Introduction
Since early 2000, there has been a dramatic increase in the number of publications and clinical trials devoted to moderate to severe hidradenitis suppurativa (HS). HS is a complex disease process in which a complete mechanism is still unknown. Recent data on pathogenesis are presented in earlier chapters, and a currently proposed model is presented in Fig. 34.1 . Drugs currently in the therapeutic pipeline target a broad range of inflammatory pathways that may be important in the pathogenesis of HS.
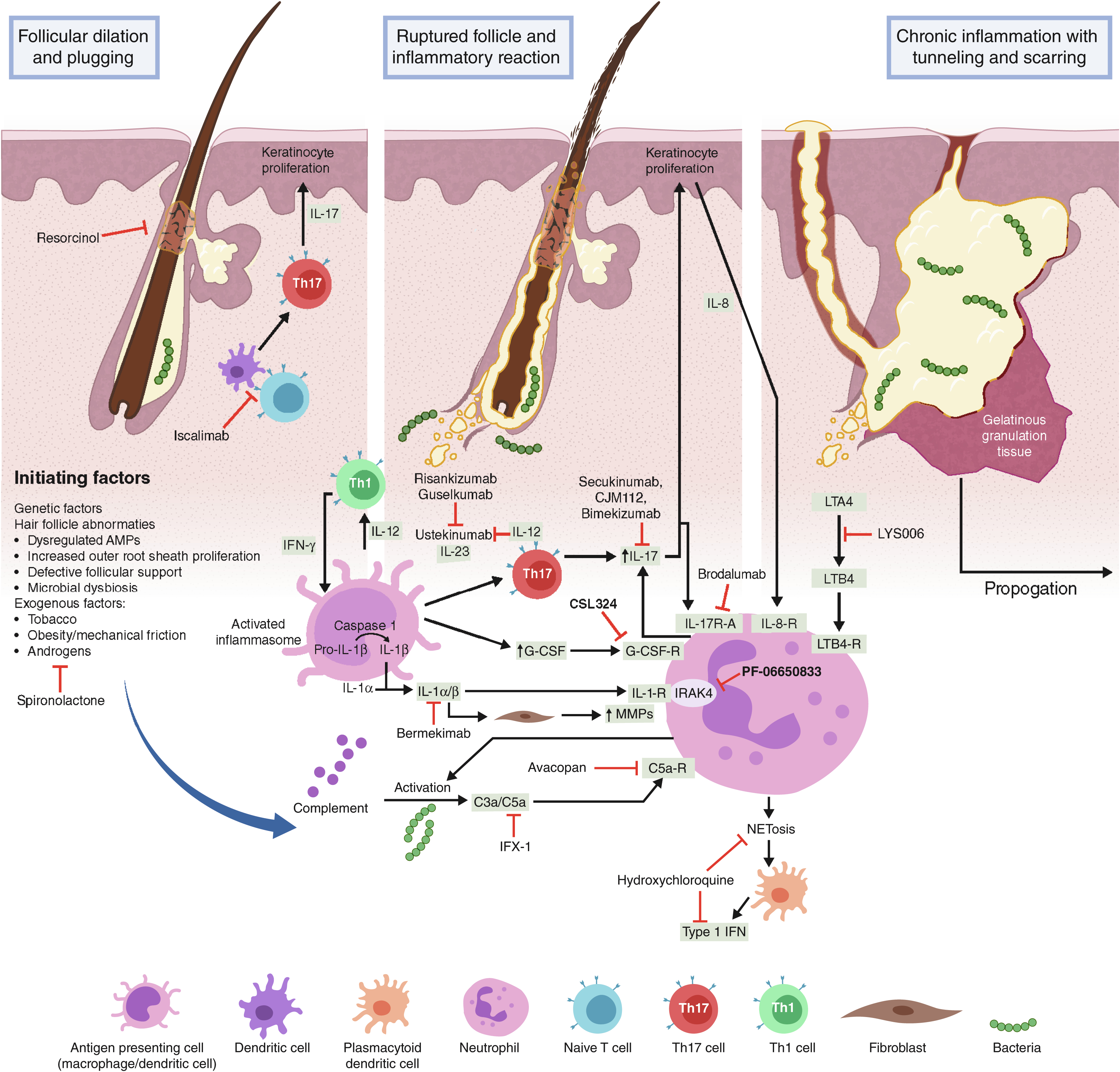
This chapter summarizes the drugs, procedures, and complementary and alternative medicine (CAM) modalities currently in clinical trials for HS. Outcome measures for HS clinical trials have been presented in Chapter 13 . Table 34.1 lists drug trials for HS registered at www.clinicaltrials.gov as of January 1, 2020, which are active, recruiting, not yet recruiting, or recently completed but results are unpublished. Potential therapeutic targets currently being studied in drug clinical trials include neutrophils, the complement pathway, inflammatory cytokine signaling pathways such as interleukin (IL)-17, IL-23, and IL-1α/β, as well as the Janus kinase (JAK)-signal transducer and activator of transcription (STAT) signaling pathway. Fig. 34.1 illustrates where these agents may act in the pathogenic pathway of HS. Surgical, procedural, CAM treatments, and wound care approaches currently under investigation and registered as of the same date are listed in Table 34.2 .
