Popliteal Nerve Blocks
Ming Zhuo-Stine
Sarah Madison
DEFINITION
The popliteal nerve block targets the sciatic nerve in the popliteal fossa proximal to its bifurcation into the common peroneal and tibial nerves.
It is a commonly used block for surgeries involving the lower leg, ankle, and foot.
The nerve block can provide surgical anesthesia or postoperative analgesia. The duration of the block varies based on the choice of local anesthetic and the choice of single injection versus continuous catheter technique. For painful surgeries, the continuous catheter technique can provide several days of excellent postoperative pain control.1
The popliteal nerve block spares the medial aspect of the lower leg, an area that is innervated by the saphenous nerve. A femoral or saphenous nerve block must be performed in conjunction with a popliteal block for full sensory blockade of the lower leg (FIG 1).
ANATOMY
The sciatic nerve consists of two distinct nerves, the tibial and common peroneal nerves, which provide motor and sensory innervation to the majority of the lower leg. The two nerves have their own epineurium and are encased in an additional layer of connective tissue.2,3
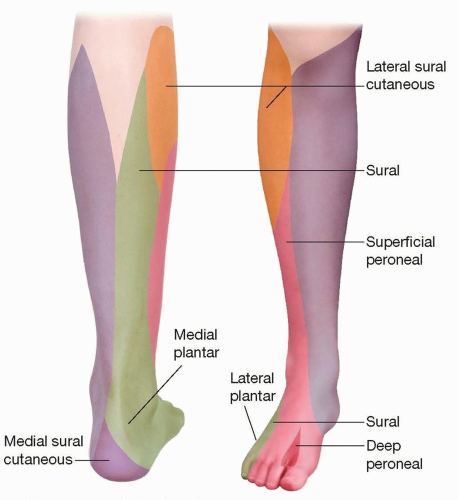
FIG 1 • Sensory distribution of the leg.
Within the popliteal fossa, the branches of the sciatic nerve usually lie lateral and posterior to the popliteal vessels. More proximally, the nerve can be found between the biceps femoris, and semitendinosus and semimembranosus tendons.
2 to 10 cm proximal to the popliteal fossa crease, the sciatic nerve bifurcates into the tibial and common peroneal nerves. The common peroneal nerve then travels laterally around the head and neck of the fibula, whereas the large tibial nerve continues caudally with the popliteal vessels.
PATIENT HISTORY AND PHYSICAL FINDINGS
Assess patient’s pain history and proposed surgery to determine if a popliteal nerve block is appropriate for the procedure.
Examine patient for preexisting neuropathy and weakness.
Assess for contraindications or increased risk of complications with regional anesthesia:
Patient refusal
Allergy to local anesthetic
Infection at site of nerve block or systemic infection
Coagulopathy
Preexisting neuropathy
Increased risk of compartment syndrome
The patient’s surgeon and primary anesthesia team should agree with placement of block.
Determine if a single injection nerve block or perineural catheter is indicated depending on the requirements for surgical anesthesia and postoperative analgesia. If a prolonged block is preferred for outpatient surgery, ensure that the patient will be able to care for an insensate limb at home and can be contacted for follow-up.
Prior to starting the nerve block, ensure that the patient will be able to proceed with surgery and anesthesia (consents completed, appropriately NPO, etc.).
SURGICAL MANAGEMENT
Preoperative Planning
Patient preparation:
Surgical and anesthesia consents signed
Monitors—blood pressure cuff, ECG, pulse oximeter, capnography
Supplemental oxygen via nasal cannula or facemask
Pillows, blankets, or tables to aid positioning
Skin marker to mark the site laterality and surface landmarks
Sedation to optimize patient comfort—typically midazolam and fentanyl
Rescue drugs and emergency airway equipment available
Supplies for single injection technique:
Antiseptic skin disinfectant
Sterile gloves, mask, hat
Sterile drapes or towels
50- to 100-mm 20- to 22-gauge short-bevel insulated stimulating needle
Small syringe and small gauge needle with lidocaine for skin infiltration
30 mL local anesthetic of choice
Nerve stimulator and/or ultrasound machine with highfrequency linear probe, sterile ultrasound probe cover, and ultrasound gel
Supplies for continuous catheter technique:
Antiseptic skin disinfectant
Sterile gloves, gown, mask, hat
Ultrasound machine with high-frequency linear probe or nerve stimulator
30 mL local anesthetic of choice
Sterile regional anesthesia tray:
Drapes or towels
Gauze
A 100-mm block needle, often a 17- or 18-gauge Tuohy needle
A flexible nerve block catheter with connector (may use stimulating catheter with nerve stimulator technique)
10- to 20-mL syringe
Local anesthetic or saline for injection through needle
Extension tubing
Small syringe and small gauge needle with lidocaine for skin infiltration
Surgical skin glue
Transparent dressing
Catheter stabilization device
Ultrasound probe cover with ultrasound gel
Approach
Ultrasound-Guidance Versus Nerve Stimulation
Nerve localization can be achieved using peripheral nerve stimulators and/or ultrasound guidance.
Over the past decade, ultrasound-guided nerve blocks have rapidly gained popularity because they provide several advantages compared to the nerve stimulator technique. The use of ultrasound provides direct, real-time visualization of target nerves, needle advancement, and spread of local anesthetic in the desired location.6 With continuous catheter techniques, the precise location of the catheter tip can be visualized. Blood vessels and smaller peripheral nerves can be identified and avoided. Research suggests that ultrasound guidance provides an improvement in time required to perform the block, block onset, and block success.7,8,9,10
For the popliteal sciatic block, ultrasound allows visualization of the precise point where the sciatic nerve bifurcates, which is variable between patients. Identifying this location is helpful in blocking both components of the sciatic nerve.
For these reasons, although this chapter briefly covers nerve stimulator approaches, the focus will be on ultrasound-guided techniques, which have become routinely used in regional anesthesia.

FIG 2 • In-plane approach to popliteal sciatic nerve block.
Ultrasound in-plane versus out-of-plane needle insertion approaches
With the in-plane approach, the needle is inserted at the side of the transducer, in line with the ultrasound beam (FIG 2). Because the needle is within the plane of imaging, the entire needle shaft and tip should be seen as echogenic line. In-plane approach is often used due to superior visualization of the entire needle as it is advanced toward the target.
With the out-of-plane approach, the needle is introduced perpendicular to the transducer (FIG 3). The needle crosses the plane of the ultrasound beam such that the needle shaft and tip are seen as an echogenic dot on ultrasound. Needle tip localization is more difficult with this approach. Techniques to help locate the needle tip include looking for tissue displacement, scanning for the needle tip, and injection of fluid to separate tissue planes (hydrodissection). One advantage of using the out-ofplane approach is that the needle traverses only skin and adipose tissue, avoiding muscle.
Approaches related to patient positioning
A wide range of positions can be used during popliteal sciatic nerve blockade. Each is discussed and illustrated in further detail in the following section.
Choice of positioning is typically dictated by a combination of patient comfort, patient mobility, operator ergonomics, and the operator’s personal preference. Body habitus, pain, or the presence of external fixation devices may limit the ability of the patient to assume a lateral or prone position.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree