Introduction
Topical therapy is a mainstay of dermatological treatment and holds many advantages, including ease of use, relative lack of systemic side effects, and patient-directed application. In hidradenitis suppurativa (HS), topical therapeutics are often used for early-stage lesions or as a complement to systemic or surgical treatments. The four categories of disease-modifying topical therapy for HS are antibiotics, antiseptics, keratolytics, and bathing additives (each of which will be discussed in this chapter), while symptom-control therapies such as topical analgesia and antipruritics are reviewed in Chapter 19. Some complementary and alternative therapies are also thought to be helpful when applied topically, and these will be briefly reviewed as well.
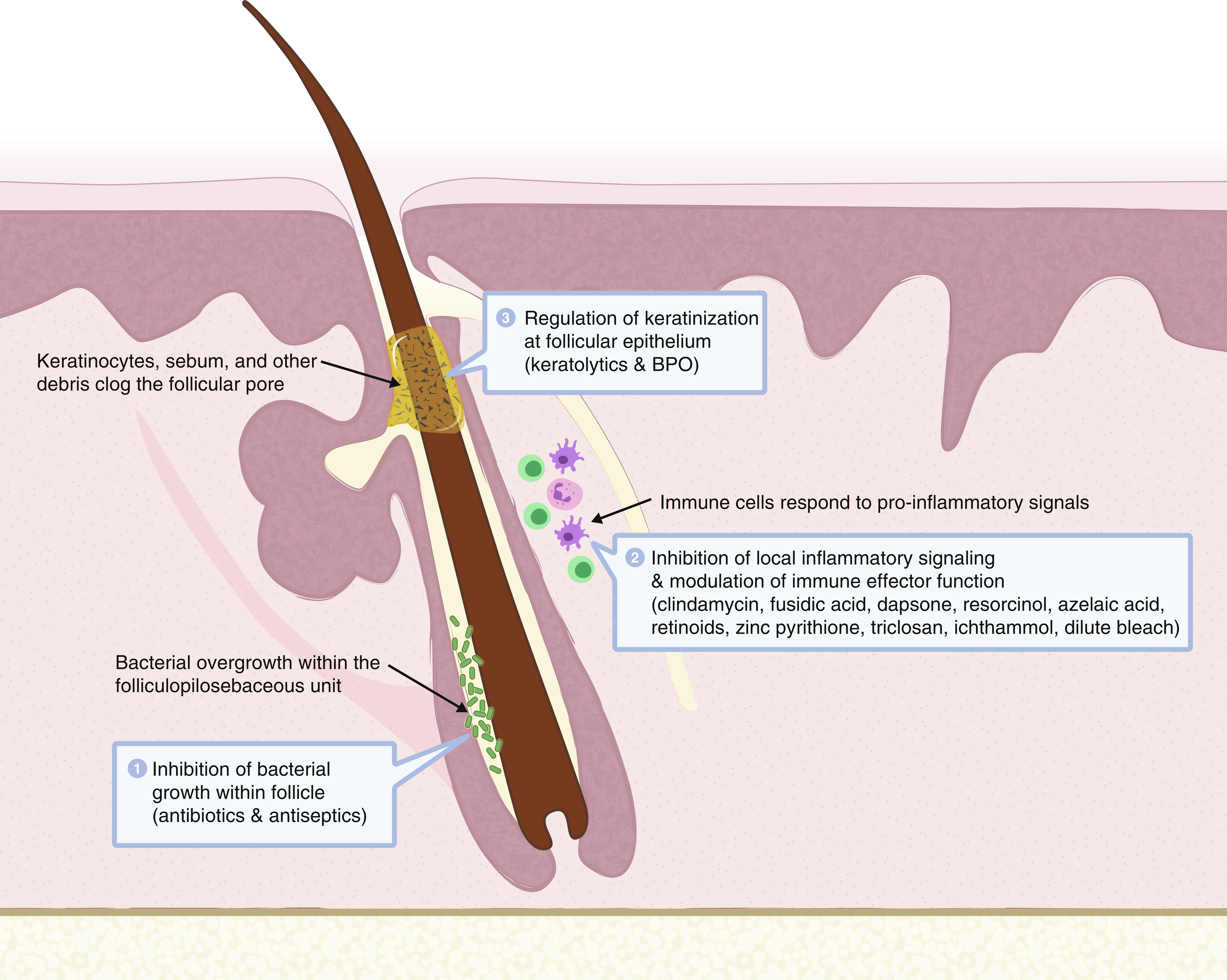
Unfortunately, the level of evidence supporting the use of most topical therapies in HS is low ( Table 15.1 ). This chapter will provide an overview of dosing schedules, drug mechanisms of action ( Fig. 15.1 ), and contraindications of topical therapeutics for HS to better inform these decisions.
