Pityriasis Rosea
Kevin Shih
Murad Alam
I. BACKGROUND
Pityriasis rosea (PR) is a mild self-limited eruption seen predominantly in adolescents and young adults during the spring and fall. A viral etiology for PR has often been suggested, although there has been inconsistent supporting laboratory evidence. A number of studies suggested a role for human herpesvirus 7 (HHV-7)1 while others have failed to find serologic or tissue-based evidence for HHV-7 in patients with PR.2 Other studies have implicated HHV-6 as a possible cause.3 Recently, HHV-6 and the influenza A (H1N1) viruses were found to have possible implications in the pathogenesis of PR.4 More studies are required before the etiology can be resolved.
PR may be asymptomatic, but many patients will experience pruritus, which at times can be severe. The onset of the eruption is sometimes coincident with mild malaise and symptoms similar to those of a viral upper respiratory tract infection or gastrointestinal symptoms (<20% of patients report some preceding viral symptoms).
II. CLINICAL PRESENTATION
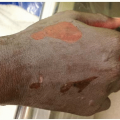
The initial lesion is frequently a 2- to 6-cm, round, erythematous, pink- to salmon-colored scaling patch or plaque, which may appear anywhere on the body but most commonly on the trunk (about 50%), more rarely on the limbs. The collarette of scale is described as “trailing,” with the free edge pointing inward (Fig. 33-1). This “herald patch” or “mother patch” is not present, or at least not noticed, in 20% to 30% of cases. The patch can enlarge progressively to reach a diameter of 3 cm or more. Within several days to 2 weeks, a more generalized eruption can develop consisting of small 1- to 2-cm pale, red, round to oval macular and papular lesions with a crinkly surface and a rim of fine scale which appear in crops on the trunk and proximal extremities (Fig. 33-2). Minute pustules may also be seen. The face, hands, and feet are usually spared, except in children. The long axes of the lesions are oriented in the planes of cleavage running parallel to the ribs and are classically said to form a Christmas tree-like pattern (Fig. 33-3). Lesions may be few or almost confluent, slowly enlarging by peripheral extension, and can continue to appear for 7 to 10 days. Oral lesions are unusual, but when present consist of red patches and plaques with hemorrhagic puncta or white erosions. Annular lesions have also been described in the mucosa.
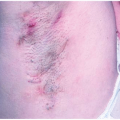
Variants of PR at times seem to appear as commonly as the classic disease. In children, the lesions are often papular, and purpuric lesions have also been described. Vesicular and bullous lesions may be seen, often with involvement of the palms and soles. Occasionally, eruptions may be limited to a small area or confined only to skin folds, which is known as inverse PR. Urticarial, intensely inflammatory, and very symptomatic lesions are possible. The herald patch may be absent, not noticed, or the only manifestation of the disease. In patients
with Fitzpatrick skin types IV and V, individual lesions may have more of a lichenoid appearance and may show more depigmentation. The distribution may be atypical, often including the face. Either hyper- or hypopigmentation may persist after the initial eruption has resolved.
with Fitzpatrick skin types IV and V, individual lesions may have more of a lichenoid appearance and may show more depigmentation. The distribution may be atypical, often including the face. Either hyper- or hypopigmentation may persist after the initial eruption has resolved.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


