div class=”ChapterContextInformation”>
4. World Changing Scenario of Urethral Stricture Management
Keywords
Urethral strictureUrethrotomyDirect visual internal urethrotomyUrethroplasty4.1 Introduction
Urethral stricture etiology: DC vs. UDC
UDC |
Trauma |
Lichen sclerosis |
Infection |
Iatrogenic |
Idiopathic |
DC |
Idiopathic |
Iatrogenic |
Trauma |
Lichen sclerosis |
Infection |
The basic management of male urethral stricture consists of urethral dilatation, internal urethrotomy, stenting and open reconstructive surgery. In 1949 Scardino and Hudson published the declaration that urethral dilatation for stricture was “useless”. Most urologists still routinely use internal urethrotomy or dilatation, although evidence shows no definitive satisfactory outcome with this approach. Endoscopic urethral surgery and urethral dilatation can transiently improve urinary flow; however open urethral surgery is now regarded as the gold standard treatment for urethral stricture disease [8, 11–16].
The choice of endourologic surgery or open urethroplasty depends on etiology, location, length and character of the stricture. The initial management of the male urethral stricture has become increasingly debatable. Proper initial management is the best chance to correct the stricture and the failure rate increases with subsequent surgery. Many urologists still believe that there is a “reconstructive ladder” and that treatment should always start at the bottom with dilatation and or internal urethrotomy and work up the ladder to open reconstructive surgery as the last resort. The published data has shown that there is a 50% stricture free rate with internal urethrotomy or dilatation, exclusively in patients who have a single, previously untreated, short, membrane-like stricture of the bulbar urethra [8].
Surgical treatment for urethral stricture disease has been adopted worldwide with significant improvement of outcomes and simultaneously a decrease in complications. Various surgical techniques have been developed in the last 30 years and are being used to repair anterior and posterior urethral stricture or stenosis with the goal of reducing morbidity and obtaining the best outcome with less complications. Since the late 1980s, buccal mucosa grafts have gained popularity as a surgical technique during urethral reconstructive surgery. There are many reconstructive surgical techniques, and no one technique is appropriate for all stricture diseases [15]. The different techniques of surgical intervention are documented and presented in the literature by various authors from different countries. Several factors play a role in the decision of open surgical treatment such as location of the stricture, cause of the stricture, previous urethral surgeries, the quality of the urethral plate, availability of autologous tissue to be used as flaps or grafts, experience, expertise and the preference of the treating urologist [16]. The urethral reconstructive urologist is requested to be familiar with the use of various techniques to deal with any etiology, location, length and characteristics of the stricture. Proper patient selection and reconstructive techniques will play a role in terms of successful management.
Standardizing urethral stricture evaluation, management and follow-up according to guidelines with grading recommendations will help to improve practice. In 2013, the American Urological Association (AUA) releasedguidelines written by the Male Urethral Stricture Guideline Panel of the AUA Education and Research, Inc. In 2010, the International Consultation on Urological Disease (ICUD) panel on urethral stricture bringing more consistency to the literature in terms of terminology, definition and specific management recommendations. Strictures can be divided into two main types, anterior and posterior, according to the underlying pathogenesis. Understanding the etiology of urethral strictures plays an important role in deciding on the specific type urethral reconstructive surgery . In the past, urethroplasty was only considered after failure of instrumentation or occurrence of complications. However, medical care has improved and the procedure has become safer [17, 18].
In this chapter, we will discuss the changing landscape of urethral stricture management. An historical perspective will be given as well as a discussion of the present treatment options. Minimal invasive therapies including urethral dilatation, urethral stenting, internal urethrotomy and other endoscopic options are making way for open urethral reconstructive surgeries due to its curative intention. The role of urethrotomy and other minimally invasive interventions in the management of urethral stricture disease will also be discussed.
4.2 Historical Perspective
Urethral stricture disease is as old as human civilization. It is one of the oldest known urological diseases. Reports have been documented in ancient Hindu, Egyptian and Greek literature. In ancient India, Sushruta described in Ayurveda (the traditional Hindu system of medicine) the use of graduated dilators made of metal or wood. Urethral dilators were mentioned in 3000 BC in the ancient Egyptian tombs of pharaohs to dilate the strictures in the after life. This demonstrates that having an urethral stricture meant having it for life, as well as in the after life [15, 19].
