Introduction
Successful treatment of a patient with hidradenitis suppurativa (HS) requires a multidisciplinary approach. As such, establishing a multidisciplinary HS clinic is crucial to address this multifaceted disease. Having a basic treatment algorithm, expertise in the field, access to other specialties for referral, knowledge and access to the latest research, and quality improvement initiatives are all important in establishing a successful HS clinic.
Treatment Algorithm
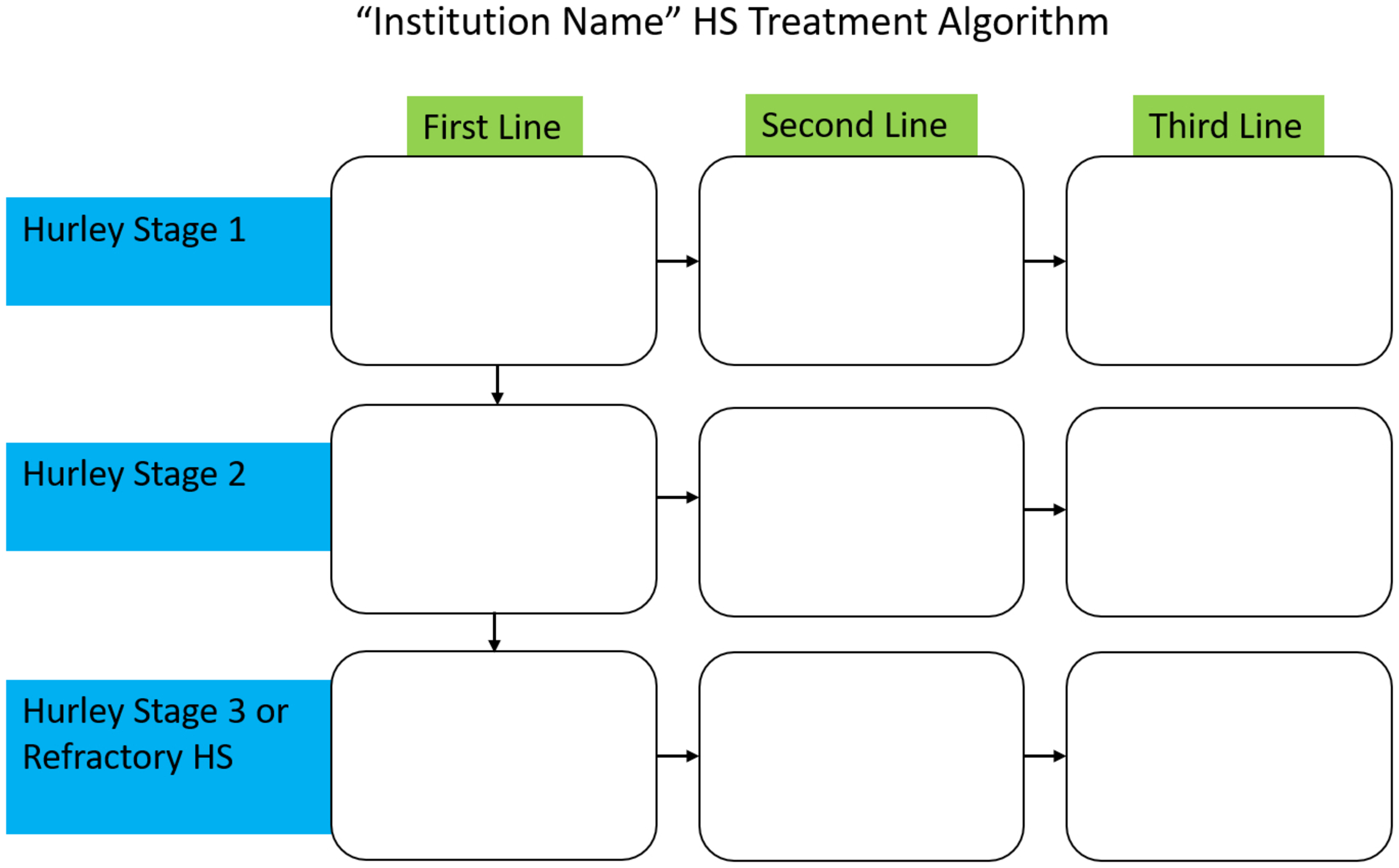
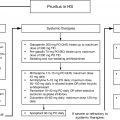
Every patient with HS presents differently, and accordingly, every patient should have an individualized treatment approach. Having a multidisciplinary HS care plan has been associated with high levels of patient satisfaction. Implementing a standard treatment algorithm can be a valuable implementation tool and starting point for residents, physicians, and other practitioners, particularly those who are new to treating patients with HS. Establishing an institutional treatment algorithm can allow for the inclusion of institution-specific information regarding local specialized pharmacies, collaboration with non-dermatology colleagues, and important institutional contact information. Various international groups have provided information on region-specific guidelines that can be referenced as a starting point and are discussed further in Chapter 14 . Disease severity classification methods such as Hurley staging and stability questions should guide this initial treatment approach and algorithm. An example of an institution-specific algorithm from Henry Ford Hospital, Detroit, MI, has been published, and a skeleton structure is shown in Fig. 32.1 . The goal of medical treatment is to stabilize and maintain low HS activity, while the goal of surgical treatment is to debulk affected tissue with the possibility of potential remission. A multimodal, individualized, and multidisciplinary approach should be applied, and institutional and clinic resources will guide the creation of the algorithm with site-specific components.
Domains of Expertise