| Topical Antibiotics | ||||||
|---|---|---|---|---|---|---|
| Therapy Name | Mechanism of Action | Dosing | Contraindications | Adverse Effects | Level of Evidence a | Notes on Use |
| Clindamycin | Inhibit bacterial ribosome, inhibit PMN chemotaxis, inhibit biofilm formation, potentiate phagocytosis of bacteria | BID Limit monotherapy to 3 months | Hypersensitivity to clindamycin or lincomycin derivatives, history of regional enteritis or ulcerative colitis, history of antibiotic-associated colitis | Pruritis, xeroderma, erythema, burning, exfoliation, oily skin, bacterial resistance | B | Strongly consider in all mild HS patients and as adjunct therapy in moderate to severe cases. Safe for pregnant patients. |
| Fusidic Acid | Bind to elongation factor-G on bacterial ribosome inhibiting translation, suppress cytokine signaling | TID | Hypersensitivity to therapeutic vehicle or FA itself | Mild irritant or allergic contact dermatitis, bacterial resistance | B | Consider for Hurley stage 1 and early lesions. Avoid prolonged monotherapy as bacterial resistance is common. |
| Dapsone | Halt bacterial folate metabolism, reduce oxidative damage to tissue | BID | Hypersensitivity to therapeutic vehicle or dapsone itself | Methemoglobinemia, mild irritant or allergic contact dermatitis, bacterial resistance | D | Consider for Hurley I and early lesions or as adjunct therapy in later stages for patients who cannot use topical clindamycin. |
| Gentamicin | Inhibit bacterial ribosome | TID following surgery | Hypersensitivity to therapeutic vehicle or gentamicin itself | Mild irritant or allergic contact dermatitis, bacterial resistance | E | Use after de-roofing or local excision procedures. Consider for a secondarily infected HS lesion that grows gram negative species. |
| Topical Keratolytics | ||||||
| Resorcinol | Cytotoxic, modulate cytokine/chemokine release | BID with increasing concentration to therapeutic level (typically 15%–20%) | Concomitant use of intense pulsed light therapy, hypersensitivity to therapeutic vehicle or resorcinol itself | Desquamation, depigmentation, mild irritation, or allergic contact dermatitis | B | Use for acute lesions and to maintain quiescence. Check baseline pregnancy test. Not for use in women actively trying to get pregnant. |
| Azelaic Acid | Modulate keratinocyte proliferation | BID | Hypersensitivity to therapeutic vehicle or azelaic acid itself | Photosensitivity, desquamation, depigmentation, mild irritant or allergic contact dermatitis | E | Consider in children given low risk profile. |
| Bathing Additives and Complementary Therapies | ||||||
| Bleach baths | Creation of superoxide radicals, modulate NF-κB signaling | 2–3 times weekly | None | Caustic effects, bleaching of hair and fabrics | E | Consider in combination with other topical therapies for mild disease. |
| Magnesium Sulfate | Unknown | PRN | None known | Unknown | E | Not enough evidence to make a definitive conclusion. |
| CBD oil | Decrease pain perception, inhibit keratinocyte proliferation while regulating cellular differentiation and promoting apoptosis of both keratinocytes and sebocytes | PRN | None known | Unknown | E | Not enough evidence to make a definitive conclusion. |
| Turmeric | Disrupt bacterial membranes, inhibit bacterial replication, disrupt microbial biofilms | PRN | None known | Unknown | E | Not enough evidence to make a definitive conclusion. |
Antibiotics
