Fig. 16.1
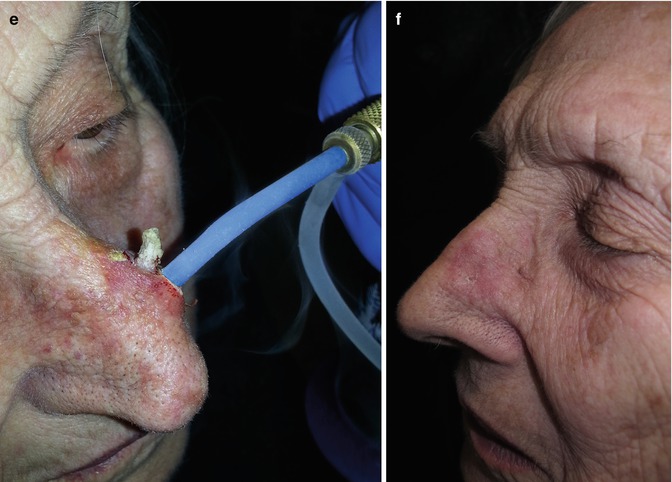
(a) Large double cutaneous horn on the nose of 93-year-old patient; (b) dermoscopy image of the double cutaneous horn; (c) cryotweezer used for freezing the largest lesion down to the base; (d) removal by shaving of frozen lesion (histopathology reported a well-differentiated invasive SCC); (e) contact freezing with 4 mm probe; the same procedure was performed of the smaller lesion; (f) postoperative result after 1 month
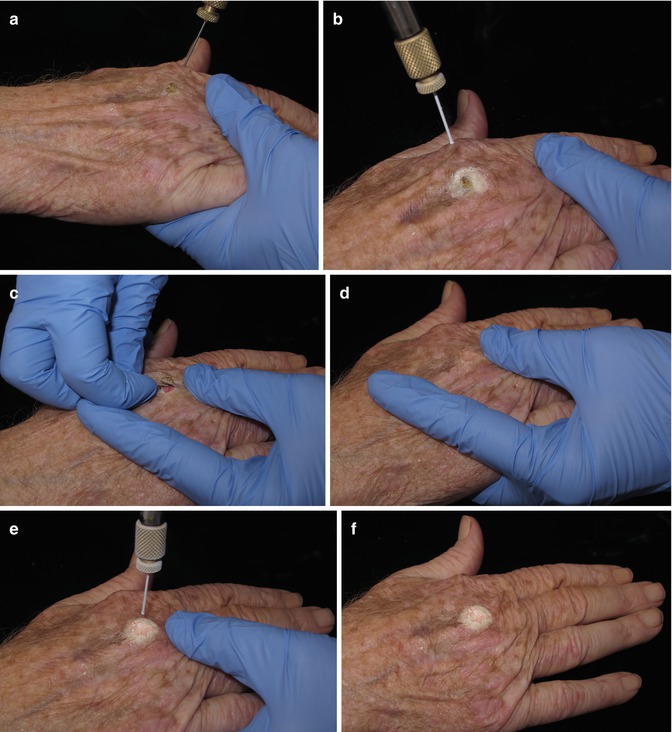
Fig. 16.2
(a) Open (spraying) freezing of a hyperkeratotic AK. (b) Leaving a 1–2 mm margin. (c) Shaving during thawing. (d) Hemostasia at the base was followed by (e) one spray freeze-thaw cycle with a freezing front that covered the base and 1–2 mm margin (f)
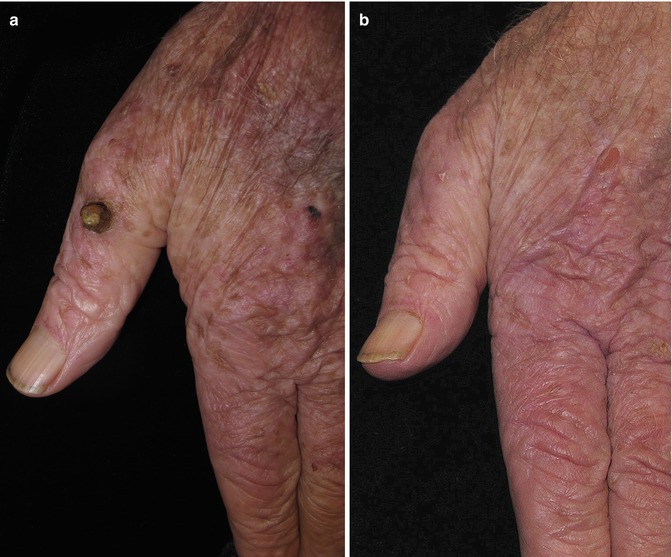
Fig. 16.3
(a) A hyperkeratotic lesion on the left hand thumb done with freeze spraying-shaving-hemostasia-freezing at the base and biopsy (which reported an in situ SCC); (b) result 4 months later
16.2.2 Field Treatment
Several therapeutic approaches are available for field treatment. Once applied, patients are the first to notice the improvement: they report softer sensation when touching the treated areas, less scaling, and improved appearance.
