Introduction
The treatments for hidradenitis suppurativa (HS) can generally be divided into those with pharmacologic focus, and those that are procedural. For milder Hurley stage I disease, management is usually medication-focused, and designed to control or prevent the inflammatory events. For more severe disease, the physical signs of scars, acute or persistent abscesses, nodules, and sinus tracts may be accompanied by symptoms of ongoing or acute pain, drainage, itching, and odor. It is therefore in the setting of incomplete control of either signs or symptoms of the disease that procedural management becomes an important option.
Procedural Options
Procedures may be categorized by their applications in (1) the acute manifestations of the disease, or (2) for chronic, persistent disease. When treating acute lesions, it is helpful to note that the intensity of inflammation alters the pH of the perifollicular dermis, leading to blunting of the effectiveness of local anesthetics. It is, therefore necessary to often administer a “ring” of anesthesia outside the inflamed lesion. Additionally, the presence of scarring, multilocular abscesses, or sinus tracts may limit anesthetic dispersal, and thereby reduce the effectiveness of anesthetic agents.
Treatment of the Acute Lesion
Management of the acute lesion can be pharmacologic, destructive, or ablative in nature.
Acute flares may be initially managed with medications, with treatment options including oral or intralesional anti-inflammatory agents, antibiotics with anti-inflammatory properties, or analgesics. The question of superinfection with bacterial pathogens should be considered; this may be suggested by the presence of prominent erythema and warmth surrounding the primary process, and/or increasing malodor. Culture, and treatment with appropriate antibacterial agents, may be warranted.
Procedural treatments may be considered for those lesions that might be uncontrolled with pharmacologic agents alone. Large abscesses, or lesions comprised of sinus tracts and/or scars, are especially not likely to be successfully managed with only pharmacologic therapy. Intralesional corticosteroids may help to reduce acute pain in the short term, but are often ineffective in acute, larger cavitary lesions.
Unroofing/Deroofing, Incision, and Drainage
Unroofing and incision and drainage (I&D) are most beneficial for the solitary abscess or tract; they are less effective in the more chronic lesions where there may be scarring, nodules, and sinus tracts. For management of larger, acute lesions, a procedure to facilitate release of the purulent material within an abscess is often associated with almost-immediate symptom improvement. I&D is usually effective in reducing acute pain, but is associated with significant risk of recurrence. Unroofing, also known as deroofing, is generally more effective than I&D, and results in less risk of recurrent abscess formation. It may be helpful especially where there is a single cavitary abscess. Unroofing/deroofing and I&D are discussed in detail in Chapter 22, Chapter 23, Chapter 24 .
Other options for procedural treatment of HS lesions may be broadly categorized into two general choices: (1) destruction/ablation, or (2) removal. Destruction may be defined as the ablation of the inflammatory process, without physically removing tissue. Alternatively, physical removal of affected skin may be employed, with various options for wound-healing. Local anesthesia is appropriate for all these procedures.
Destruction
Destruction of the acute lesion attempts to produce controlled injury to the tissue, followed by healing with lesion resolution. Multiple approaches have been evaluated, including carbon dioxide laser ablation, radiotherapy, peeling agents, cryoinsufflation, and neurotoxins. Each of these will be reviewed, with strength of recommendations as noted in Table 26.1.
| Modality | Strength of Recommendation | Level of Evidence |
|---|---|---|
| Incision & Drainage | C | III |
| Unroofing/Deroofing | B | II |
| Cryosurgery | C | III |
| Cryoinsufflation | E | III |
| Peeling Agents | B | II |
| Neurotoxins | D | III |
| CO 2 Laser Excision | C | II |
| CO 2 Laser ablation | C | II |
| Staged CO 2 Laser Excision/Marsupialization | C | II |
| Radiation | C | II |
Treatment of the Chronic Lesions
Carbon Dioxide (CO 2 ) Laser Ablation
Laser ablation has the same goals as that noted with cryo- or electro- surgical approaches; that is, the destruction of the inflammatory process. Although potentially able to treat acute lesions, the treatment is largely reserved for Hurley stage II to III patients with chronic disease.