The occlusion of the folliculopilosebaceous unit that heralds the onset of HS is followed by bacterial growth, inducing inflammation that leads to abscesses, sinus tracts, and destruction of adnexal structures. Given that bacteria are thought to contribute to the development and perpetuation of these lesions, it is no surprise that antibiotic therapy can be a useful approach to treatment. Topical antibiotics are postulated to work by two complementary methods in the treatment of HS: the reduction of bacterial burden and the prevention of inflammation. Their antibacterial effects decrease bacterial colonization, which then tempers the local inflammation associated with the body’s response to the resident bacteria. A number of topical antibiotics also have antiinflammatory effects independent of their antibacterial properties, and many are also delivered in vehicles that themselves may soothe inflamed skin via emollient, cooling, hydrating, or barrier-forming properties. In this section, various topical antibiotics that have been used in the treatment of HS will be discussed.
Clindamycin
Clindamycin is a broad-spectrum antibiotic of the lincosamide class that interferes with the synthesis of bacterial proteins by binding to the 50S ribosomal subunit, providing a bacteriostatic effect with concentration-dependent bactericidal activity against staphylococci, streptococci, and some anaerobes. It also boasts independent immunomodulatory effects. Though the mechanism of these additional properties is poorly understood, studies have postulated that clindamycin may inhibit complement-derived chemotaxis of polymorphonuclear leukocytes, potentiate the uptake of microorganisms by phagocytic cells of the innate immune system, and inhibit biofilm formation, thus assisting in the clearance of bacteria without drawing in additional inflammatory milieu. Given its localized effect, topical clindamycin is most effective for limited disease in the absence of deep abscesses and sinus tracts. Treatment has been shown to reduce pustules but has limited effect on abscesses and nodules. However, it can be used as an adjunct in more severe stages of HS along with the addition of systemic medications and surgical intervention.
Clindamycin is the only topical antibiotic treatment for HS to have been validated in randomized controlled trials. In these trials, topical clindamycin treatment was responsible for a significant reduction in the number of abscesses, inflammatory nodules, and pustules compared to the placebo, with effects equivalent to systemic tetracycline. Interestingly, the efficacy of clindamycin in one trial was independent of the presence of bacteria at the onset of treatment, as measured by culture of aseptic aspirate from inflamed HS lesions, indicating that the antiinflammatory properties of the drug may have played a major role.
Though HS treatment guidelines recommend various formulations of topical clindamycin such as solution, gel, or lotion, the original studies demonstrating efficacy were performed using clindamycin 1% solution. Availability, price, and patient preference are all considerations when choosing the most appropriate vehicle. Most consensus clinical guidelines recommend twice-daily application of topical clindamycin to areas affected by HS. However, use as monotherapy should not exceed 3 months, as studies have shown the emergence of resistant Staphylococcus aureus in the lesions of patients treated for prolonged periods. The addition of benzoyl peroxide (BPO) can mitigate the development of bacterial resistance and allow prolonged use.
Contraindications to the use of topical clindamycin either alone or in combination with other therapies are rare and limited to those with a history of hypersensitivity to preparations containing clindamycin or lincomycin derivatives, a history of regional enteritis or ulcerative colitis, or a history of antibiotic-associated colitis. Cutaneous adverse effects experienced by some patients include pruritis, xeroderma, erythema, burning, exfoliation, or oily skin.