Before and after clinical photography aids physicians in confirming such changes. We believe there is the need to develop image change detection algorithms to calculate mathematically such improvement. Changes are easier to detect in infrared photography, which highlights keratin (white) and vessels (black). A simple way to obtain infrared-like images is through image processing [22]. Most photography editing programs have incorporated such a feature.
16.2.3 Cryopeeling
By far, the largest experience of cryopeeling for field cancerization has been reported by Chiarello [23]. In 2000, he published his long-term follow-up results on the use of extensive cryosurgery to treat areas of field cancerization on 373 patients. 34,604 individual AK were treated by open (spraying) technique and the surrounding areas were sprayed at a distance of approximately 5 cm, in a paint brush or circular fashion until the entire area was frozen. For cryopeeling, an acne tip can work very nicely as well (Fig. 16.4) since it allows for feathering the liquid nitrogen in a lineal pattern and covers large areas at once. Chiarello’s data show that cryopeeling is twice as effective as 5FU when measured 1–3 years post cryosurgery. The number of SCC recorded over 5–6 years was 33 with no metastases, a much lower number than predicted if AK had been left untreated [23].

Fig. 16.4
Cryopeeling with acne aperture which feathers LN in a linear pattern
Pain can be an issue when freezing large areas, especially on the head. Chiarello suggests using EMLA or 30 % lidocaine mixed in acid mantle cream vigorously applied after freezing. The immediate post-thawing vasodilation and skin barrier breaking will permit a rapid penetration and relief in seconds; block anesthesia is also an option as well as local injections or “blebs” of 1 or 2 % Xylocaine with epinephrine followed by massage [23].