The principle of such treatment relies on the laser energy absorption by the moisture of skin, with the resultant thermal effects causing destruction of the targeted lesion. The technique is usually performed using local anesthesia. Patients may continue pharmacologic therapy without interruption.
In 1987, Darlymple and Monaghan described the use of CO 2 laser to ablate HS lesions in six patients with a variety of sites. Subsequently, in 1991, Sherman and Reid reported using the CO 2 laser to treat large areas of the vulva in 11 patients, employing a combination of laser ablation and focal areas of laser excision.
The technique is performed as follows. The visible and palpable margins of the lesion to be treated are identified. The laser parameters are set for scanning/defocused mode, to make repeated passes over the HS lesion. Treatment is continued until the delivery has reached the pre-set depth and margins of the affected lesion(s). All elements of HS, including abscesses, nodules, scars and sinus tracts may be treated. Healing takes place by secondary intention. The presence of thickened scars and/or extensive epithelial-lined sinus tracts may blunt the effects of the scanning laser.
The technique has been associated with good patient acceptance, acceptable qualities of healing, and improved comfort of treated areas. However, recurrence rates approach 30%. A potential side effect is a post-operative flare of other involved areas. Laser treatments for HS, including Nd:YAG, are further discussed in chapter 25 .
Radiotherapy
Superficial x-ray therapy has been used for over 75 years to treat numerous dermatologic diseases. It was used to successfully treat dissecting cellulitis of the scalp as well as axillary HS. While superficial x-ray therapy fell out of favor in the 1970s, superficial radiotherapy is valuable for the subset of HS patients who have severe disease and have failed all other therapies. Today, electron beam therapy is the source of superficial radiotherapy, and has been used to successfully treat acne conglobata, axillary HS, and dissecting cellulitis of the scalp.
Treatment of chronic lesions of HS with ionizing radiation has been suggested for recalcitrant lesions or for patients who may not be surgical candidates. X-ray therapy has been used to treat areas of variable size when such circumstances exist. In 1950, Schenck reported a series of 54 patients treated three times per week for 5 to 10 treatments, with virtually all patients showing clinical improvement. However, there is little published data in the recent literature addressing this modality, and older reports detail the results from treatment using orthovoltage.
Fröhlich et al. treated 231 HS patients with orthovoltage therapy using multiple fractionation regimens. Of the total treated, complete amelioration of symptoms was seen in 38%, with an additional 40% seeing improvement. No side effects were noted. They felt their results warranted more attention to superficial radiotherapy as an effective treatment for severe HS.
Dissecting cellulitis of the scalp is quite difficult to treat. Chinnaiyan et al. treated four patients with electron beam and/or photon therapy. All patients experienced significant pain reduction as well as decrease in drainage and nodule size. Because these patients already had significant hair loss secondary to scarring, dosing was selected not only to treat the inflammatory element but to also ensure as little residual hair growth as possible.
Myers et al. treated a 53-year-old man with long-standing severe acne conglobata and HS after the patient had failed multiple therapies. The patient underwent several sessions of electron beam radiation to large plaques on the cheeks. At 3 weeks, cyst size, drainage, pain, and self-esteem were all improved. No dryness or pigmentary changes were noted. These changes persisted to the 5-month follow-up visit.
Trombetta et al. treated one patient with stage III HS, refractory to all other therapies. Significant improvement was seen 3 weeks after treatment and was proven to be a durable change. Small persistent lesions were treated with additional fractions.
Patel et al. treated five patients suffering from severe refractory HS with various fractions of electron beam therapy to multiple areas. Some response was noted in all patients 2 months after treatment, but only in the axillary region. No response was noted in the perineal areas. The authors suggest that the significant scarring in these areas was deeper than the radiotherapy could penetrate, thus compromising the effect. Prolonged follow-up was noted to be difficult, as all patients went on to receive different additional treatments for their HS.