Fusidic Acid
Fusidic acid (FA) inhibits the activity of the bacterial ribosome. FA binds to elongation factor G on the ribosome, preventing translocation of the bacterial ribosome. FA is most active against gram-positive bacteria, particularly Staphylococcus species (which are one of the most commonly found bacteria in HS wound cultures), and likely responsible for a significant amount of subsequent inflammation. Although biochemically comparable to many steroids, FA does not possess any steroid activity. There is excellent penetration of FA into deeper layers of the skin due to its lipophilic steroid-like structure and independent antiinflammatory activity due to suppression of cytokine signaling.
Evidence for FA utility in HS patients is limited to case reports and a single prospective cohort study. In this study involving 627 patients with Hurley stage 1 axillary HS, FA 2% ointment was applied thrice daily after washing with antibacterial soap. All patients had complete healing within 4 weeks of treatment. These data have, to our knowledge, not yet been replicated elsewhere.
FA for treatment of HS is typically formulated as a 2% sodium fusidate ointment or cream. Other formulations of FA are available and used for dermatologic conditions, such as combination formulations of FA with 1% hydrocortisone or 0.1% betamethasone, which can be used to treat eczema complicated by staphylococcal infection. While each of these formulations is available to those suffering from HS, further study of the relative efficacy of combined versus FA-only topicals is needed before a particular formulation can be recommended. There are significant concerns about the development of resistant bacteria with FA monotherapy, given that a single point mutation is enough to confer significant resistance and contribute to outbreaks of multi-drug-resistant bacteria. Prolonged monotherapy with FA is therefore generally avoided. Adverse events during treatment are uncommon and generally limited to reactions to components of the vehicle, which can lead to mild allergies or irritant contact dermatitis. Contraindications are limited to hypersensitivity to components of the topical therapeutic vehicle or FA itself.
Dapsone
Dapsone is an antibiotic with significant independent antiinflammatory activity commonly used for the treatment of a variety of dermatological conditions. The antibiotic activity of dapsone is mediated through the inhibition of dihydropteroate synthesis, halting folate metabolism and resulting in the stasis of bacterial growth. Its antiinflammatory activity is accomplished through inhibition of myeloperoxidase, an enzyme vital for oxidative destruction of microbes by neutrophils that often causes simultaneous damage to local tissues. Dapsone has also been postulated to inhibit neutrophil chemotaxis, a function that may serve to lessen inflammation in HS abscesses and sinus tracts. Limited evidence based on expert opinion suggests topical dapsone may be useful in early disease.
Commercially available topical dapsone for use in dermatological conditions is currently limited to gel form, with 5% and 7.5% formulations available. Initial dosing begins at twice-daily application, which is the recommended frequency for treatment of acne vulgaris. While concerns of antibiotic resistance would theoretically also apply to the use of topical dapsone, the literature currently suggests that monotherapy over periods up to 12 weeks does not lead to bacterial resistance. However, further study must be undertaken over longer periods to establish the safety of long-term dapsone monotherapy for conditions such as HS, which often requires more than 12 weeks of therapy.
While dapsone is structurally similar to sulfonamide drugs, allergy to sulfonamides is not a contraindication to its use. Although various dermatological side-effects of oral dapsone have been described, including severe reactions (such as toxic epidermal necrolysis), these effects have not been seen with topical dapsone. Unlike with the use of systemic dapsone, a glucose-6-phosphate dehydrogenase (G6PD) level does not need to be checked before commencing treatment with topical dapsone as there is no evidence of clinically relevant hemolysis or anemia after topical administration. Dapsone may also induce methemoglobinemia in the presence of other pharmaceuticals with similar propensities (such as local anesthetics), and this is true of both oral and topical dapsone.
Gentamicin
Gentamicin is an aminoglycoside antibiotic that inhibits the production of bacterial proteins by binding to ribosomal subunits, preventing the translation of messenger ribonucleic acid. Its broad spectrum of action makes it an attractive candidate for use in treating infected wounds. Thus far, study of topical gentamicin in HS has been limited to postoperative application as a strategy to reduce the rate of post-operative infection. While short-term complications, including dehiscence and infection, were mitigated by topical gentamicin use, the rate of recurrence of HS lesions was unaffected in the long term.