The results are quite spectacular because most benign lesions are removed as well (seborrheic keratosis, lentigos solaris) (Figs. 16.5a–c, 16.6a–c, 16.7a–c, and 16.8a–c). Likewise, make sure the whole field has been carefully examined to avoid peeling away by freezing lesions that needed other treatment procedures.
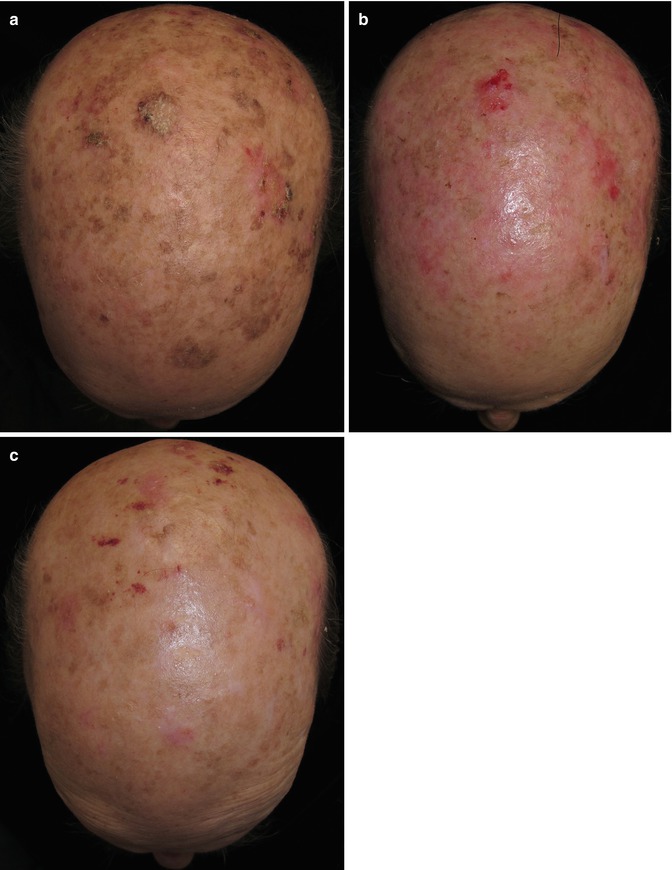
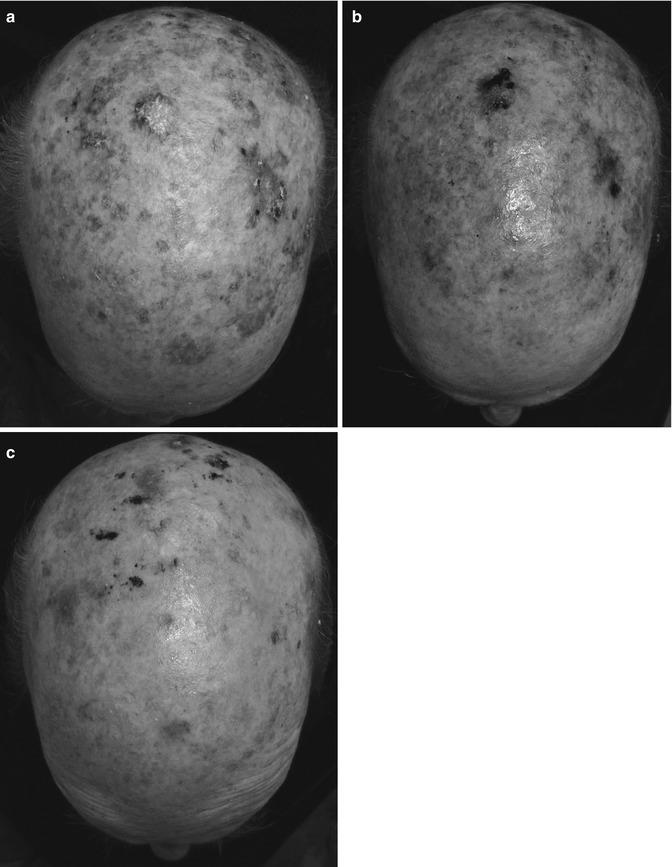
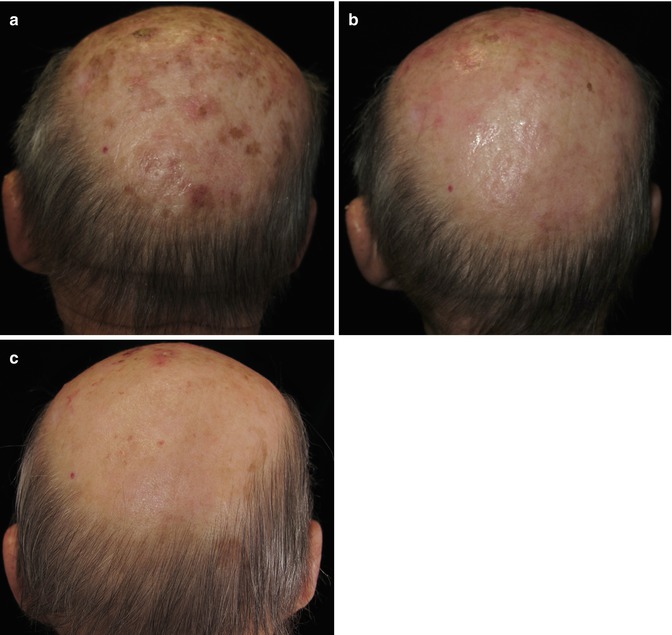
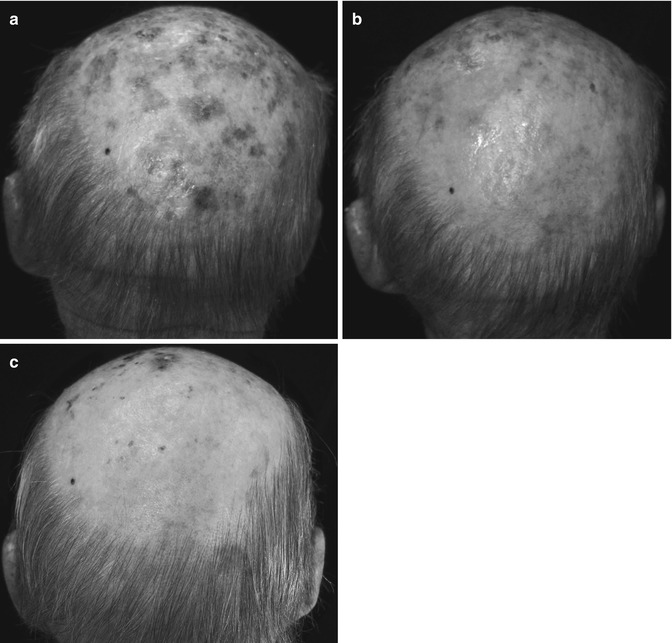
Fig. 16.5
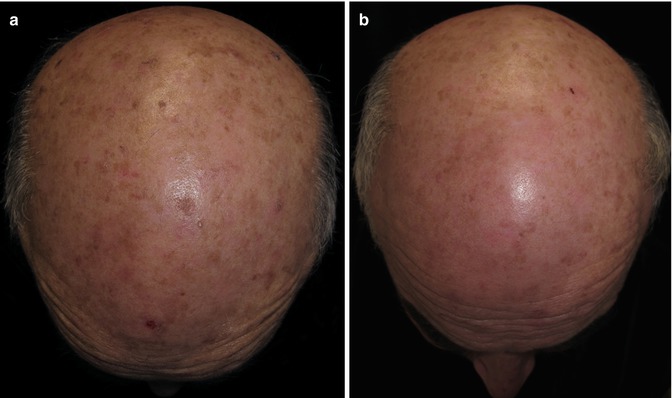
Cryopeeling on sun-damaged scalp. (a) Before; (b) 3 months after treatment; (c) 9 months after treatment
Fig. 16.6
Same patient as in Fig. 16.5 with image processing (infrared) which (a) allows to assess the extent of the damage (the hyperkeratotic lesion at 12 looks white due to high content of keratin); (b) 3 months post treatment (the hyperkeratotic area at 12 looks black due to redness post cryo, which was deeper in this area because of excess keratin); (c) general improvement in the amount of white (keratotic lesions) and black (redness post cryo and redness from sun damage)
Fig. 16.7
Cryopeeling on sun-damaged area on the occipital area of the scull (a) before, (b) 3 months, and (c) 9 months after treatment
Fig. 16.8
Same patient as in Fig. 16.7 with image processing (infrared) which (a) allows assessment of the extent of the damage (redness is seen as black; keratin is seen as white); (b) 3 months post treatment; (c) 9 months after treatment with almost no black lesions (hypervascularization)
16.2.4 Combination Treatment
Combining different treatments has two purposes:
Summing Up. Adding up two different mechanisms that run in parallel and that maximize the combined clinical outcome. Such is the case of field plus single-lesion treatment combination. In general, field treatment is best for superficial and also for nonclinical damage but insufficient for thick individual lesions. Individual treatment (topical or procedural) is usually more destructive