To establish a successful multidisciplinary HS clinic, the clinic should be customized to the needs of the patient. Billing and insurance coverage for HS medications are important considerations. Since adalimumab is the only FDA-approved medication for the treatment of HS, prior authorizations are often needed to obtain coverage for many medications including biologics as well as for procedural treatments and lasers (e.g., neodymium-doped yttrium aluminum garnet [Nd:YAG]). Having friendly and knowledgeable clinic staff who can help handle these issues and communicate effectively with the patient and insurance company is crucial. A staff member(s) dedicated to these tasks can help to reduce the administrative burden.
Having expertise in wound care is also fundamental in establishing a successful HS clinic. HS patients often require multiple dressing changes per day due to chronic wounds and persistent drainage. Wound care supplies can consequently result in an extremely costly burden for patients. Determining the optimal wound dressing regimen and having helpful and affordable wound care recommendation options for patients is therefore essential (see Chapter 20 for comprehensive wound care management). If the HS clinic performs more invasive surgical procedures, including traditional surgical excisions or carbon dioxide (CO 2 ) laser excisions, having nursing staff with expertise in wound care is necessary to manage patients postoperatively and at follow-up visits. Access to a specialized wound care clinic can also aid in caring for patients who have chronic or post-operative, slow-healing wounds.
Knowledge regarding cutting-edge HS research is important to be able to convey this information to patients with HS as well as answer questions that arise from patients regarding new treatments. Staying up to date with current treatments and guidelines is also paramount. Having a research unit that conducts clinical trials or performs basic science research within your HS clinic offers a significant advantage, particularly with subject recruitment and the establishment of HS biobanks. Basic science HS research leads to a better understanding of the disease and leads to new treatment options with the goal being an eventual cure. Working closely, collaborating, and understanding the needs of basic scientists helps dramatically to advance the field of knowledge. If basic scientists researching HS require tissue or serum from patients with HS, where better to collaborate than with an HS specialty clinic? Having a dedicated and knowledgeable clinical research team can help facilitate the collaboration between clinical and basic science research. Understanding and working with institutional review boards is often an arduous process that can be managed effectively by a clinical research team.