Gentamicin is available commercially as gentamicin sulfate 0.1% cream and ointment. Given the paucity of data and the lack of published success in treating HS lesions, guidelines tend to recommend that topical gentamicin be used only if other topical antibiotics are not available or cannot be used. Generally, topical gentamicin can be applied 3 to 4 times daily for treatment of superficial skin and soft tissue infections.
Contraindications are limited to hypersensitivity to product components, and adverse effects include skin irritation and the potential emergence of superinfection with atypical, resistant organisms. Given the varied bacterial milieu within HS wounds and the importance of bacterial control for mitigation of HS symptoms, such emergence should not be taken lightly.
Antiseptics
As opposed to the more narrowly targeted effects of antibiotic compounds, antiseptic washes are not absorbed into the body and have a broad spectrum of antimicrobial activity that relies on a variety of mechanisms to slow or stop microbial growth, resulting in reduced selective pressure and rare development of resistance. Antiseptic washes provide an additional method of minimizing bacterial colonization and reducing concomitant inflammation for HS patients, and are even more frequently utilized in some practices than topical antibiotics (though they are often used in tandem.) Given that lesions of HS are often polymicrobial on culture, antiseptic washes are theorized to be of similar utility to antibiotics without the risk of bacterial resistance or insufficient breadth of coverage that can accompany antibiotic use. However, such intervention comes with risk of both allergic and irritant contact dermatitis. There are few studies evaluating their effectiveness in preventing and treating HS flares. Patient adherence to using antiseptic washes has been reported to be low, with only 70% of patients using the recommended wash at all, and only 30% of those patients using it daily. Reported barriers to use included difficulty finding and affording the recommended wash with little perceived benefit. In this section, antiseptic washes commonly prescribed as treatment for early-stage HS will be discussed.
Chlorhexidine
Chlorhexidine is a cationic biguanide surfactant compound that destabilizes bacterial cell walls and membranes with residual activity lasting several hours after initial application. Commonly used as a disinfectant scrub prior to surgery or a mouthwash for gingivitis, it is also used topically by those with HS for this broad-spectrum antibacterial effect. Current evidence for utility of topical chlorhexidine is limited only to expert opinion.
Unfortunately, chlorhexidine has difficulty overcoming the biofilms that characterize many HS lesions, and is thus thought to be less able to affect the inflammation caused by secondary bacterial colonization. Patients should be counseled that chlorhexidine’s activity can be diminished through the concomitant use of incompatible products that include anionic surfactants commonly found in laundry detergents, handwashes, bodywashes, and household cleaners. Use of chlorhexidine on open wounds weeping purulent discharge, serum, or blood is also ineffective, as presence of excess phospholipids similarly blunts its antimicrobial activity. Chlorhexidine is available over the counter, and side effects include irritation and, more rarely, allergic contact dermatitis.
Benzoyl Peroxide
Use of benzoyl peroxide (BPO) as a topical treatment for HS is based on its use for the same theoretical reason—decreased bacterial colonization—in other dermatological conditions such as acne vulgaris. The compound destroys bacteria by creating free radicals that disrupt bacterial proteins via oxidation and also exhibits a mild sebostatic and keratolytic effect postulated to be beneficial in treatment of HS. In one randomized trial, BPO was used along with topical clindamycin in both arms of therapy as the standard of care; laser therapy was added in the treatment arm. Both arms of this study showed improvement in HS from baseline.
BPO washes are available over the counter in formulations between 2.5% and 10%. Patients may continue their regular bathing schedule while simply replacing other soaps or cleansers with a BPO-containing wash. Given its keratolytic effects, BPO-based washes can lead to irritation and desquamation in addition to rare allergic hypersensitivity reactions. Patients should also be counseled to rinse thoroughly before initiating contact with hair or fabrics, as the reactive oxygen species created by BPO have been known to have a bleaching effect.