and thus best for thick localized lesions. Some authors have suggested the use of topical or injected substances to augment or assist cryosurgery [24] based on concepts taken from the field of cryopreservation. The concept is valid and additional clinical studies aimed to establish such possibility are warranted.
Potentiate. Two individual treatment options can be maximized by having them work simultaneously or sequentially. The end result should be better than either option applied individually. For example, in the section dealing with keloids, Lopez combines freezing and local corticoid infiltration sequentially. He proposes infiltration of corticosteroid into the fibrous tissue a few minutes (10–15 min) after the last freeze-thaw cycle; keloid tissue edema “softens” the tissue and the injection is greatly facilitated. A higher volume of the drug can be injected into the tissue after the freezing compared with the amount that can be injected without a previous cryosurgery.
In immunocryosurgery, imiquimod is combined with freezing in such a way that the final amount of the topical drug and freezing is less than that used if either approach would be applied separately. The end result is better than with either treatment used separately. This concept (Chap. 3) and its application (Chap. 20) have deserved two entire chapters in this book.
Baust et al. state that since most chemotherapeutic agents initiate apoptosis in cancer cells, subfreezing (which can occur at the periphery of tumors treated with cryosurgery) applied sequentially with low-dose chemotherapy improves cancer cell death in the periphery [25].
In skin cancerization, when a topical treatment is applied before cryosurgery, part of the benefit is related to the loss of the superficial layers of the epidermis. Keratin is a bad conductant of cold; therefore, a desepitelized surface will allow a better and more regular expansion of the freezing front.