Quality Improvement
Given the widespread prevalence of HS with an estimated 0.1% to 2% of the population affected and the relatively small number of physicians with an expertise in HS, specialty HS clinics can quickly become saturated. Thus, quality improvement initiatives to continuously improve the clinic as it grows are important. Videos on the various HS procedures can be created to be viewed by patients so they can be aware of what to expect pre-, intra-, and postoperatively. This also cuts down on lengthy physician explanations in a clinic.
In addition, implementing a shared HS clinic with multiple providers can help to decrease patient wait times. Educating other physicians in the department about the institution-specific HS treatment algorithm can help facilitate bringing others on board to participate in the HS specialty clinic. Implementing sub-clinics within the HS specialty clinic can also be beneficial. Establishing a nursing wound care clinic and educating nursing staff to care for chronic and post-operative HS wounds can help with clinic flow. Establishing an urgent HS referral sub-clinic to triage complex patients can also help with some of the more serious acute problems that patients with HS can experience, including flares, pain, and infection. Establishing a dedicated medical laser clinic can allow for patients to come in for scheduled laser treatments to be performed by nursing staff or residents to free up physician visit appointments for others with more acute needs. Additionally, given the ever-increasing research into HS, new treatments continue to emerge. Treatments including ertapenem and infliximab are administered intravenously; thus, establishing an infusion center within the clinic or having easy access and a partnership with a nearby infusion center can be of valuable assistance to patients.
Core Specialties for Referrals and Collaboration
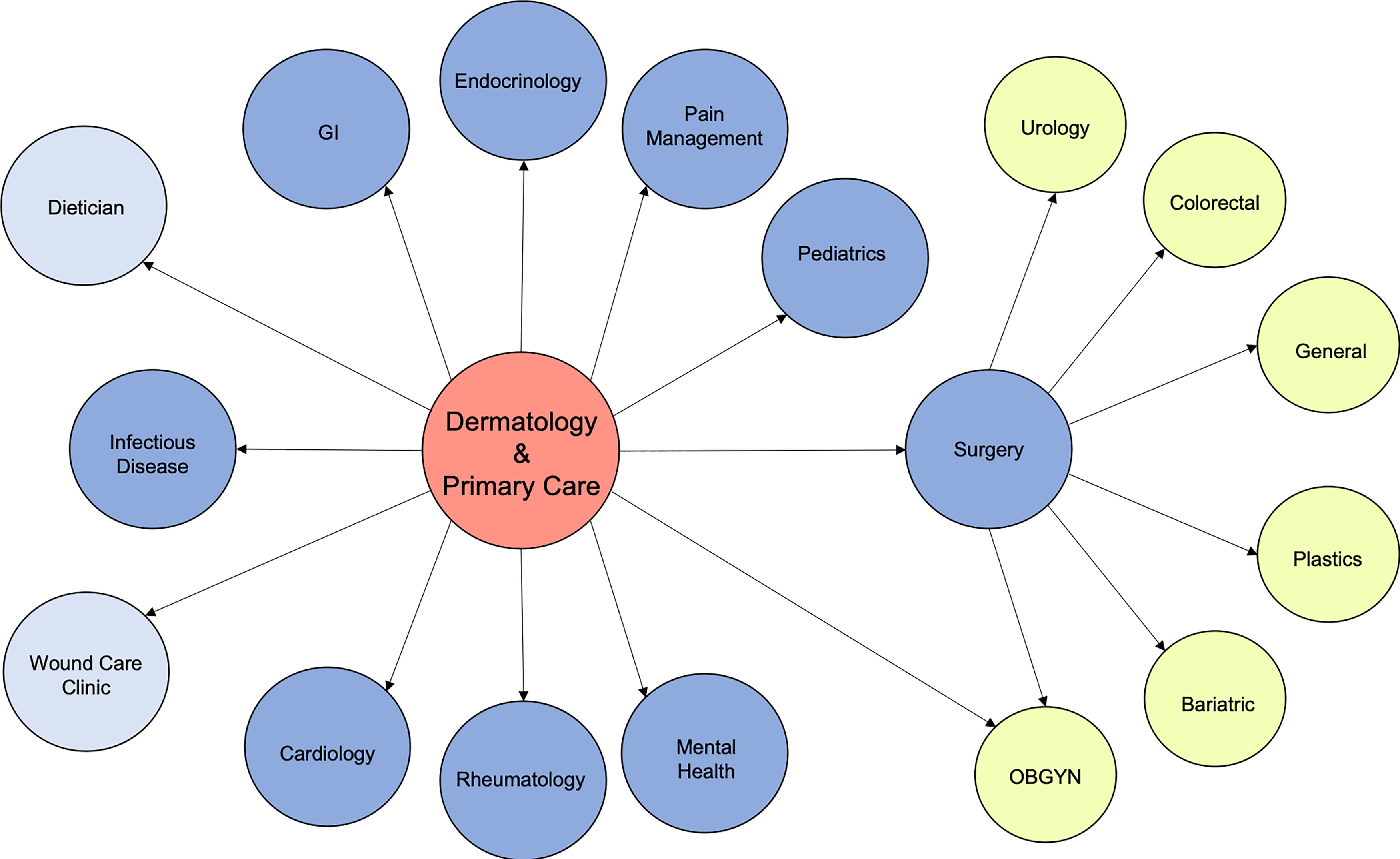
As previously stated, the management of patients with HS is often a multidisciplinary effort. HS is associated with numerous comorbidities and often requires input from multiple specialties ( Fig. 32.2 ). Given this fact, close collaboration is often required with colleagues within other specialties. Establishing these relationships for referrals and collaboration is essential. Compiling a handout for local physicians, medical staff, and patients with relevant contact information can be an invaluable tool. Comorbidities and systemic associations are discussed further in Chapter 8 .
Surgery