| Sections | Drug name | Target(s) | Structure | Sponsor | Trial number | Phase | Status |
|---|---|---|---|---|---|---|---|
| Complement/Neutrophils | CSL324 | G-CSF receptor | Monoclonal antibody | CSL Behring | NCT03972280 | I | Recruiting |
| LYS006 | LTA4 hydrolase | Small molecule | Novaritis Pharmaceuticals | NCT03827798 | II | Recruiting | |
| IFX-1 | C5a | Monoclonal antibody | InflaRx GmbH | NCT03487276 | II | Completed | |
| Avacopan | C5a receptor | Small molecule | ChemoCentryx | NCT03852472 | II | Recruiting | |
| TNF-α | Adalimumab | TNF-α | Monoclonal antibody | Wake Forest University Health Sciences | NCT04132388 | IV | Not yet recruiting |
| IL-17 | Secukinumab | IL-17A | Monoclonal antibody | Novartis Pharmaceuticals | NCT03713632 NCT03713619 NCT04179175 | III III III | Recruiting Recruiting Recruiting |
| CJM112 | IL-17A/F | Monoclonal antibody | Novartis Pharmaceuticals | NCT02421172 | II | Completed | |
| Bimekizumab (vs adalimumab/placebo) | IL-17A/F | Monoclonal antibody | UCB Biopharma | NCT03248531 | II | Completed | |
| Brodalumab | IL-17 receptor A | Monoclonal antibody | Florida Academic Dermatology Centers | NCT03910803 | II | Not yet recruiting | |
| IL-23 | Risankizumab | IL-23p19 | Monoclonal antibody | AbbVie | NCT03926169 | II | Recruiting |
| Guselkumab | IL-23p19 | Monoclonal antibody | Rockefeller University University Medical Center Groningen Janssen Research & Development | NCT04084665 NCT04061395 NCT03628924 | I II II | Not yet recruiting Not yet recruiting Active, not recruiting | |
| IL-1 | Bermekimab (MABp1) | IL-1α | Monoclonal antibody | XBiotech, Inc. | NCT04019041 | II | Recruiting |
| PF-06650833 | IRAK4 | Small molecule | Pfizer | NCT04092452 | II | Recruiting | |
| JAK/STAT | PF-06700841 | JAK1/TYK2 | Small molecule | Pfizer | NCT04092452 | II | Recruiting |
| PF-06826647 | TYK2 | Small molecule | Pfizer | NCT04092452 | II | Recruiting | |
| INCB054707 | JAK1 | Small molecule | Incyte Corporation | NCT03569371 NCT03607487 | II II | Completed Recruiting | |
| Other Medications | Hydroxychloroquine | Multiple | Quinolone | University of Pittsburgh | NCT03275870 | I/II | Completed |
| Spironolactone | Androgens | Steroid | Medical University of South Carolina | NCT04100083 | IV | Not yet recruiting | |
| Iscalimab (CFZ533) | CD40 | Monoclonal antibody | Novartis Pharmaceuticals | NCT03827798 | II | Recruiting | |
| 15% Topical Resorcinol | Keratin | Benzenediol FIZEVI | FIZEVI, Fundación Pública Andaluza para la gestión de la Investigación en Sevilla; | NCT04099212 | II | Recruiting |
| Sections | Drug name | Sponsor | Trial number | Status |
|---|---|---|---|---|
| Surgery/Procedures | Sclerotherapy | Beth Israel Deaconess Medical Center | NCT02805595 | Recruiting |
| Alexandrite Laser | Wayne State University | NCT03054155 | Recruiting | |
| Radiotherapy | Montefiore Medical Center | NCT03040804 | Recruiting | |
| Adalimumab Peri-surgically (SHARPS) | Abbvie | NCT02808975 | Completed | |
| Adalimumab vs. Adalimumab/Surgery | Erasmus Medical Center | NCT03221621 | Recruiting | |
| Axillary Perforator Flap vs. Secondary Intention Wound Healing | Assistance Publique – Hôpitaux de Paris | NCT03784313 | Not yet recruiting | |
| Negative pressure therapy | Royal Free Hospital NHS Foundation Trust | NCT04325607 | Recruiting | |
| Wound Care | Methylene blue, gentian violet, and bovine forestomach | Wake Forest University Health Sciences | NCT04354012 | Not yet recruiting |
| Multiple Cutimed® dressings | University of Miami | NCT04194541 | Recruiting | |
