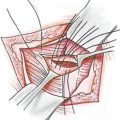
Picture 11.1
Covering the incision line with strips
The umbilical area requires special attention. Protecting the suture line in this area from maceration is highly important. The dressing applied to this area with antibiotic pomades during the operation is uncovered on the third day at the first dressing change, and it can be left uncovered since epithelialization is completed then. It is enough to clean and put pomade on the area daily over 10 days. One should be careful in cases of redness and discharge in this area and try to control the local infection in the early period with oral antibiotics and sterilizing agents used for wound care, if necessary (Picture 11.2).
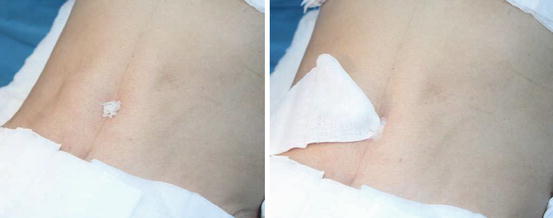
Picture 11.2
Umbilical area dressing
Desired abdominal shape is ensured in the early period by pressure applied on the nature-identical sulci created on the midline and as lateral to the rectus. Besides, with pressure on these areas, the flaps adhere to the base within a short time and the risk of complications, such as seroma, decreases [2]. After the gauze sponges are placed, the abdomen is pressured with tensile bands from the lower end of the costa to the suprapubic area (Pictures 11.3, 11.4). The corset worn over all these dressing should be used for 3 weeks (Picture 11.5).



Picture 11.3
Abdominal dressing after covering the incision line after operation. Placing the sponges and covering with tensile plasters
Picture 11.4
Covering the whole abdominal area with tensile plasters
Picture 11.5
View of patient with corset worn over the dressing
This dressing can be removed after the postoperative third day or can be maintained up to 1 week depending on the surgeon’s choice. Dressings, apart from strips, do not need to be replaced after removal. After checking the suture line and umbilical area and explaining the daily abdominal care to the patient, a corset can be worn. After removing all dressings of the patient on the third day, the patient is allowed to take a shower while maintaining the strips.
11.2 Hospital Follow-Up
Postoperative hospital care varies for every patient. It typically falls between 24 and 72 h. If all goes well in the follow-up of the patient, the patient can be discharged from the hospital within 24 h.
The parameters to be followed are:
Mobilization
Drain follow-up (bleeding and seroma follow-up)
Blood pressure follow-up
Prevention of DVT
Prevention of pulmonary problems
Pain control
11.2.1 Mobilization
The patients are encouraged to get mobilized as soon as the sixth hour postoperatively. This is important for the prevention of many complications like respiratory insufficiency and DVT.
11.2.2 Drain Follow-Up
Prevention of early hematoma is of primary importance in the postoperative period. Rates of hematoma reported in the literature are in the range of 0.8–3 % [3].
Another problem, which is observed more frequently than hematoma, is seroma in abdominoplasty follow-up [4]. It arises when lymphatics in the deep fat tissue are damaged after surgery. While bleeding is observed frequently within the first 24 h, the incidence of seroma increases later on. Therefore, there are various protocols for follow-up of patients with drains. There are protocols recommending follow-up up to 7 days with drains to avoid from seroma in patients with wide dissections. In addition, other protective methods tried include decreasing dead space with sutures or facilitating adherence of the flap to the base with fibrin glue and protecting the Scarpa fascia on the base during the dissection [5].
However, since there is no wide dissection in our technique with minimal dead space, we use only closed drain systems. We keep drains until less than 30–40 cc/24 h and their contents become serous. This process is usually completed within the first 24 h in many patients. Depending on the surgeon’s choice, two silicon or Jackson-Pratt drains placed on the incision line or suprapubic area will be enough.
Postoperative hematoma or seroma generally restrict themselves; however, if the accumulated blood is not detected in the early period, it may lead to necrosis on the flap area due to the pressure it causes and wound healing problems due to tightness on the suture line [6]. In suspicious cases, the abdomen should be checked by removing the dressing. Ultrasonography (USG) is the most valuable method in early period diagnosis. While it is difficult to discharge hematoma with an injector in the early period, it becomes easier due to fall of fibrin within the following days.
11.2.3 Blood Pressure Follow-Up
While a TA follow-up with 4–6-h intervals within the first 24 h after operation is enough for patients with no hypertension problems, this must be more frequent for patients with previous medical history. Preoperatively used medication must be screened carefully, and any existing antihypertensive drugs must be continued. Severe pain and improper liquid uptake in the postoperative period may lead to fluctuations in tension values of patients. Hypertension problems in the early period are the most important risk factors increasing the hematoma [7].
One should be careful with the liquid treatment and avoid charging excessive volumes to the patient. Cardiology consultation should be requested for patients who still have tension fluctuations and TA values over 150–100 mmHg despite meeting all these criteria [8].
11.2.4 Prevention of Deep Vein Thrombosis
Venous thrombosis begins in areas in stasis, particularly on the small veins in the legs. Hypercoagulability associated with surgical stress and trauma increases the risk of venous thrombosis associated with hypotonia on the leg muscles during anesthesia. Thrombosis is firstly caused by the obstruction in the vein [9]. If the obstructed vein is a major vein, distal venous pressure increases and edema occurs in the extremity. Rupture of the clot may occur and its embolization of the right heart and then the lungs threatens life [10].
Early postoperative mobilization is highly important to reduce venous stasis and prevent venous thromboembolism. Thromboembolic deterrent stocking and intra- and postoperative intermittent pneumatic compression boots worn during the operation and maintained within the first 24 h are the most important protection methods against thromboembolism [11, 12]. Low-molecular-weight heparin (LMWH) shall be the routine treatment in patients with major tissue removal and high-volume liposuction. SC Fraxiparine can be applied 1 h before the surgery. The doses up to 40 mg/g would not increase the risk of bleeding and can be used with confidence [13].
In healthy patients who do not have additional problems and achieve early postoperative mobilization, the abovementioned measures are enough. However, for patients with risk factors, a more detailed examination must be performed, and appropriate treatment shall be planned.
In 2011, the American Society of Plastic Surgeons’ task force compiled recommendations for thromboembolism prophylaxis in patients undergoing plastic surgery procedures including body contouring. Risk factors are defined in accordance with the 2005 Caprini Risk Assessment Model (RAM), and the risk group and treatment protocol to be applied to the patient were determined [14] (Tables 11.1 and 11.2).
Table 11.1
Risk factors for venous thromboembolism based on the 2005 caprini risk assessment model
One point for each risk factor | Two points for each risk factor | Three points for each risk factor
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|