One case report detailed radiation treatment induction of HS. The patient, a 52-year-old woman with axillary, inframammary fold and groin involvement, underwent 6 weeks of radiation therapy for breast ductal carcinoma in-situ (DCIS). She developed an HS flare only in the window of her radiation treatment. The authors post that the significantly higher dosing for DCIS induced a greater immune response leading to the flare. As a cautionary note, it is recognized that the clinical findings of HS may mimic clinical findings of metastatic breast cancer. Inflammatory lesions should have diagnostic pathologic findings before being considered for radiotherapy.
Superficial radiotherapy has played an important role in the treatment of HS for many years. There are few studies looking at large numbers of patients, and a long-term follow-up is not available for any of these patients. Most of the literature details treatment, specifically in severe refractory cases of HS. In 1965, Zeligman detailed his experience with a single dose of superficial x-ray therapy, which he felt would provide temporary epilation. In his hands, this dose resulted in long-term resolution of chronic HS.
Unfortunately, there is a great deal of concern evinced by patients when superficial radiation treatment is offered as a treatment, whether for skin cancer or HS. This could be a reason why it is not offered or performed more often. There is a need for better optimization of regimens, which will be difficult to achieve because of such concerns. Patel et al. and Trombetta et al. both used similar regimens to effect change, which appears to have been efficacious.
The authors feel that superficial radiotherapy should be considered when the following criteria are observed: contraindication or failure of systemic therapy; significant and ongoing debilitation; age greater than 60; areas of involvement are so large and/or comorbidities preclude or mitigate against successful surgical therapy. One of us (BR) has used superficial radiotherapy to treat two patients, both with significant buttock and perirectal disease. Both patients were over the age of 60, had failed multiple therapies including several biologics, and their disease was not controllable with standard therapy. It was felt that the benefits of the therapy outweighed the short and long-term risks. In both cases, significant decrease in discharge and pain were noted within 2 weeks of treatment and persisted after treatment for at least 1.5 years. One patient refused additional treatment but offered no criticism of the superficial radiotherapy he had previously received. The other patient’s treated disease remained in remission but the patient died of unrelated causes.
A caution, based upon personal observation, is that newer radiation delivery modalities have the potential to be highly penetrative, and that the use of such therapy has the potential to cause injury to deeper structures. Since the localization of HS is largely dermal, such depth may not be needed for clinical response. In some patients, skin breakdown and delayed healing have been noted (PH personal observation). Currently, there is inadequate data to evaluate such therapy.
Peeling Agents
Resorcinol, a vitamin A derivative, is the only peeling agent reported in the literature as a treatment for HS. The suggestion that HS is a disease in which follicular occlusion plays a part suggests that topical keratolytic like resorcinol and retinoids could represent a logical treatment. Topical retinoids such as adapalene, tazarotene, and tretinoin have long been used for their keratolytic action in acne, but there are no studies of these medicines in HS, perhaps because they do not have enough peeling effect.
Based on several case reports showing resorcinol to be of help in HS, an open trial was created to evaluate resorcinol cream’s ability to mitigate flares and reduce pain. The study looked at 12 patients with Hurley stage I or II disease. All participants had significant flares and a high pain score. Resorcinol 15% cream was applied twice daily when flares began and could be used once daily as maintenance. Most reported significant pain reduction within 2 days of inception. Breakthrough flares were more easily controlled with the topical resorcinol. While the topical had little control on limiting the number of flares, they were more easily controlled when they did occur, and pain levels were significantly reduced.
In a more recent study, resorcinol 15% was again evaluated in an open trial of Hurley stage I and II patients, using both clinical and ultrasonographic measures. A total of 32 patients were evaluated. Topical resorcinol was again shown to reduce pain and clinical size of the treated lesions. However, ultrasound showed persistence of inflammation after it was clinically resolved, suggesting incomplete response.