| CAM | Cannabis oil | TO Pharmaceuticals | NCT03929835 | Not yet recruiting |
| Battlefield Acupuncture | Wayne State University | NCT04218422 | Recruiting |
Neutrophils and Complement
Hair follicle content exposed to the dermis, due to follicular occlusion and subsequent rupture, provokes a robust neutrophilic infiltration via inflammatory cytokines (e.g., IL-8), lipid signaling (e.g., leukotriene B4 [LTB4]), and complement activation (e.g., C3a, C5a). These chemoattractants, as well as others, bind to over 30 chemokine, selectin, and integrin receptors on the neutrophil’s surface. Neutrophils have been implicated in the pathogenesis of HS due to the large number of neutrophils seen in early lesions and several case reports and series suggesting efficacy for anti-neutrophil agents, such as dapsone and colchicine, in HS.
Primed neutrophils produce reactive oxygen species (ROS); secrete granules containing antimicrobial peptides (AMPs), alarmins, and proteases; and release neutrophil extracellular traps (NETs). These result in tissue damage as well as recruitment and activation of macrophages, that produce pro-inflammatory cytokines, such as IL-1α/β, TNF-α, and granulocyte-colony stimulating factor (G-CSF), recruiting more neutrophils. In vitro, stimulated neutrophils from HS patients secrete higher levels of ROS compared to healthy controls and produce NETs, even without stimulation. In HS lesional tissue, NETs have been detected that correlate with disease activity.
Currently, researchers are investigating two novel drugs that target neutrophil recruitment in HS. CSL324 is a fully human G-CSF receptor monoclonal antibody. The G-CSF receptor signals via the JAK1/STAT3 signaling pathway. It regulates mobilization of neutrophils from the bone marrow into the peripheral circulation as well as neutrophil recruitment to tissues via changes to cellular adhesion and chemokine receptors on the neutrophil surface. In animal models, G-CSF receptor inhibition reduces neutrophilic inflammation without causing neutropenia or reducing neutrophil function. CSL324 is currently in its first-in-human study, a phase I, open-label, two-dose regimen trial in patients with HS and palmoplantar pustulosis.
LYS006, an inhibitor of LTA4 hydrolase, is currently being studied for acne, Crohn’s disease, and non-alcoholic fatty liver disease (NAFLD), in addition to HS. LTA4 hydrolase catalyzes the rate-limiting step in converting LTA4 into LTB4, a potent neutrophil chemotactic agent. LTB4 has been shown to be critical for the recruitment and clustering of neutrophils into localized collections (abscess). LTB4 and LTB4-induced pathways in HS have been found to be increased in lesional skin, suggesting that this lipid pathway could be an important target for HS treatment. A three-arm randomized controlled trial studying LYS006 vs. iscalimab (CFZ533, anti-CD40) vs. placebo is presently recruiting.
Activated neutrophils are able to initiate the complement alternative pathway on their cell surfaces. Anaerobic bacteria, such as Porphyromonas spp. can also cleave and activate complement. The resulting complement fragments, including C3a and C5a, are strong chemoattractants for both neutrophils and macrophages. C5a has also been shown to induce NET release in activated neutrophils and prime monocytes to produce TNF-α and IL-6. In HS, the complement pathway may be an important contributor to the heightened neutrophilic inflammatory response. With increased levels of C5a found in both tissue and plasma of HS patients, C5a and its receptor have become therapeutic targets for HS treatment.
