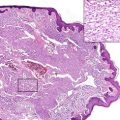
Fig. 66.1
CD8+ AECTCL: Clinical presentation with disseminated erosive plaques on the trunk (By courtesy of Dr. Dipendra Gurung, Kathmandu, Nepal)
Pathology
Histology shows prominent epidermotropism of mostly small to medium atypical lymphocytes with chromatin dense nuclei (Figs. 66.2 and 66.3). Apoptotic keratinocytes and spongiosis are commonly found, and blister formation may occasionally be seen. Extension of the lymphocytic infiltrates into the deeper dermis and subcutis with angiocentric growth and destruction of adnexal structures can occur. Hemorrhage is common.
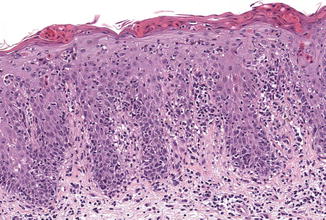
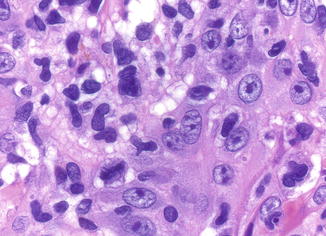
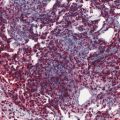
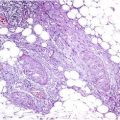
Fig. 66.2
CD8+ AECTCL: Superficial band-like infiltrate with epidermotropism and ulceration
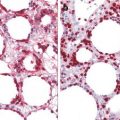
Fig. 66.3
CD8+ AECTCL: Epidermotropic infiltrate of small- to medium-sized lymphocytes with convoluted nuclei (Note apoptotic keratinocytes)
The tumor cells express CD3, CD8 (Fig. 66.4), and CD45RA, betaF1, as well as TIA-1 and other cytotoxic proteins, but are negative for CD4, CD30, CD56, CD45RO, and often CD5. The proliferative index (Ki-67) is high (>50 %). A CD2− CD7+ phenotype seems to be associated with a more aggressive course. A clonal rearrangement of T-cell receptor genes can be demonstrated in most cases. There is no association with Epstein–Barr virus.
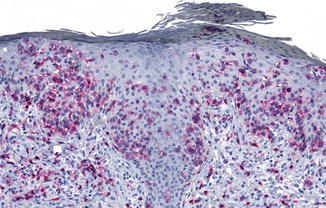
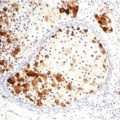
Fig. 66.4




CD8+ AECTCL: Characteristic expression of CD8 by tumor cells
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
