13 Posterior Neck and Occipital Region
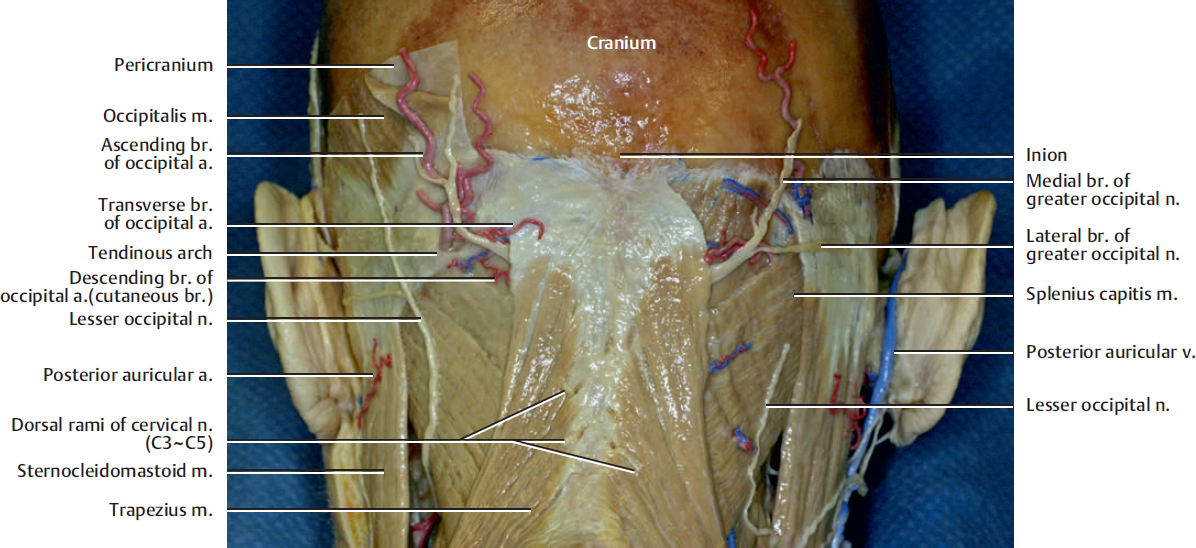
Fig. 13.1. The posterior neck region. The skin and the galea have been removed to leave the occipitalis muscle on the left side.
The occipitalis muscle has two muscle bellies that are separated in the midline by the aponeurosis. Each occipital belly arises from the lateral two-thirds of the supreme nuchal line of the occipital bone and from the mastoid process of the temporal bone. The muscle extends forward to become continuous with the galea aponeurotica. It is a part of the occipitofrontalis muscle, along with the frontalis muscle. It is innervated by the posterior auricular branch of the facial nerve. Its function is to move the scalp back.
The greater occipital nerve and occipital artery reach the subcutaneous tissues by passing between the attachment of the trapezius and sternocleidomastoid muscles to the superior nuchal line. The occipital artery crosses deep to the greater occipital nerve approximately 4 cm lateral to the external occipital protuberance (inion). After it pierces the deep fascia, it gives rise to three major cutaneous branches: descending, transverse, and ascending. The greater occipital nerve branches into medial and lateral branches around the superior nuchal line. It supplies the skin over the occipital part of the scalp up to the vertex of the skull.
The lesser occipital nerve has a variable origin either from the second or the second and third cervical ventral rami. The lesser occipital nerve lies at approximately 7 cm lateral to the external occipital protuberance. This nerve supplies the skin over the scalp and cranial surface of the upper part of the auricle.
The medial branches of the dorsal rami of the third, fourth, and fifth cervical nerves pierce the trapezius muscle at its paramedian position to supply skin over the back of the neck.
The trapezius muscle covers the back of the head and neck. It extends from the medial half of the superior nuchal line, the external occipital protuberance, and the spinous processes of the cervical and thoracic vertebrae and converges on the shoulder to attach to the scapula and the lateral third of the clavicle.