IFX-1 is a monoclonal IgG4 kappa antibody against human C5a. Selective C5a inhibition leaves the membrane attack complex (MAC) intact, minimizing immunosuppression, especially for encapsulated organisms. An early open-label study of IFX-1 indicated an 83% treatment response rate after three months in patients with severe HS. A phase IIb clinical trial for IFX-1 in HS patients was recently completed and the results were released in two press releases. Unfortunately, IFX-1 failed to meet its primary end point (a statistically significant dose-dependent improvement in HS Clinical Response [HiSCR] over placebo), although there was a significant improvement in the DLQI. Secondary endpoint and post-hoc analysis demonstrated significant reductions in draining fistulas and IHS4 score in the high-dose IFX-1 group compared to controls. The company has indicated that it plans to continue to develop IFX-1 as a treatment for HS, and an open-label extension study is continuing. Avacopan, an orally available small-molecule C5a receptor antagonist with demonstrated efficacy in ANCA-associated vasculitis, is now undergoing a Phase II clinical trial in moderate to severe HS patients.
Cytokines
There are numerous cytokines that have been implicated in the pathogenesis of HS. To date, the inhibition of TNF-α has been the mainstay of medical treatment. Currently, the only United States Federal Drug Administration (FDA) approved medication for HS is adalimumab, a fully human, IgG1 monoclonal antibody targeting TNF-α. Unfortunately, only 40% to 60% of patients achieve HiSCR, and of those that achieve HiSCR, some lose their response over time. Data from studies on inflammatory bowel disease suggest that secondary loss of response is either due to mechanistic failure or low drug concentrations, with or without the development of anti-drug antibodies. Poor adherence to therapy has been associated with secondary loss of response due to low drug concentrations and increased immunogenicity. A phase IV randomized trial is planning to evaluate the practical administration of adalimumab for HS, specifically whether a novel electronic medication monitoring device compared with usual care can improve clinical outcomes and adherence compared with usual care. In addition to issues related to adherence and loss of response to TNF-α inhibitors, many patients are not able to tolerate or never respond to TNF-α inhibition initially. Thus, researchers have started investigating new cytokine targets, such as interleukin (IL)-17, IL-23, and IL-1α/β. The following section highlights each cytokine, its association with HS, and preliminary results from clinical studies. Clinical trials data of adalimumab are further discussed in Chapter 18 .
IL-17
The family of interleukin-17 (IL-17) cytokines (IL-17A-F) signal through multiple IL-17 receptors formed from six unique IL-17 receptor subunits that exist as homodimers or heterodimers. While not critical for differentiation, IL-23 plays an important role in sustaining T H 17 differentiation and promoting IL-17 and IL-22 production. In addition, IL-17A and IL-17F act synergistically with IL-1 and TNF-α to augment and perpetuate the inflammatory cascade triggered by these pro-inflammatory cytokines. IL-17A activates keratinocyte proliferation and produces AMPs and numerous neutrophil-attracting chemokines, including IL-8 (also referred to as CXCL8). IL-17F has similar functions biologically as IL-17A, signaling through the same receptor and forming a heterodimeric complex with IL-17A. Multiple studies have demonstrated significantly increased IL-17 levels in HS lesions and perilesional tissue, compared to control skin. 29 The elevated levels of IL-17 in perilesional tissue may suggest an early role in HS pathogenesis. In addition, IL-17 has also been found to be elevated in the serum of HS patients, which correlates with disease activity.
Secukinumab is a human IgG1 monoclonal antibody that binds IL-17A, preventing its interaction with the IL-17 receptor. Initially, several case reports were published demonstrating benefit to HS patients. However, an in vitro study using HS skin lesions showed that secukinumab did not significantly lower overall cytokine (TNF-α, IFN-γ, IL-1β, IL-6, and IL-17A) levels compared with prednisolone, TNF-α inhibitors, or ustekinumab. More recently, there has been increased enthusiasm for this approach after three open-label 16- to 24-week prospective studies for moderate to severe HS demonstrated benefit, with 67% to 75% achieving HiSCR. Two core phase III multicenter, randomized, double-blinded placebo-controlled studies with two secukinumab dose regimens (300 mg every 2 or 4 weeks) are currently underway for moderate to severe HS. A randomized withdrawal extension study for the two core trials is already recruiting. The goal of the study is to assess the long-term maintenance of HiSCR out to week 104. Those participants that achieve HiSCR by week 52 of the two core studies will be randomized (2:1) to continue their regimen or placebo until week 104 to evaluate the loss of response. Those participants that either did not achieve HiSCR by week 52 in the core studies or lose response in the extension trial or complete the 104-week extension trial maintaining HiSCR will be offered to enroll in the open-label treatment study to week 260.