Zinc Pyrithione
Although best known as a topical antifungal agent for treatment of seborrheic dermatitis, zinc pyrithione has antiinflammatory and antiproliferative properties that also make it a theoretically effective choice as a topical antiseptic for HS. As a positively charged ion coordination complex, it derives its antimicrobial properties through cell membrane depolarization and inhibition of substrate transport and ATP synthesis. Its antiinflammatory and antiproliferative effects are due to modulation of dendritic cell activity and an accompanying reduction of inflammatory signaling. Expert opinion suggests zinc pyrithione may be non-inferior to chlorhexidine wash for HS ; however, there are currently no studies examining its therapeutic efficacy. Studies have indicated that the antimicrobial effects of zinc pyrithione outlast those of chlorhexidine, making it a theoretically better choice for those who desire long-lasting antiseptic effect from a single wash. There are no absolute contraindications for zinc pyrithione use; patients should be cautioned to watch for allergic or irritant contact dermatitis.
Zinc pyrithione is available for patients as a 0.25% spray and a wash up to 2% concentration. These formulations are easily applied to the hair-bearing areas typically affected by HS. In addition, these products are usually less expensive than other medicated washes such as chlorhexidine and are available without a prescription.
Triclosan
Triclosan is a halogenated bisphenol compound that acts via disruption of the bacterial cell wall and fatty acid synthesis. It is also active against biofilms, an important consideration in the treatment of HS, and has demonstrated notable antiinflammatory effects in ex vivo studies via the suppression of both acute and chronic mediators of inflammation. While it is recommended by several expert-developed guidelines, well-controlled studies are lacking at this time to support specific usage directions.
Of note, there is significant controversy regarding the safety and effectiveness of triclosan as an antiseptic. Due to concern regarding its role in bacterial resistance, potential endocrine toxicity, evidence of accumulation of triclosan in wastewater, and questionable efficacy as compared to other antimicrobial options, the United States Food and Drug Administration banned its inclusion in antiseptic washes in 2016. However, the product continues to be available outside of the United States, and many non-US dermatologists continue to recommend its use in the treatment of HS.
Ammonium Bituminosulfate (Ichthammol)
Ammonium bituminosulfate, also known as ichthammol, is a topical medication that has been used to treat a variety of cutaneous conditions. It is thought to have both antiinflammatory and antimicrobial properties through the inhibition of inflammatory cell-to-cell signaling, modulation of superoxide production, and mild inhibition of bacterial growth. It is recommended by multiple expert guidelines for treatment of HS ; however, no studies have been done to date that prove efficacy in prevention or treatment of HS-related inflammation or lesions.
Ichthammol is available over the counter in multiple forms but is most commonly used for HS as a 20% ointment. Though this compound is available worldwide, ichthammol is more commonly recommended by European clinicians than their US counterparts. There are no absolute contraindications to the use of ichthammol, and adverse effects are limited to skin irritation, though the sulfur-like odor of topical preparations may prove bothersome to many patients. Patients should be advised of the potential for staining of fabrics, skin, and hair with certain preparations.
Keratolytics
As HS is theorized to begin with follicular occlusion due to hyperkeratosis, preventing this initial event is another promising therapeutic target in the treatment of HS lesions. Keratolytics, which lead to separation and desquamation of the cornified epithelium, help to unblock occluded follicles and prevent future occlusion. In this section, the mechanism of action, level of supportive evidence, dosing schedule, contraindications, adverse effects, and available formulations will be discussed for keratolytics used in the treatment of HS.
Resorcinol
Resorcinol is a benzenediol chemical with keratolytic properties mediated through cytotoxicity and cytokine modulation, as well as antipruritic and antimycotic properties. It has been shown to decrease both pain and duration of HS abscesses with adequate treatment, with over 80% clinical resolution of lesions in a 1-month-long trial. However, there have to date been no controlled trials of resorcinol treatment, with current data limited to case-reports and open-label studies. It is also important to note that studies have been limited to lesions that do not have scarring or fistulas, as pilot data showed that such lesions were not amenable to resorcinol treatment.