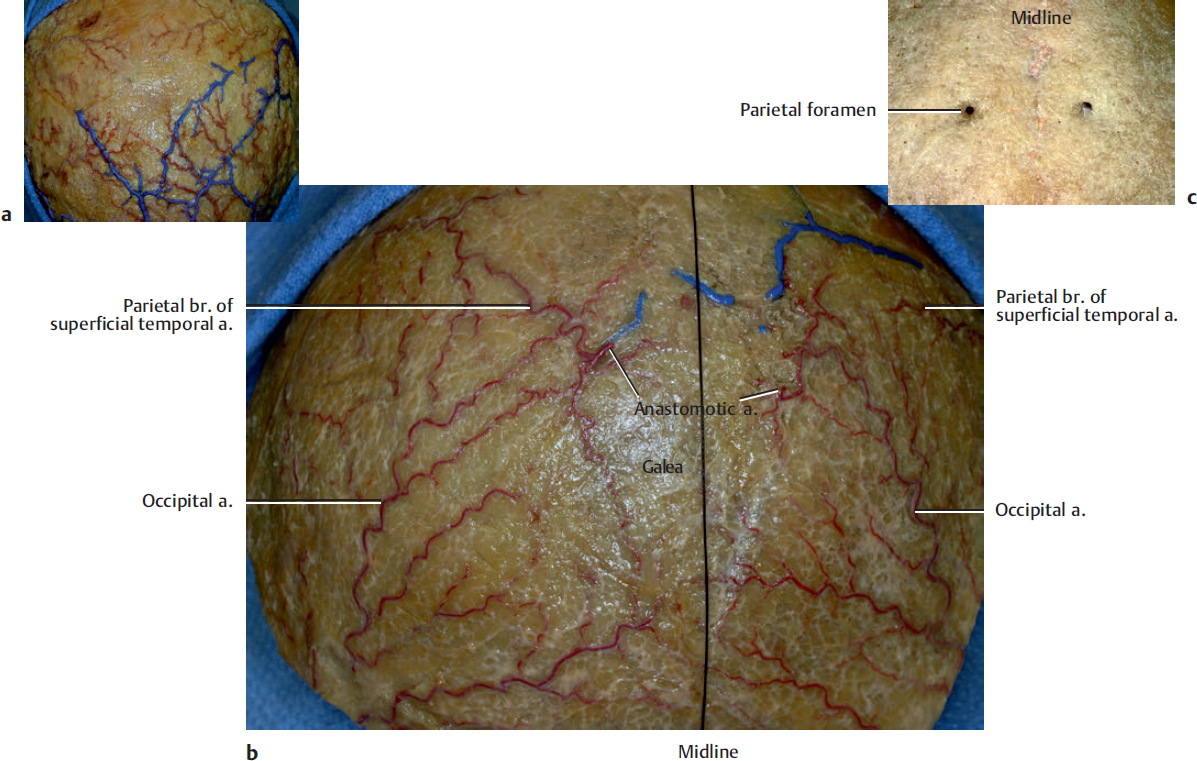
The branches from the superficial temporal, posterior auricular, occipital, supraorbital, and supratrochlear arteries freely anastomose in the scalp.
This figure shows the meningeal branch (anastomotic artery) from the occipital artery bilaterally which is passing through the parietal foramen. The well-developed anastomotic artery is found in approximately 50% of specimens, and it develops the vascular network of the galea and scalp. The rich vascular connection in the galea and scalp contributes rich vascularity to galeal and scalp flap in the head.
The parietal foramen is found in more than 60% of skulls. It may be unilateral or bilateral or duplicate on one or both sides. The vertical distance from the inion to the level of the parietal foramen is approximately 8 cm, and the distance from the midline to the foramen is within 10 mm (Fig. 13.2c).
The superficial temporal artery that supplies the galea does not cross the midline or anastomose with the contralateral superficial temporal artery on the galeal layer. The vein on the galea generally runs superficially on the artery except for the vertex region. The artery in the vertex region courses more superficially on the vein and anastomoses with the contralateral artery in the subcutaneous layer (Fig. 13.2a).