When cryosurgery is applied at the start, edema, vasodilation, and also loss of superficial skin layers will allow topical treatments to be absorbed better.
Some authors have suggested that large-diameter lesions (greater than 1 cm) and the presence of pain predict conventional treatment resistance either to topical monotherapy or cryosurgery [26] and require combination treatment.
Some combinations with cryosurgery are:
Get Clinical Tree app for offline access

1.
Acitretin/tretinoin: Oral acitretin has been used in transplant patients with clinical improvement (probably due to peeling off the stratum corneum) although no changes in proliferation were observed. Its potential combination with cryosurgery requires consideration and further studies [27]. The use of topical tretinoin in combination with cryosurgery has no formal support, but it is used in the treatment of AK [28] and for preparation on skin before cryopeelings or treatment of multiple lentigos of face and/or dorsum of hands.
2.
5 Fluorouracil: Cryosurgery with 5 FU is probably the most used topical treatment but underused in combination despite evidence of its benefit. In fact it is used only on 1.1 % of actinic keratosis treated [29]. Evidence shows that 0.5 % fluorouracil has similar efficacy and is better tolerated than 5 % fluorouracil. It has proven beneficial in 1-week treatments with once-daily use followed by cryosurgery [30]. Extending treatment for up to 4 weeks further improved AK lesion clearance rates [31, 32]. The use of this drug before freezing eliminates some cancerous cells and leaves others in apoptosis; with freezing, there will be increase in cell death when compared to either application alone [33] (Fig. 16.9a, b, 16.10a, b, and 16.11a, b).
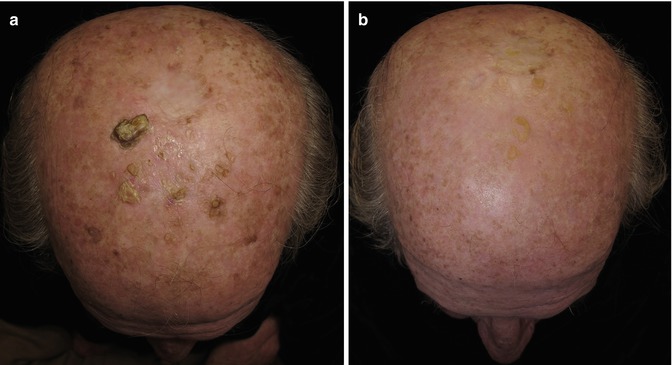
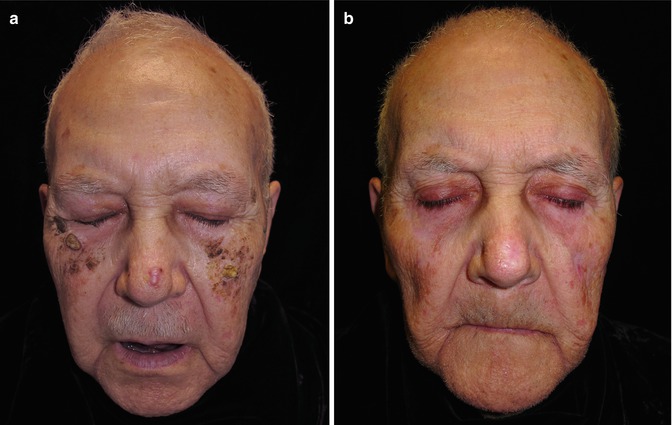
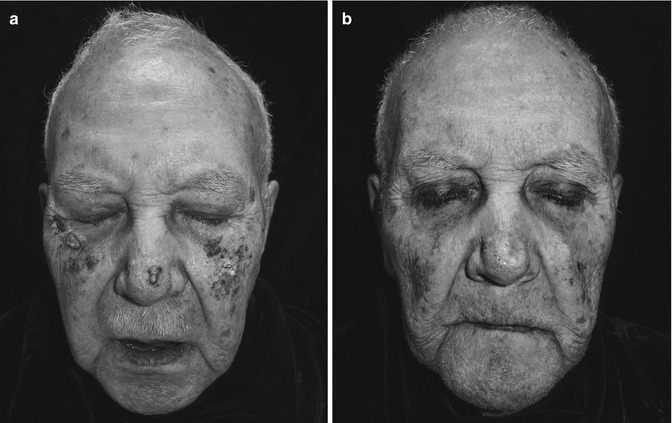
Fig. 16.9
(a) Severe sun-damaged scalp. 5 % 5FU was indicated daily for 3 weeks, and then individual residual lesions were treated with one freeze-thaw cycle; (b) control image after 13 months
Fig. 16.10
(a) Severe field cancerization on the face. Three weeks of 5 % 5FU in the evenings was followed by cryosurgery (one freeze-thaw cycle on residual lesions). The BCC on the nose was treated with close (probe) technique with a double freeze-thaw cycle. (b) One year later
Fig. 16.11
Same patient as in Fig. 16.10a, b. Image processing (infrared) to highlight affected areas before and after treatment
3.