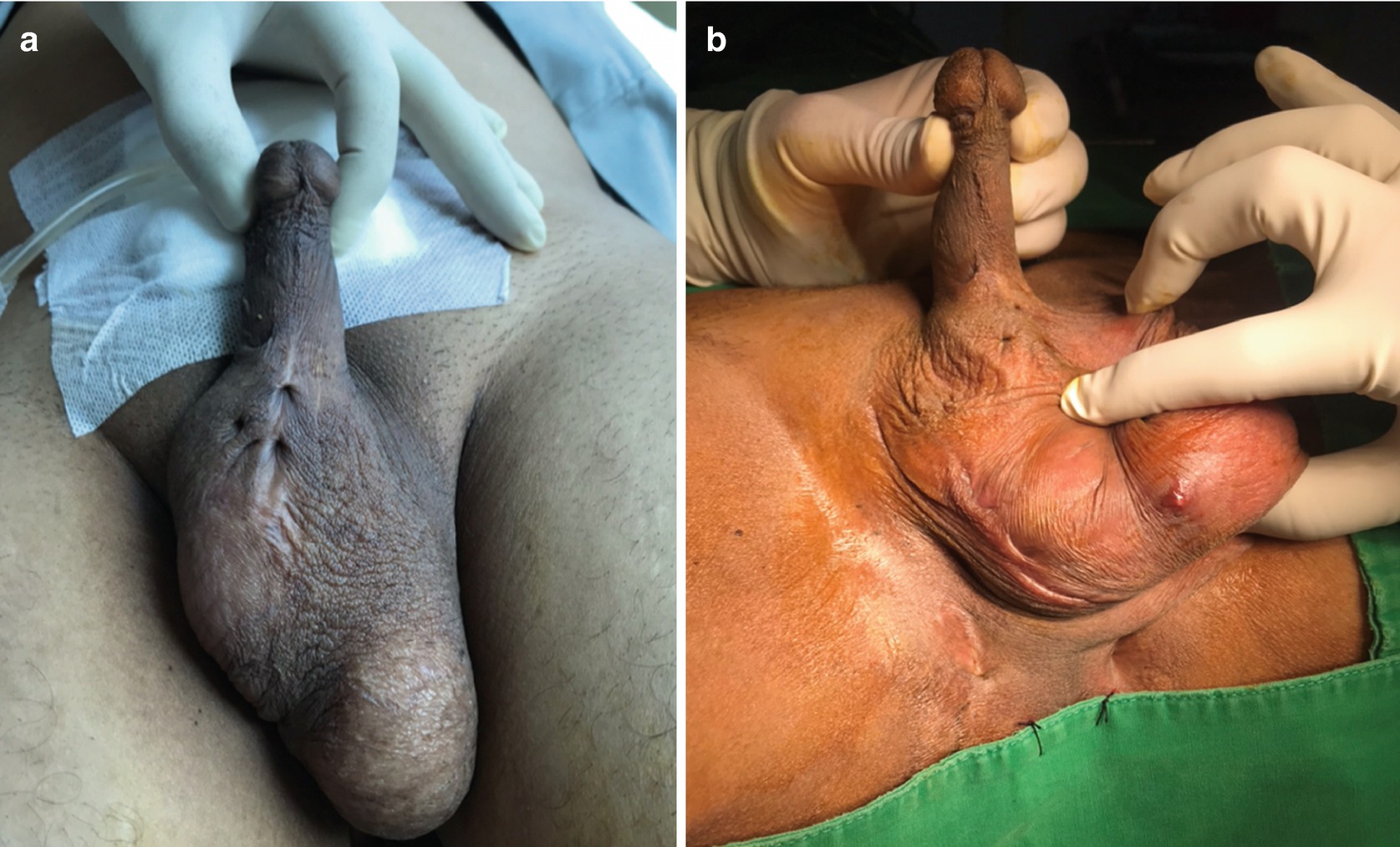
Urethrocutaneous fistula . Three fistulae (a) and nine fistulae (b)
The pioneering development of urethroplasty started in the 1950s and1960s. Since then, there have been two basic principles of surgical treatment, anastomotic urethroplasty for short strictures and substitution urethroplasty for long strictures. In 1953, Johanson applied Denis Browne’s buried skin strip technique to adult male strictures. Surgeons all around the world adopted this new two-stage urethroplasty. It was successful in relieving hundreds of patients from a suprapubic tube and the periodic torment of urethral dilatation. The Johanson’s two-stage technique became so successful that it was used in more and more simple strictures. Nevertheless, the procedure was considered as a complex and difficult operation for a general urologist [15, 20].
The discovery of optical urethrotomy by Hans Sache from Nurnberg in 1971 became the gold standard of today’s endoscopic stricture treatment. During his time at the Department of Urology at University of Munich, he evaluated internal urethrotomy with the electric knife. He found that the necrosis following the electric incision caused scarring and that this side effect could be avoided for the most part by simple cold-knife incision. In June 1971 he conducted his first operation with the prototype of a cold-knife urethrotomy built by Karl Storz Co., Tuttlingen [21].
The discovery of cold-knife urethrotomy as a minimal invasive procedure decreased the popularity of urethroplasty. The procedure was considered elegant, easy and safe with a reported 23% re-treatment rate. Many urologists began to question the place of urethroplasty in the context of Sachse’s optical urethrotomy . The results were that the number of urethroplasties globally fell dramatically [22]. Optical urethrotomy was started for all types and locations of urethral stricture, obliterated and non-obliterated, single or multiple strictures for the next several decades and became the most popular treatment option in the management of urethral strictures.