The mechanism of action for resorcinol is its putative keratolytic action. However, other factors may be at work. Resorcinol is a derivative of phenol, which is well-known for its topical anesthetic effects. This may be the reason for its ability to ameliorate pain when used topically in HS, while its keratolytic action mitigated flares. Resorcinol cream appears to offer real effect regarding pain control and reduction of acute flares. However, resorcinol USP is no longer available in the United States, due to a lack of manufacturers, and there appears to be no change in these circumstances expected in the immediate future.
Cryoinsufflation
Although generally suggested for more chronic HS lesions, cryodestruction can also be used as an ablative therapy for acute lesions. The agent may be delivered by spray or through direct contact with a cotton-tipped applicator. It has generally been recommended for smaller lesions, and in the experience of the authors, may require multiple applications to achieve complete resolution.
Cryoinsufflation was introduced to help those patients suffering from stage II or III HS and who could not use or tolerate systemic medical therapies, or who had chosen to defer or had failed other surgical techniques. Pagliarello et al. published the first paper in 2014, detailing two patients who desired definitive treatment but were not able to tolerate standard medical therapies.
The technique is straightforward (  ). A hollow needle or catheter is placed within a tract and liquid nitrogen is introduced via a standard cryo-gun and a Luer-lock attachment. The gas expands to pass through and fill the existing tracts, and then advances through distant fistulous openings to the exterior. Treatments are repeated up to three times at monthly intervals to allow for the greatest healing. Both patients in the original paper achieved clearance of the localized disease treated, with no additional scarring or color change. Local anesthesia was used and gave adequate pain control. Post-procedural pain was reported to be minimal and managed with paracetamol (acetaminophen).
). A hollow needle or catheter is placed within a tract and liquid nitrogen is introduced via a standard cryo-gun and a Luer-lock attachment. The gas expands to pass through and fill the existing tracts, and then advances through distant fistulous openings to the exterior. Treatments are repeated up to three times at monthly intervals to allow for the greatest healing. Both patients in the original paper achieved clearance of the localized disease treated, with no additional scarring or color change. Local anesthesia was used and gave adequate pain control. Post-procedural pain was reported to be minimal and managed with paracetamol (acetaminophen).
In 2015, the same group presented some technical refinements to the original procedure. These changes were prompted by concerns for air embolus and necrosis at the entry points. The possibility that the needle could potentially be advanced into the subcutaneous space, and redirect gas flow from the tunnels into the subcutaneous space, was worrisome. The use of a 21–gauge olive–tipped catheter was proposed, which, with its blunted tip, would obviate the concern for placing the gas in the subcutaneous space. A chlorhexidine solution was sprayed onto the site to gauge gas outflow by the appearance of bubbles at points of exit.
There was also concern that the use of metal needles might produce necrosis at the entry points as a result of ice-ball formation where the needle shaft meets the overlying skin. Short pulses of liquid nitrogen would seemingly serve to reduce the possibility of formation, while allowing enough gas to traverse the tunnels. The use of small plastic intravenous catheters was alternately proposed in an attempt to decrease the likelihood of formation of ice–balls at the entry points.
In 2019, Daveluy suggested that cryoinsufflation might be a valuable diagnostic tool in other surgical approaches such as unroofing and CO 2 staged marsupialization. Running liquid nitrogen through the affected skin would help delineate the area to be treated, and possibly reveal tracts not obvious to palpation.
In an interesting modification to the standard technique of I&D, Molina-Leyva et al. reported a technique using liquid nitrogen for either acute or chronic abscesses of HS. After the contents of an abscess were drained, liquid nitrogen was used to scar the pocket closed. A 4 to 5 mm disposable punch biopsy trocar was used to incise the abscess. The abscess contents were drained and the resultant pocket flushed with saline. The trocar was then reintroduced, and liquid nitrogen was introduced into the pocket by the simple expedient of placing the tip of the cryosurgical unit flush to the rear handle opening of the hollow trocar. They used 5 second applications, repeated twice. The area was then drained with the drain hole left open. Complete resolution, defined as no inflammatory signs observed, and no persistence of fluid collection noted by clinical and ultrasound examination, was achieved in 70% (7/10) of the treated lesions in one month. Post-procedural pain was minimal, and no adverse effects were noted in the treated population.