Dosing of resorcinol is carefully titrated to reach a therapeutic concentration where adverse effects are still tolerable. Generally, a 10% cream is applied twice daily for the first week, with concentration then increased by 5% each week until lesions and pain begin to resolve, at which point the concentration is kept constant. The final prescription is usually for at least a 15% cream as keratolysis is minimal below this concentration, though creams up to 30% concentration have also been used for other dermatologic indications. Maintenance therapy involves prophylactic application twice weekly. Resorcinol is not available in the United States except via specialty compounding pharmacies, which can significantly increase the price and be an inconvenience for both patient and physician.
There is risk of contact dermatitis with use of resorcinol, as well as brownish hyperpigmentation of the skin. Resorcinol is not recommended for concurrent use with intense pulsed light (IPL) for HS due to the combined irritative effect. Resorcinol will also cause desquamation in most patients, and moisturizers may be used to mitigate this side effect. Of note, resorcinol also has potential to interfere with thyroid hormone synthesis at elevated concentrations in the bloodstream, and thus should be avoided in open wounds of pregnant patients in the absence of sufficient safety data.
Azelaic Acid
Azelaic acid is commonly used in the treatment of acne and has been postulated to have a theoretical benefit for patients with HS. Its major mechanism of action is the modulation of keratinocyte proliferation, though it has been shown to dampen inflammatory cytokine signaling and exhibit antifungal and bacteriostatic properties. No formal studies are available to demonstrate its benefit in HS, so it is generally not used for this indication. There is limited expert opinion that discusses use of azelaic acid cream in pediatric HS.
Formulations of azelaic acid consist of gels, creams, and foams with up to 20% concentration. For acne and acne rosacea, dosing schedule is up to twice daily; however, optimal dosing schedule has not been independently investigated in HS. Patients should be cautioned about the drying effect of azelaic acid preparations, as well as the potential for photosensitivity, irritant or allergic contact dermatitis, and changes of skin color in darker-skinned individuals. There are no absolute contraindications to the use of azelaic acid.
Retinoids
Retinoids, such as tretinoin and adapalene, are structurally related to vitamin A and promote keratinocyte maturation via transcription factor modulation. They also have antiinflammatory properties via alterations to multiple pathways in the inflammatory response, from reactive oxygen species release to cytokine signaling. While these properties would carry a theoretical benefit for the treatment of HS, this has not been true in clinical practice, and current expert opinion is that topical retinoids are not recommended in the treatment of HS.
Bathing Additives
While bathing additives can provide an antimicrobial strategy similar to the antiseptic washes previously discussed, emerging evidence suggests that some bathing additives are associated with antiinflammatory, reparative, or antioxidative properties, which could provide additional benefit in the treatment of HS. Current expert opinion on bathing additives in HS is limited to that of bleach (sodium hypochlorite) baths. Though magnesium sulfate (Epsom salt) baths and other soaks are popular among patients, there is a lack of scientific support or clinical evidence from similar dermatological conditions for such therapies. In this section, both bleach baths and Epsom salt baths will be discussed, with Epsom salt baths serving as the bridge to the concluding section of this chapter, “complementary and alternative therapies.”
Bleach Baths
Bleach (sodium hypochlorite) is best known as an antimicrobial household cleaner, for which it relies on the creation of superoxide radicals to destroy bacteria, spores, viruses, and fungi. Previous studies have found that dilute (0.005%) bleach baths create a bacteriostatic effect in as little as 5 minutes, and the superoxide radicals exhibit a concentration-dependent ability to penetrate and dissipate biofilms created by bacteria. However, it is important to note that recent evidence suggests dilute bleach baths have no direct antimicrobial ability, thus any benefits may not be due to the previously presumed antiseptic properties. Bleach also exhibits antiinflammatory properties that have made it an important part of dermatological therapy in recent years, particularly as treatment for acute flares of atopic dermatitis. This antiinflammatory effect is postulated to be due to the modulation of nuclear factor kappa B transcription factor, signaling and resulting in decrease of inflammatory cytokine levels. While there have, as yet, been no studies of the efficacy of bleach baths for HS, their use is recommended by several treatment guidelines developed by expert committees.