CJM112 is a fully human IgG1 monoclonal dual anti-IL-17A and anti-IL-17F antibody. It has higher potency compared with secukinumab, achieving similar results for psoriasis, but at significantly lower doses. In addition, in vitro studies have demonstrated that dual IL-17A/F inhibition significantly lowers inflammatory mediators more than either IL-17A or IL-17-F alone. Recently, a phase II randomized placebo-controlled trial for HS showed 32% (10/32) participants had a two-point drop in HS physician global assessment (HS-PGA) score, compared to only 12.5% (4/32) in the placebo group.
Bimekizumab is also a human IgG1 monoclonal dual anti-IL-17A/F antibody. Phase II proof-of-concept and dose-ranging studies have already shown significant improvements in both plaque psoriasis and psoriatic arthritis at higher doses compared to controls. A phase II randomized, double blind trial comparing two different doses of bimekizumab against adalimumab and placebo was recently completed. Results from this study have not been released, but two phase III randomized, placebo-controlled trials are currently being planned.
Brodalumab is a human monoclonal IgG2 antibody that binds with high affinity to the IL-17 receptor A, competitively inhibiting IL-17A, C, E, and F. As the responses to direct IL-17A inhibition with secukinumab can take up to 12 to 24 weeks for HS, the faster response rates seen for brodalumab in psoriasis makes it an attractive potential treatment for HS. Initially, a case report of brodalumab for HS showed rapid improvement in draining tunnels, global assessment, and quality of life over 12 weeks. More recently, results from an open-label early Phase I study of 10 participants with moderate to severe HS showed that using the FDA-approved dose for psoriasis resulted in all 10 participants achieving HiSCR by 12 weeks. Although there is a black box warning for suicidal ideation and behavior for brodalumab, no episodes of self-harm or suicidality were experienced by HS patients in this small study.
IL-12/23
Interleukin-12 (IL-12) and interleukin-23 (IL-23) are cytokines secreted by macrophages and dendritic cells in response to wound healing and infection. While IL-12 promotes T H 1 cell differentiation of naïve CD4 T cells, IL-23 contributes to the IL-17 producing T helper (T H 17) cell response. Both cytokines are highly expressed by infiltrating macrophages in lesional HS skin, and share a p40 subunit. IL-12 is a heterodimer composed of the IL-12p40 and IL-12p35 subunits which signal through the IL-12 receptor. IL-23 is a heterodimer composed of the IL-12p40 and IL-23p19 subunits that bind to the IL-23 receptor and signal through the JAK/STAT pathway. IL-23 has become a therapeutic target for both HS, psoriasis, and Crohn’s disease, three conditions with mechanistic as well as clinical overlap. Ustekinumab, an IL-12/23 inhibitor, has been FDA approved for the treatment of Crohn’s disease, while the data supporting its use in HS are less substantial. Ustekinumab has been shown to inhibit HS-related cytokine production in vitro. In addition to several case reports and case series suggesting benefit, moderate-to-marked improvements of the modified Sartorius score were seen in 82% of patients in a small open-label study of ustekinumab in 17 HS patients. More recent case series have suggested more frequent and higher doses of ustekinumab, with an initial intravenous infusion, may be of added benefit.
Recently, rizankizumab, a high-affinity monoclonal antibody to the p19 subunit of IL-23, demonstrated significantly increased rates of clinical remission of Crohn’s disease compared to placebo. They used doses of 600 mg intravenous infusion monthly, much higher than the FDA-approved dosing for psoriasis. Now there is increased interest in IL-23 specific antibodies for the treatment of HS. Currently, a phase II multicenter randomized double blinded placebo-controlled study is underway, evaluating the efficacy of rizankizumab at two dose levels for moderate to severe HS.
A similarly designed trial for HS is also starting for another IL23 p19 monoclonal antibody, guselkumab, at doses of 200 mg subcutaneously every 4 weeks, more than double the FDA-approved psoriasis dosing. One case report and a small case series of eight patients receiving guselkumab suggested benefit, with ~ 60% of patients demonstrating improvement over 2–4 months with typical psoriasis doses.