This technique is relatively straightforward and is not equipment intensive. One of us (BR) has used it for a number of patients since it was delineated, with variable results. Patients whose circumstances would make them good candidates for cryoinsufflation most often had so much involvement that it precluded use of the technique. Those who completed the course of treatment were uniformly pleased with the results. Although there is relatively little published data, the authors believe that it should be included in the procedural options for appropriate patients. A cautionary note reflects the observation that the contents of the abscess or scarred tract being treated will be expelled along with the gas. Placing a gauze over the treated area while injecting the gas will contain any expelled contents.
Neurotoxins
Neurotoxins such as onabotulinum toxin A and abobotulinum toxin A have shown some positive effect in the treatment of HS. The mechanism of action is proposed to be a downregulation of apocrine gland function, possibly reducing the potential for follicular occlusion. Alternatively, reduction of sweating may change the environment by reducing humidification.
Neurotoxin was first used in 2005 to treat a young woman with HS (stage not noted). Its use was prompted by symptoms of hyperhidrosis, although a diagnosis of focal hyperhidrosis had not been made. A total of 250 units of abobotulinum toxin A was used for both axillae and the patient experienced a cessation of symptoms beginning 2 weeks after injection, and lasting for 10 months.
In 2009, onabotulinum toxin A was used in a 7-year-old girl with stage I HS who had failed several topical and oral therapies. A total of 40 units was injected in both inguinal folds in the standard 1 cm point model used in hyperhidrosis. She experienced 6 months of remission. A few lesions occurring towards the end of that period responded to a second treatment in the same way as the first.
Khoo and Burova reported on their results with botulinum toxin A in three patients. Their most successful case involved a 46-year-old woman with stage II disease who had failed numerous topical and oral therapies. Noting the presence of hyperhidrosis in the axillae, onabotulinum toxin A 50 units was injected in each axilla. She showed some response and went into remission after the second treatment 3 months later, and remained in remission and was discharged from follow-up after her fourth treatment. They note that this degree of response was not mirrored in their other two patients, although each experienced disease-free intervals of 5 to 6 months after treatment.
Successful use of onabotulinum toxin A in a 41-year-old woman with stage III HS and obesity has also been reported. The patient had failed all treatments and presented to the authors’ physical medicine and rehabilitation clinic for chronic pain management. She was initially treated with 400 units into the bilateral axillary and inframammary folds (100 units in each site). She had good response on follow-up and reported 50% pain relief. Additional injections at a dosage of 50 units per site showed effect, but symptoms returned more quickly. With resumption of 100 units per site administration, treatment was more successful, and she remained “open-wound-free” with periodic injection sessions. This success was notable as most of the previously reported patients had been stage I and II. Its success in a Stage III patient is exciting.
Campanati et al. treated two patients with botulinum toxin A, both Hurley stage II. The first, with disease limited to the axillae, had failed topical and oral therapies. A dose of 50 units per axilla was used. The second patient had disease involving the groin and thighs. Topical and oral therapies did not reduce the pain and drainage. A dose of 100 units per area was used. Both patients experienced close to 10 months of little to no pain and no evidence of active disease. Like the results experienced in hyperhidrosis treatment, both patients began to experience recurrence of their disease symptoms at this time.