Bleach baths are typically kept to 0.005% bleach (0.5 cup of household bleach per standard 40 gallon [150 L] bathtub) for optimal benefit while avoiding caustic damage to the skin. More concentrated preparations have been known to cause urticaria and irritant contact dermatitis. There are no clinical studies demonstrating the effect of varying frequency of bleach baths for treatment of HS, but 2 to 3 times weekly at 0.005% concentration is thought to produce benefit. Patients should be cautioned regarding the caustic effects of concentrated bleach on the skin, as well as the potential for bleaching of hair and fabrics. Although pigmentation changes may occur with more concentrated preparations, skin pigmentation should not occur at the recommended 0.005% concentration.
Magnesium Sulfate Baths
Magnesium sulfate baths, colloquially known as “Epsom salt soaks,” have long been a favorite of those seeking non-pharmacological treatment for dermatological or musculoskeletal complaints, with claims of healing illnesses, reducing bodily aches and pains, and tempering inflammation. Unfortunately, no study has been able to prove an antimicrobial, analgesic, or antiinflammatory benefit to these soaks. However, patients have anecdotally reported both in the clinic and in online forums that they find these baths soothing and perceive benefits in their daily function. While reports of toxicity secondary to hypermagnesemia from Epsom salt enemas have been published, there are no reports of adverse effects from these baths. Given the lack of evidence of harm, patients can be advised to continue such regimens if desired, though counseling regarding proven disease-modifying interventions should also be offered.
Complementary Therapies
Many patients with chronic diseases that prove recalcitrant to conventional medication regimens explore complementary and alternative medicines (CAM), and those who suffer from HS are certainly no exception. These therapies often appear on online message boards and support groups, and it is common for HS patients to not inform their healthcare provider about their use of CAM. Topical CAM that have been purported as helpful (but that lack studies in HS) include turmeric, cannabidiol (CBD) oil, menthol, aloe vera, tea tree oil, apple cider vinegar, iodine, zinc paste, and others. CAM therapies are discussed extensively in Chapter 28 ; however, the most widely used topical CAM therapies will be covered in this chapter (including magnesium sulfate baths, CBD oil, and turmeric).
Cannabidiol Oil
CBD oil is thought to assist in wound healing and pain relief. In addition to its ability to decrease pain perception, in vitro studies have also shown CBD to inhibit keratinocyte proliferation while regulating cellular differentiation and promoting apoptosis of both keratinocytes and sebocytes. Current evidence beyond patient anecdotes is lacking for its long-term safety and effectiveness in treating HS.
Turmeric
In vitro, turmeric has been shown to disrupt bacterial membranes, inhibit bacterial replication, and disrupt microbial biofilms. It may possess antiinflammatory and antiproliferative potential via modulation of NF-κB signaling and phosphorylase kinase activity. While it can be taken as a systemic medication, it has a long history of use as a topical therapeutic. However, studies of topical turmeric in HS are needed to determine efficacy.
Summary
Topical therapies are an important part of the clinician’s treatment arsenal for HS. While their use has the potential to provide more complete relief in the case of mild or Hurley stage 1 disease, utilization as an adjunct in later stage disease can still provide benefit. Most lack large-scale or well-controlled studies, and as such the decision of the optimal topical regimen must be an open dialogue between the clinician and patient based on expert opinion, clinical experience, and the trajectory of the individual patient’s disease. Owing to their relative ease of use and very low risk of side effects, most experts recommend all patients with HS use a daily antiseptic wash (most commonly BPO, chlorhexidine, or zinc pyrithione) and a topical antibiotic (most commonly clindamycin solution or lotion).
References
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


