Soft Tissue Coverage of Lower Leg—Soleus Flap
Rahim Nazerali
Lee L. Q. Pu
DEFINITION
Mathes and Nahai type II muscle
Most commonly proximally based pedicled flap, but a distally based flap has been reported.
ANATOMY
Broad, large, bipennate muscle
Deep to the gastrocnemius muscle in the posterior compartment of the leg
Occupies major portion of superficial posterior compartment of the leg in the middle third tibial level
Two separate muscle bellies, medial and lateral with separate origins
Origin
Lateral belly: posterior surface of the fibula
Medial belly: middle third of the medial border of the tibia
Insertion
Lateral belly: dorsal lateral aspect of the Achilles tendon
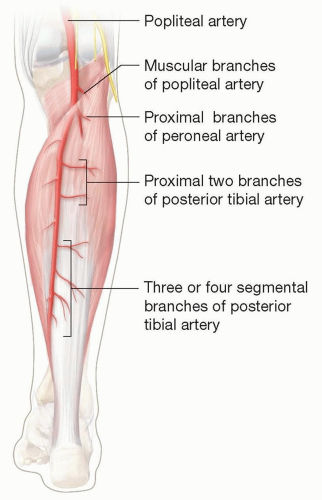
FIG 1 • A schematic diagram shows the vascular anatomy of a soleus muscle.
Medial belly: dorsal medial aspect of the Achilles tendon
Vascular supply (FIG 1)
Proximal portion of muscle receives independent axial vascular supply to its medial and lateral bellies.
Dominant pedicle: muscular branches of the popliteal artery and from proximal two branches of the posterior tibial artery and peroneal artery
Distal portion of muscle primarily receives segmental blood supply from two to four segmental branches from the posterior tibial artery.
Innervation
Motor: posterior tibial and medial popliteal nerves
Function
Plantar flexion
PATIENT HISTORY AND PHYSICAL FINDINGS
Just like any other major flap surgery for the lower extremity, a patient’s general medical condition and neurovascular physical examination should be evaluated carefully.
Previous orthopedic trauma to the leg and ongoing orthopedic procedures should also be taken into a consideration when planning a soleus muscle flap.
IMAGING
Preoperative angiogram is recommended if using a distally based medial hemisoleus muscle flap to assess the blood supply, which is typically from branches of the posterior tibial vessels.
Soleus is the standard muscle flap of choice for middle third defects of the leg.
Numerous limitations with bulk, arc of rotation and weakening of plantar flexion when using the entire muscle.
Medial hemisoleus muscle flap can be elevated based either proximally or distally depending on the location of the soft tissue reconstruction required.
Medial hemisoleus muscle flaps should be chosen to reconstruct a less extensive wound (less than 50 cm2 in most adult patients).
Proximally based flaps can be used to cover middle third tibial wounds in the leg, whereas distally based flaps can be used for distal third defects. In addition, proximally based flaps can also be used to cover distal third defects if done properly.
Preoperative Planning
Positioning
Frog leg positioning
Approach
Elevate under tourniquet control.
Longitudinal skin incision made 2 cm medial to the medial border of the tibia and parallel to the tibia.
Only the muscular portion of the soleus muscle is used as the flap, whereas the tendon portion of the flap is left intact.
To cover a wound at:
Middle and distal third of the leg: medial hemisoleus muscle flap is elevated to the level just below the junction between the proximal and middle third of the leg for a middle third defect or just above the junction between the middle and distal thirds of the leg so that an adjacent perforator from the posterior tibial vessels to the flap can be preserved (FIG 2A).
Distal third of the leg: medial hemisoleus muscle flap is elevated only to the level just below the junction between the middle and distal thirds of the leg, preserving as many major perforators to the flap as possible, even in the distal third of the leg while allowing adequate arc of flap rotation (FIG 2B).
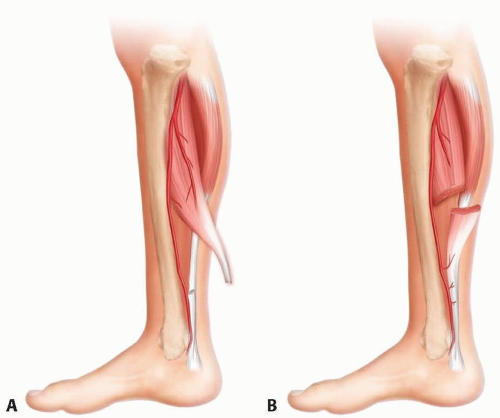 FIG 2 • A. Flap dissection and blood supply to the proximally based medial hemisoleus muscle flap. The flap receives its blood supply primarily from the posterior tibial vessels. The flap also receives additional blood supply from one or two perforators from the posterior tibial vessels to its distal portion. B. Flap dissection and blood supply to the distally based medial hemisoleus muscle flap. The flap receives its blood supply primarily from the most distal two perforators of the posterior tibial vessels. The flap also receives additional blood supply from the proximal source in a retrograde fashion.
Related posts: Fasciotomy of the Thigh, Lower Leg, and Foot Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts) Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction Tibial Reconstruction
 Reconstruction of Femur Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|