these two conditions, with a predominantly Th1 response in psoriasis and a predominantly Th2 response in atopic dermatitis. However, in patients with psoriasis in atypical locations and/or treatment-resistant lesions, the possibility of allergic contact dermatitis as a triggering factor needs to be considered.
A bi-directional relationship exists between lichen simplex chronicus (LSC) and psoriasis. If a psoriatic lesion is pruritic, superimposed LSC may develop and the surface becomes shiny with increased skin markings. Because the LSC itself is pruritic, the resultant rubbing may worsen the psoriasis (Koebner phenomenon). The patient then enters a vicious cycle. Therapeutic regimens must address both disorders.
Seborrheic dermatitis is characterized by pink to red patches with yellowish, sometimes greasy, scales (see Ch. 13 ). The sites of predilection are the scalp, central face, ears, presternal area, and intertriginous zones. As the clinical features of psoriasis and seborrheic dermatitis can be seen in the same patient, some authors use the term “sebopsoriasis”, especially when diagnostic lesions of psoriasis are not present elsewhere.
Infections
In contrast to atopic dermatitis, psoriatic lesions are seldomly impetiginized, i.e. secondarily infected by bacteria. One explanation for this resistance to secondary bacterial infections is increased production of skin-derived antimicrobial peptides, e.g. defensins, SKALP/elafin (see Pathogenesis ).
The prevalence of onychomycosis, due to Candida species or dermatophytes, is increased in psoriatic patients (average, ~18%), compared to control groups . In flexural psoriasis, concomitant Candida infections are frequently observed and have been incriminated as a local triggering factor.
Cancer
Patients with psoriasis may have a slightly higher incidence rate of all malignancies compared to the general population . With the exception of a significantly higher rate of nonmelanoma skin cancer in those who had received phototherapy (type not specified), differences in rates were minimal when various systemic therapies were compared . It has been shown that psoriatic patients who have had >200 PUVA treatments are at increased risk for the development of skin cancers, especially squamous cell carcinomas (SCCs). Of note, the use of cyclosporine in patients previously treated with PUVA significantly increases the number and rate of appearance of SCCs. Lastly, there is controversy as to whether PUVA-treated patients have an increased risk of cutaneous melanoma.
Association with internal diseases (including comorbidities)
Cardiovascular diseases , e.g. myocardial infarctions, peripheral arterial disease, cerebrovascular accidents, are more common in patients with severe psoriasis. The latter is associated with a threefold increased risk for myocardial infarction and a 3.5–4.4-year reduction in life expectancy. This is largely due to an increased risk for having metabolic syndrome (see Table 53.5 ) . In patients with psoriatic arthritis, serum levels of C-reactive protein (CRP) have been reported to be elevated (as compared to healthy controls), and elevated CRP levels represent a risk factor for the development of cardiovascular disease. It has also been shown that TNF-α and IL-6 can target adipocytes and induce dyslipidemia. It has not yet been shown convincingly that treatment with methotrexate and/or TNF-α inhibitors reduces the risk of atherosclerotic cardiovascular disease. Patients with psoriasis may also be at increased risk for the development of venous thromboembolism.
Non-alcoholic steatohepatitis , characterized by fatty infiltration, periportal inflammation and focal necrosis, is more commonly observed in patients with psoriasis. In a study of 142 adults with psoriasis, non-alcoholic fatty liver disease was detected in 59%, and it correlated with the presence of obesity, hyperlipidemia, the metabolic syndrome, an AST : ALT ratio >1, and psoriatic arthritis . Chronic administration of methotrexate is associated with a significant risk for hepatic damage in patients with psoriasis, whereas similar methotrexate dosages in patients with rheumatoid arthritis do not pose such hepatotoxic potential. Although the reason for this difference is not known, several possible explanations have been put forward, including a genetic predisposition, increased alcohol consumption by psoriasis patients, and a higher incidence of non-alcoholic fatty liver disease.
Crohn disease, ulcerative colitis, and psoriasis share an association with sacroiliitis and HLA-B27 positivity. In genome-wide association studies of Crohn disease and psoriasis, shared susceptibility loci were identified . Additional disorders that share susceptibility genes with psoriasis are listed in Table 8.1 . Lastly, in a population-based cohort study, an association between psoriasis and kidney disease was suggested .
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


