div class=”ChapterContextInformation”>
70. Penile Prostheses in Transgender Males
Keywords
Penile prostheticPhalloplastyTransgenderComplications70.1 Introduction
An ideal phalloplasty would be completed in one surgical stage with good aesthetic appearance, erogenous and tactile sensitivity, patency of the neourethra, sufficient rigidity to allow sexual intercourse and a volume sufficient to place a protected prosthesis [1]. Pedicled flaps transfer tissue from the thigh, groin or lower abdomen to reconstruct the neophallus, while free flaps transfer tissue from a remote location [2–5]. After phalloplasty, the neophallus is empty and flaccid. Erectile implants are needed to obtain rigidity and complete the reconstruction [6, 7].
The neophallus has decreased phallic sensation and a lack of corpora cavernosa, making penile prosthesis placement inherently difficult and prone to complication. Implant procedures are the last stage of reconstruction, typically performed 9 months to 1 year after phalloplasty upon return of protective sensation [8]. At this time, vascular integration of the phallus should be optimized and urethral complications will have resolved or been corrected, thereby decreasing the risk of vascular complications during implantation, or unexpected urethral stricture that may be difficult to treat with a prosthesis in place [9].
When the phallus is constructed by use of a fibula flap or a radial forearm flap , rigidity can be achieved via transplantation of part of the fibula or radius, respectfully. However, donor site complications are substantially increased [10, 11] and these procedures are becoming increasingly uncommon. Furthermore, a permanently rigid phallus can be difficult to conceal and lead to embarrassment, or bone may resorb over time to varying degrees. The latissimus dorsi myocutaneous free flap may permit muscular contraction which might create penile rigidity, but also shortens the penis [12]. With the majority of the phalloplasty techniques, an inflatable penile prosthesis is used if erectile function is desired.
In the native male anatomy, the corpora cavernosa are anchored to the pubic bone and pubic rami and the prosthesis is inserted into the corpora. Phalloplasty lacks corporal tissue within which to anchor the implant proximally, therefore resulting in complications such as migration and malposition. Furthermore, a paucity of soft tissue distally can lead to erosion. Moreover, the current array of penile prostheses is designed for native male anatomy and must be retrofitted to the transman. This chapter will discuss considerations of penile prostheses after phalloplasty.
70.2 Types of Penile Implants
Penile prostheses or implants can be divided into three types: noninflatable, a two-piece inflatable implant, and a three-piece inflatable implant.
Noninflatable Penis Implants
This includes semirigid malleable and nonmalleable rods. One or two cylinders are inserted into the penis. Often the implants are covered first in Gore-Tex vascular graft material (W.L. Gore & Associates, Flagstaff, AZ) to mimic a neo-tunica albuginea and potentially decrease erosion and migration. The rods have an outer coating of silicone and an inner stainless-steel core or interlocking plastic joints. These devices are entirely contained in the neophallus. Noninflatable implants are always rigid but can be positioned up or down and can be bent into different positions for erect and flaccid states. A wide range of sizes are available and these are easy to manipulate; however, these are the least commonly used implants. Semirigid devices may provide constant pressure on phallic structures and increase the risk of erosion, and should arguably be used only in the sensate neophallus. In our high-volume practice, we allow patients to choose either semi-rigid and inflatable penile prostheses; differences in complication rates between the two have not been appreciated.
Two-Piece Inflatable Penile Implants
Hydraulically activated cylinders are surgically inserted into the shaft of the penis. The erection is provided by a hydraulic pump, which transfers saline from a reservoir within the neoscrotum to the cylinders in the penis. The release valve on the pump drains the saline from the cylinders into the reservoir for deflation. This implant is entirely contained in the neophallus and more easily concealed under clothing compared to the noninflatable implant. The two-piece inflatable prosthesis requires manual dexterity for inflation. The penis is not as rigid as a three-piece inflatable penile implant. We tend not to use these devices, in favor of three-piece implants.