Based on these reports, botulinum toxin A and B remain viable options for both pain and disease control. The treatment regimens differ wildly, as do the unit counts. Because the areas are those concomitantly involved in hyperhidrosis, a starting point for standardization would be dosing used in that disease, typically a 5cc dilution resulting in a 2 units per 0.1cc dosing scheme. The authors’ experience and communications among US colleagues regarding the use and success of botulinum toxin A and B in the treatment of their HS patients reveals that it is rarely used. When it is used, it does not deliver the dramatic effects evident in the literature. Standardization of treatment regimens may help augment its success. However, significant financial barriers to the wide-spread use of neurotoxins exist in the United States and many other countries. This technique is off-label for HS and is usually denied by insurance companies and governmental health benefit payers. It is expensive if paid for privately, and patients may have unreasonable expectations if an expensive therapy requires multiple sessions to generate variable results.
Excision/Removal
Wide Local Excision
Wide local excision has been the most common surgical treatment in patients with chronic or extensive disease. It will be discussed in detail in Chapters 23 and 24 .
Electrosurgical Stripping Excision
A procedure similar to scalpel excision, skin tissue-saving excision with electrosurgical peeling (STEEP) employs electrosurgical instrumentation to remove diseased tissue in a tangential, stepwise fashion. The goals are preservation of unaffected tissue and the production of improved healing. This technique is also discussed in Chapter 24 .
CO 2 Laser Excision
In 1996, Finley and Ratz reported the use of CO 2 laser to excise lesions of HS in 7 patients and 12 sites. A single recurrence was reported in follow-up of 10 to 27 months. Additionally, in 2008, Madan et al. reported similar results in 9 patients involving 27 sites treated with laser-excision.
In contrast to carbon dioxide laser ablation, CO 2 laser excision uses the energy of the instrument in focused mode to excise individual lesion(s) of HS. It is primarily indicated for Hurley stage II to III lesions that are refractory to pharmacological management. After determining a pre-surgical margin, the laser is used as a cutting tool to carry out the removal process; it is similar in concept to that performed using scalpel excision or electrosurgical stripping.
The technique generally used is as follows. The margins of the individual lesion are defined, and local anesthesia administered. The CO 2 laser is then used in continuous, cutting mode as a scalpel to excise the delineated lesion. It is not used to address an entire physical unit, such as an axillary or groin plaque. It differs from CO 2 laser ablation in that the energy is delivered in focused mode, and that affected tissue is physically removed. Healing generally takes place by secondary intention. The procedure is associated with high patient satisfaction and good qualities of wound healing.
Staged CO 2 Laser Marsupialization
En bloc excision with primary closure is the most common surgical procedure performed for patients with HS and is designed to remove the scarred skin in a large block, including a significant amount of subcutaneous tissue. The extent of surgery is driven by visual assessment, palpation and inspection for possible sinus tracts. The resulting defect is then primarily closed with sutures, staples, split-thickness skin graft, or a musculocutaneous flap. The healing process may be long and involved, with bed rest and wound vacs the norm. Postoperative complications including wound dehiscence, graft and flap failures, infections, and reduced range of motion are common. Recurrence rates after excision and primary closure are high, ranging from 20% to 70%, and the resulting scars can be quite disfiguring.
In 2010, Hazen and Hazen reported success in managing a series of 61 patients with CO 2 laser using a technique they termed excision and marsupialization. Patient selection was based on physical findings as well as symptoms of pain, drainage, odor, itching, the frequency and severity of flares, and the degree of functional impairment as reflected by the Dermatologic Life Quality Index (DLQI) score. The procedure used the CO 2 laser as a cutting tool, followed by the intrasurgical evaluation and removal of occult areas of HS. The procedure resulted in a pocket-like (marsupial) defect. The technique had the advantages of office delivery, local anesthesia, minimal surgical complications, and low recurrence rates. Areas treated included the axilla, groin, vulva, perirectal skin, scrotum, abdomen, breast, neck, scalp, and face. Recurrence rates were less than 2%.
Since the original description, the authors have had significant opportunity to perform and evaluate this technique. This highly regarded procedure is predicated on the observation that HS begins within the mid deep dermis and is concentrated within the skin. It is not a primary disease of the subcutaneum or muscle.