During the 80s and 90s, many studies showed very interesting rates of success for the endoscopic urethrotomy of urethral stricture management and contributed to the popularity of this method. Some authors even argued the case of “cut to the light” procedure for totally obliterated stricture and intense spongiofibrosis. A review done by Passadoro and Emiliozzi observed a success rate for endoscopic urethrotomy from 56% to 96% in 23 articles. The procedure could be done on an outpatient basis, especially under local or loco-regional anesthesia and this contributed to the popularity of the procedure [23].
Despite the promising results published initially, a contemporary review of the available evidence regarding the success rate for endoscopic urethrotomy was not as favorable, especially in the long-term. Many studies suggest that dilatation and urethrotomy offer equivalent outcomes, but urethrotomies are associated with a high recurrence rate of the stricture requiring repeated procedures over a relatively short period of time. The failure after initial urethrotomy is reported to be 50% and some authors suggest that endoscopic treatment using dilatation or internal urethrotomy exacerbates scar formation and can add to the length and severity of the stricture. It is also reported that after second internal urethrotomy, the failure rate can be as high as 100% [11, 24, 25]. Santucci R et al. [11] performed a retrospective study of more than 100 patients to evaluate the stricture free rate after a single attempt of internal urethrotomy, and after a second, third, fourth and even after a fifth procedure. He concluded that urethrotomy had poor performance characteristics. The success rates after a first urethrotomy was only 9% after 1–3 years follow up and after multiple urethrotomies it was close to 0%. Additional studies also showed that one dilatation or endoscopic urethrotomy does not complicate stricture characteristic but repeated treatments are associated with increase stricture complexity and are potentially counterproductive [26]. Furthermore, the published data also showed that endoscopic treatment is less effective and cost-effective than urethroplasty [25, 27]. However, many centers of urethral reconstructive urology showed a significant result in terms of stricture free rate for patients treated with urethroplasty . A Cochrane review showed the success rate of urethroplasty to be between 85% and 90% for a simple procedure and about 80% for extreme complex reconstruction. Although no randomized controlled trials were done to compare the effectiveness of internal urethrotomy and urethroplasty, some studies showed that long-term success rates are much higher for urethroplasty (85–90%) than internal urethrotomy (20–30%) [28, 32].
The urological community began to realize that endoscopic urethrotomy is rarely curative and the patient often needs repeated procedures or regular self-dilatation. The scarring in the underlying urethra and adjacent tissue needs to be excised or replaced by healthy epithelium to achieve a cure. Once again, the urological community was questioning the role of endoscopic urethral surgery in the treatment of urethral stricture disease and also questioning the optimal indications for internal urethrotomy or dilatation.
The unsatisfactory result of internal urethrotomy and dilatation led to various attempts being made to modify and increase the durability of this technique. Such approaches included post-endoscopic urethral catheterization, clean intermittent catheterization (CIC), laser urethrotomy, urethral stenting, antifibroblast and anticollagen injections and steroid injections. None of these modifications could reach as successful rates as open urethral reconstructive management . Following this, urethral stenting was largely abandoned and removed from the market because of limited use and a high rate of complications such as perineal pain, stent migration, stent obstruction, incontinence and infection. Trials are being conducted on the future use of tissue engineering and scar modulation [19, 29–32].
Surgical treatments for urethral stricture disease have been adopted worldwide with significant improvement of successful outcomes and simultaneously a decrease in the complication rate. Urethral surgical technique modification and improvements have been made during the last 30 years to be used in the repair of anterior and posterior urethral stricture/stenosis with the ultimate goal of reducing morbidity and obtaining the best outcome with the least complications. The concept of open urethral reconstructive surgery as a complex and difficult operation is starting to change. Most reconstructive surgeons consider urethroplasty to be the gold standard management for urethral stricture and stenosis. Current data for both EPA and substitution urethroplasty show higher long-term success rates than any other form of management of urethral stricture [32]. From an economic perspective, multiple studies have evaluated the cost-effectiveness of treatment of urethral stricture and found that either immediate urethroplasty or a single attempt of internal urethrotomy, followed by urethroplasty if the procedure failed, was more cost-effective than long-term dilatation or internal urethrotomy with urethroplasty used only for salvage procedures [25, 27].
4.3 Global Standardization of Guidelines for Urethral Stricture Management
Related posts:
 Reconstruction of Post-TURP Urethral Strictures
Reconstruction of Post-TURP Urethral Strictures
 Treatment of Male Stress Urinary Incontinence: An Overview
Treatment of Male Stress Urinary Incontinence: An Overview
 Reconstruction in Female-to-Male Gender Affirming Surgery
Reconstruction in Female-to-Male Gender Affirming Surgery
 Complications of Gender-Affirming Surgery
Complications of Gender-Affirming Surgery
 Reconstruction of Panurethral Stricture Disease
Reconstruction of Panurethral Stricture Disease
 Private: Reconstruction of Pelvic Fracture Urethral Injury
Private: Reconstruction of Pelvic Fracture Urethral Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