IL-1α/β
IL-1α and IL-1β contribute to the initiation of an immune response through a shared IL-1 receptor (IL-1R). IL-1R-associated kinase 4 (IRAK4) gets recruited to the internal domain of the IL1-R, resulting in downstream activation of pro-inflammatory transcription factors such as nuclear factor-kappa B (NF-κB). This results in the production of inflammatory mediators (i.e., IL-6), potent neutrophil chemoattractants (including G-CSF and IL-8), and MMPs. In addition, IL-1 receptor signaling results in increased production of both IL-1α and IL-1β, resulting in a positive feedback loop. IL-1α is constitutively expressed and actively secreted by many cells, most notably, myeloid cells, endothelial cells, and keratinocytes. Moreover, IL-1α can activate its receptor while membrane-bound or through apoptotic bodies released after cell damage or death. Release of IL-1β from macrophages and dendritic cells; on the other hand, is mediated by caspase-1, which, in its inactive form, is a component of the NOD-, LRR-, and pyrin domain-containing protein 3 (NLRP3) inflammasome. In order to be activated, the IL-1β precursor must be cleaved by caspase-1. The IL-1 receptor signaling cross-talks with various inflammation pathways, including interactions with Th17 and type I interferon signaling. IL-1α and IL-1β act synergistically with IL-23 on T cells to produce IL-17. Type I interferons antagonize IL-1 signaling via suppression of IL-1α and IL-1β transcription, as well as several indirect mechanisms.
The role of IL-1—especially IL-1α—has become of increasing interest recently in the pathogenesis of HS. While some conflicting data exist, several studies have demonstrated overexpression of IL-1β in lesional and perilesional HS skin compared to controls. Similarly, elevated levels of IL-1α and IL-1β have been seen in pus from HS lesions. Increased serum levels of IL-1β in HS patients have also been reported.
Anakinra, a competitive antagonist of the shared IL-1 receptor, has demonstrated efficacy in case reports, case series, and a small randomized, placebo-controlled trial of 20 patients with severe HS. Retrospective analysis of this trial revealed 78% of anakinra patients versus 30% of placebo patients achieved HiSCR at 12 weeks. Currently, anakinra is recommended as third-line treatment consideration after failed response to TNF-α inhibitors. While anakinra has demonstrated some benefit in HS, canakinumab, a monoclonal antibody specifically targeting IL-1β, has had much more conflicting data.
Current clinical trials targeting IL-1 include bermekimab (previously known as MABp1), an anti-IL-1α monoclonal antibody which has shown promising results for HS. In a randomized placebo-controlled small study of 20 patients with moderate HS refractory to TNF-α inhibition, 60% of HS patients achieved HiSCR compared to only 10% in the placebo group. Similar responses were seen in a larger, multicenter, phase II open-label study of 42 patients with HS, with ~ 60 achieving HiSCR, with no difference between those that had failed TNF-α and those that were TNF-α inhibitor naïve. It has been proposed that its efficacy may be linked to its roles in both angiogenesis, as well as upregulation of human beta-defensin 2. A phase II clinical trial with bermekimab is currently ongoing.
PF-06650833, a small molecule inhibiting IL-1 receptor-associated kinase 4 (IRAK4), is also currently being investigated as a target for HS. Presently, a phase II, double-blind, randomized, placebo-controlled clinical trial is examining the efficacy and safety of PF-06650833 in moderate to severe HS alongside two other JAK family inhibitors.
JAK-STAT Signaling Pathway
The JAK/STAT signaling pathway is activated by numerous ligands, including cytokines and hormones, that are responsible for a large number of cellular functions in various cell types. In humans, there are four JAK family members identified (JAK1-3 and Tyrosine Kinase 2 [TYK2]), which associate with several different receptors and are also found in many different cell types. Each pathway can activate one or more STAT family members (STAT1-4, STAT5A, STAT5B, and STAT6). Disruption of the JAK/STAT signaling pathway interferes with T H 1/2/17 differentiation, T- and B-cell function, as well as granulopoiesis and neutrophil release and chemotaxis, depending on which of the specific JAK/STAT receptor complexes are inhibited.
JAK inhibitors have become of interest for HS due to the role that type I and II cytokines are thought to play in HS, as well as their indirect inhibition of IL-1β production and TNF-α signaling. Recently, two severe Hurley stage III patients that had failed multiple biologics treatments were reported to have responded to adjunct tofacitib (JAK 1/2/3 inhibitor) 5 mg twice a day in addition to antibiotics and various immunosuppressive agents. Due to cytokine profiles important for the various JAK family members ( Table 34.3 ), JAK1 and TYK2 are the most intriguing due to the current proposed HS pathogenesis.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