Medical therapy is intended to suppress as completely as possible the chronic inflammatory nature of the disease. However, the scarred, oozing disfiguring plaques will almost always be a source of pain. The ability to eliminate the plaques and nodules reduces the burden of HS in a patient. Frequently, all physical evidence of disease can be removed in patients who undergo the procedure. Many of these patients can stop all medicines, with the understanding that suppressive therapy may be reinstituted at the onset of a new inflammatory lesion.
Almost all patients with scarred plaques, nodules and sinus tracts are candidates for this surgical procedure. It is therefore usually reserved for Hurley stage II or III disease. Most patients are candidates for in-office surgery under local anesthesia. In our experience, lidocaine with epinephrine or tumescent anesthesia, which may be coupled with inhaled nitrous oxide or oral anxiolytics, make the procedure more comfortable for both patient and surgeon. General anesthesia may be needed for those patients with recurrence in an area of previous surgical treatment, as adequate anesthesia can be difficult to achieve in these areas due to scar tissue blocking diffusion into all targeted areas. Many patients will require general anesthesia for extensive disease, or extensive perianal, vaginal, and scrotal involvement. Patients with significant surgical anxiety or allergies to the components of local anesthesia may also desire general anesthesia.
Contraindications to treatment primarily relate to associated patient co-morbidities. Pre-surgical evaluation of clotting capabilities, as well as cardiovascular, endocrine, infectious, or wound and pain management issues should be performed. This is true especially if a general anesthesia is to be employed. The procedure is usually performed in an office setting using either intradermal or tumescent local anesthesia. If medically appropriate, anticoagulants may be withheld before and during surgery. It has always been the authors’ practice to maintain all HS-suppressive medicines including biologics before, during, and after surgery. It has been observed that healing is more rapid with controlled disease. Both authors have a zero percent infection rate, which mitigates the prevailing and long-held fear that biologic medicines may precipitate infection in surgical wounds.
The extent and borders of HS lesions to be considered for surgery are determined by visual and palpatory evaluation. To improve the identification of occult disease, some investigators have suggested that injectable dye material be injected into prospective surgical lesions to further identify the extent and location of involved areas. Recently, ultrasound of Hurley stage II to III lesions has confirmed the identification of dermal scars, abscesses, and interconnecting epithelial-lined sinus tracts. Furthermore, evaluation of the ultrasound findings seems to be able to identify those patients, and occult areas, most likely to benefit from surgical intervention. Whether the information gained with injectable dye or ultrasound will better guide the surgical process than the visual and palpatory examination is uncertain.
In contrast to pre-surgical dye or ultrasound evaluation of HS lesions, Staged CO 2 Laser Marsupialization uses an intrasurgical evaluation process to aid in the identification and treatment of affected areas. In concept, the technique is very similar to the standard of care for staged removal of cutaneous malignancies, Mohs micrographic surgery. Like Mohs, the concept is to intrasurgically identify occult areas of disease, thereby facilitating as complete a removal of HS tissue as possible, while preserving uninvolved tissue.