Imiquimod: Combination of imiquimod with cryosurgery deserves more than one chapter. In Chap. 3, Krunic has reviewed the theoretical aspects of immunocryosurgery while Gaitanis and Bassukas in Chap. 20 have gone through the applications on NMSC. New combinations are using 3.75 % instead of 5 % imiquimod followed by directed (not standardized) cryosurgery [36, 37].
4.
Diclofenac sodium 3 % gel may work by inhibiting cyclo-oxgenase-2 (COX-2) as an angiogenesis inhibitor and inducing apoptosis; used alone, complete clearance is on the order of 58 % [38]. Some authors have reported clearance of 71 % with diclofenac by the end of the 12-week topical treatment; cryosurgery was done on residual lesions [39]. In another study, cryosurgery on selected lesions followed by 3-months twice-a-day treatment with diclofenac achieved a 100 % clearance [40] (Figs. 16.12a, b, 16.13a, b, 16.14a, b, 16.15a, b, 16.16a, b, and 16.17a, b).
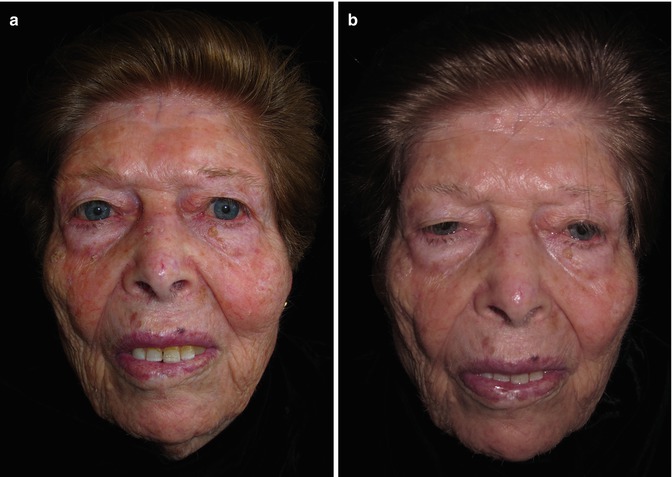
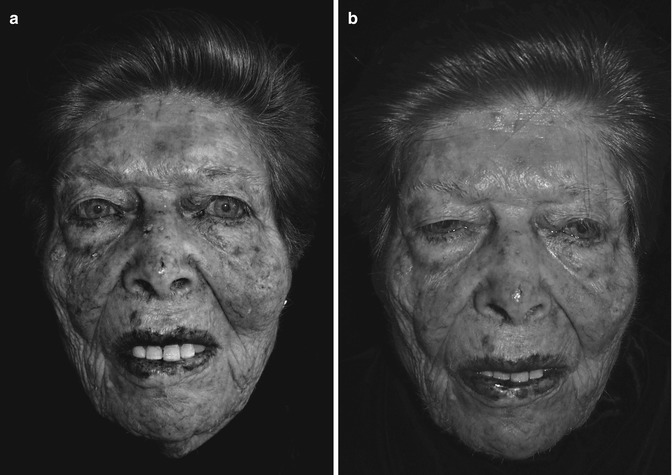
Fig. 16.12
(a) Severe skin cancerization of the face treated with Solaraze® (PharmaDerm, Melville, NY) (3 % diclofenac sodium) applied topically twice a day for 3 months; (b) 3 months after the end of treatment
Fig. 16.13
Same patient in Fig. 16.12a, b with image processing (infrared) to highlight sun damage before treatment (a) and improvement 3 months after completion of treatment (b). Cryosurgery was applied as cryospray over few residual lesions