Three-Piece Inflatable Penile Implants
Three-piece inflatable implants are the most commonly used penile implants. A single cylinder or pair of cylinders are implanted into the penis and a pump is implanted in the neoscrotum, taking the place of one of the testicle implants. The saline reservoir is implanted in the lower abdomen under the rectus muscle. By squeezing the scrotal pump, saline is transferred from the reservoir into the cylinders to create a more erect penis. Deflating the cylinders transfers the saline back into the reservoir to create a flaccid phallus. Compared to the two-piece inflatable implants, the reservoir is larger and function is generally better. This prosthesis is concealed within the neophallus . This implant is the most expensive and has a higher rate of mechanical failure compared to other implants, but is easy to use and most closely resembles the process of a normal erection.
70.3 Technique of Inflatable Penile Prosthesis Insertion
70.3.1 Background/Preoperative Preparation
The basics of this operation are very similar to that in a cismale, but some details are notably different and will be highlighted. The patient must be free of infection preoperatively (including a negative urine culture) and blood sugar must be under good control with A1c less than 7.5. Blood sugar should be in good control in the perioperative period. After clipping of excess hair in the surgical area, preparation includes gentle irrigation of the urethra with betadine solution, then standard extensive skin preparation (we perform a 15 minute prep using both betadine scrub, then chlorhexidine soap wash, followed by Duraprep (3 M, St. Paul, MN) or similar alcohol/chlorohexidine prep). Some surgeons cover the urethral meatus after prep with opsite or Tegaderm (3 M, St. Paul, MN) during surgery to exclude this area from the sterile area. Standard draping is performed. Our protocol limits unnecessary foot traffic in the room, and after draping is complete, the person draping the patient has to change their gown and gloves. Outer surgical gloves are changed frequently, and always before handling the device for the first time. Antibiotic irrigation is prepared and used extensively throughout the case. The device itself is soaked in a 10 cc vial of intravenous sulfamethoxazole/trimethoprim mixed 1:1 with saline, although other antibiotic soaking regimens may be used. Patients are generally given a weight-based dose of vancomycin (15 mg/kg) and once-daily dose of gentamycin (5–7 mg/kg) in the 30 minutes before incision. We use exclusively Coloplast products (Coloplast Corp., Minneapolis, MN) as we find them more suited to transgender phalloplasty from a design standpoint.
Other small and “clean” surgeries may be performed at the same time (glansplasty, etc.), but clean-contaminated surgeries should be avoided (e.g., urethroplasty). If desired, we also place testes prostheses through a separate scrotal incision on the opposite side of the prosthesis pump, or rarely through the same pubic incision if the vascular pedicle to the phallus can be safely avoided.
We prefer to delay penile prosthesis until at least 9 months have passed from the time of phalloplasty , or in the event the patient has had a urethral stricture repair, 9 months from the last urethral surgery, to make sure that the critical period for any urethral stricture occurrence/recurrence has passed. Subsequent repair of urethral stricture may be difficult or impossible with a penile prosthesis in place.
70.3.2 Surgery

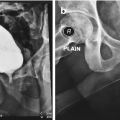
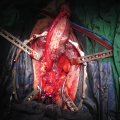
Infrapubic incision over the inferior edge of the pubis. The incision is brought down to the bone, and the underside of the pubis cleared off to make space for the rear of the cylinder

Related posts:
 Changing Scenario of Urethral Stricture Management
Changing Scenario of Urethral Stricture Management
 Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
 Reconstruction in Female-to-Male Gender Affirming Surgery
Reconstruction in Female-to-Male Gender Affirming Surgery
 Complications of Gender-Affirming Surgery
Complications of Gender-Affirming Surgery
 Reconstruction of Panurethral Stricture Disease
Reconstruction of Panurethral Stricture Disease
 Private: Reconstruction of Pelvic Fracture Urethral Injury
Private: Reconstruction of Pelvic Fracture Urethral Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