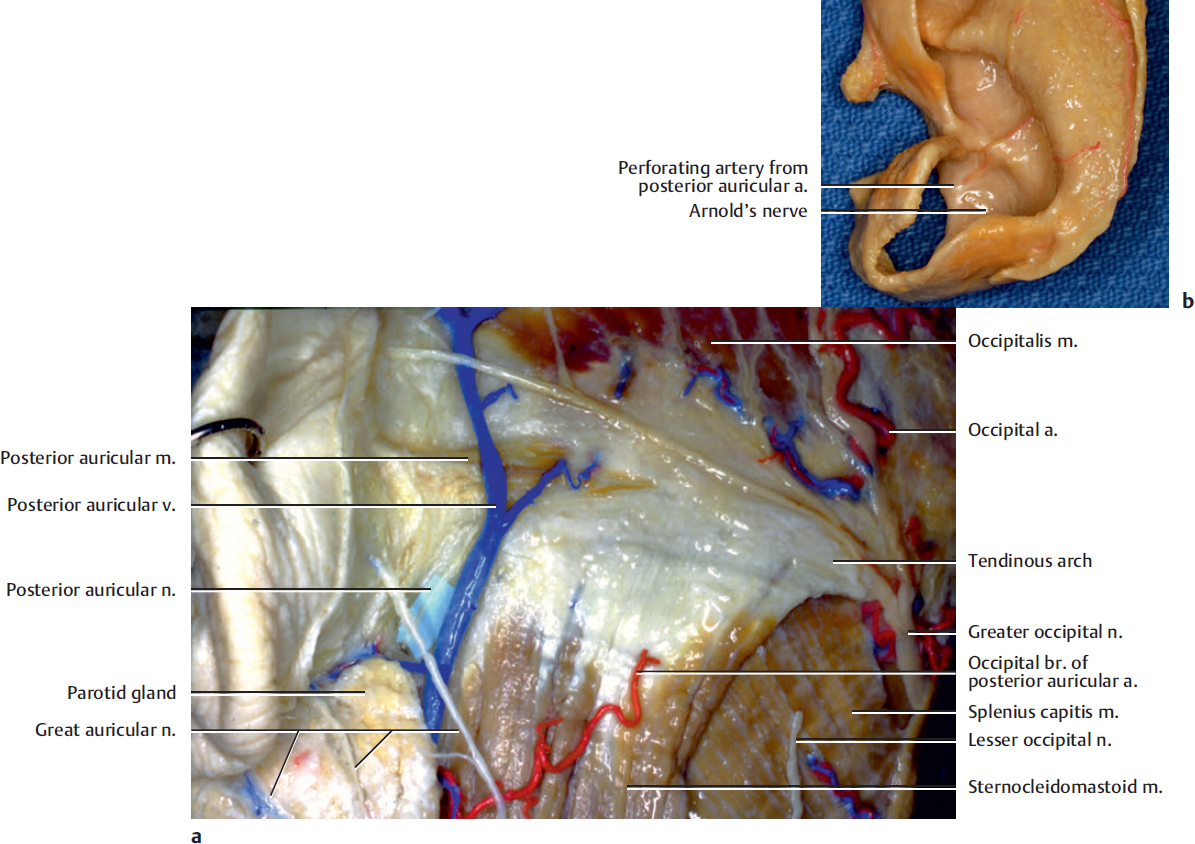
The posterior auricular nerve is the first extracranial branch of the facial nerve. It originates from the facial nerve close to the stylomastoid foramen and then courses posteriorly and upward on the surface of the mastoid bone. There, it is joined by a filament from the auricular branch of the vagus (see the text accompanying Fig. 2.2), which supplies the auricular concha as the Arnold’s nerve (Fig. 13.3b) and communicates with the posterior branch of the great auricular, as well as the lesser occipital, nerve. It supplies the posterior auricular and occipital muscles. The posterior auricular muscle arises from the mastoid bone and inserts into cranial surface of the concha. It displaces the auricle backward.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