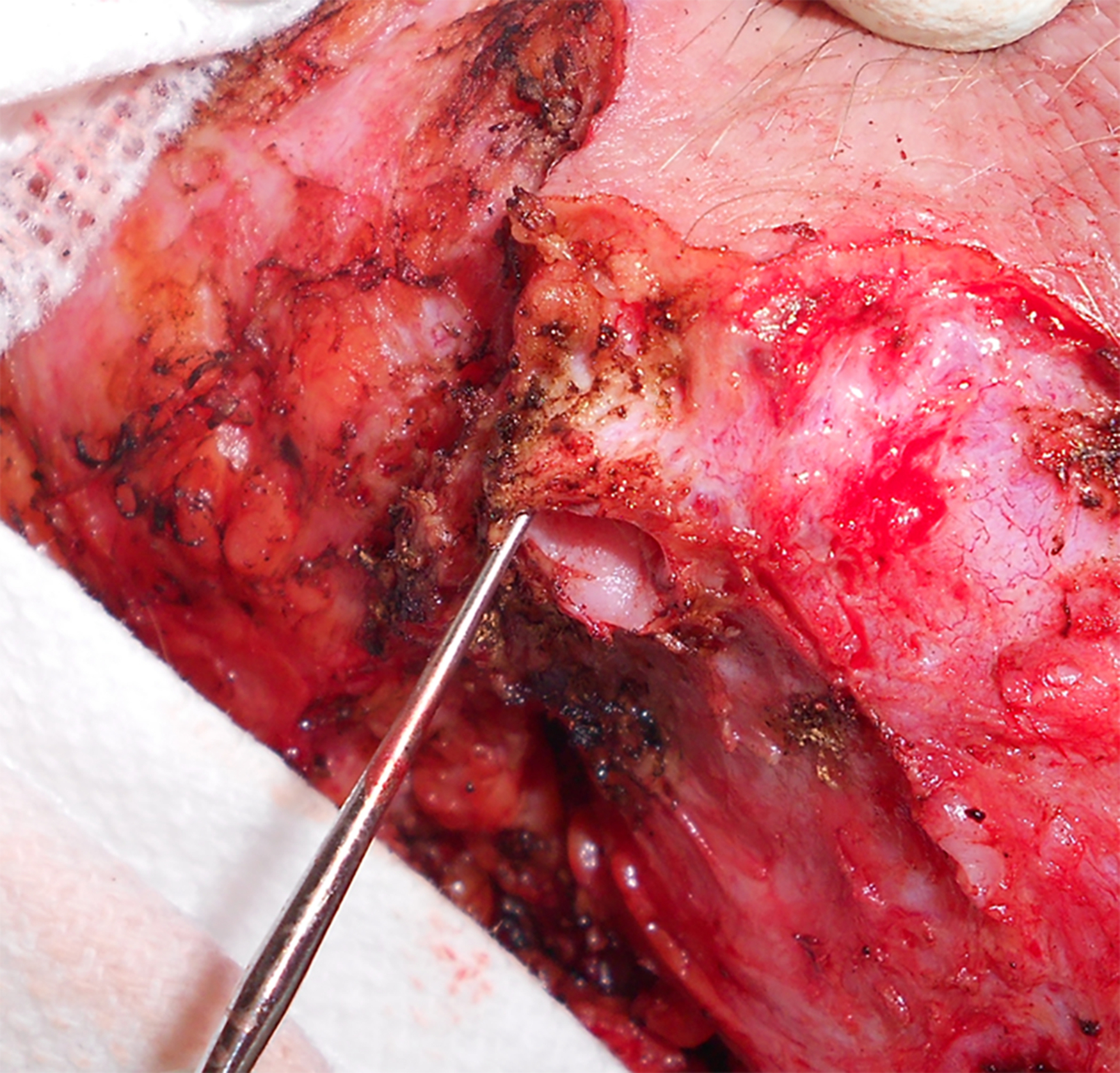
The surgery is performed as follows: The extent of the planned marsupialization is outlined with a skin marker. Local anesthesia is placed. Using the CO 2 laser in focused mode, a 2mm margin is used to excise the area of HS. Minimal bleeding and minimal tissue contraction allow for the preservation of the internal architecture of the wound. Additional areas of occult disease may be identified visually or with a probe or a 1mm ice-cream curette, which is used to “run the border,” physically searching for additional missed tunnels (  ).
).
Four potential abnormalities may be noted on the underside of the plaque as it is carefully freed from the subcutaneous tissue:
- 1.
A translucent, bubble-like outcropping or “bulge.” This is usually seen to extend from the underside of the inflammatory mass.
- 2.
Epithelial-lined sinus tracts. The extent and direction of such tracts may be identified by use of a 1mm ice-cream scoop curette placed within the lumen of the tract. Transit through the tract may identify a distant cutaneous exit point ( Fig. 26.1 ).