One of the most common specialties to help manage patients with HS is surgery. While dermatologists and surgeons are capable of performing many deroofing office procedures for HS, general and plastic surgeons are often tasked with performing large excisions of affected HS areas that require utilization of general anesthesia. In HS clinics, dermatologists and surgeons are a complementary combination to evaluate patients together in the clinic, if possible. Colorectal surgeons are often needed in cases with extensive buttock and rectal involvement. Urologic or gynecologic evaluation is sometimes needed for those with penile, scrotal, urethral, or vaginal involvement, or for those who have HS involvement near these areas.
Endocrinology, Weight Loss and Diet
Due to the fact that HS is associated with an increased risk for diabetes mellitus, metabolic syndrome, and polycystic ovarian syndrome (PCOS), consultation and referral to endocrinology for management of these comorbid conditions are often necessary. In addition, dietary modifications can help in the management of some of these disease states. Accordingly, referral to a dietician can be helpful. Some patients report that the avoidance of dairy and brewer’s yeast improves disease severity. Dieticians can make helpful recommendations regarding avoidance of these patient-specific dietary triggers. The prevalence of overweight or obesity in patients with HS may be greater than 75%, and as such, evaluation for bariatric surgery is sometimes warranted. Bariatric surgery can be beneficial for some patients with HS as improvement in the severity of the disease in one retrospective review was seen in 35% of patients after bariatric surgery.
Cardiovascular Disease
HS has also been linked to major cardiovascular events including myocardial infarction (MI) and stroke with a 23% increased risk compared to those without HS. As such, close collaboration between family practice, internal medicine, and cardiology is needed to evaluate and assess for the presence of modifiable risk factors and to screen for these comorbidities. In addition, the prevalence of smoking in patients with HS is between 70% and 75%. Thus, taking a thorough smoking history is recommended, and smoking cessation counseling by providers is encouraged.
Comorbid Autoimmune and Inflammatory Conditions
Rheumatology can be brought on board to help manage patients with HS who also have fibromyalgia, polymyositis, and ankylosing spondylitis, among others. Gastroenterology is often needed for the management of patients with HS who also have concomitant inflammatory bowel disease. Often, some of these diseases can be treated using the same immunosuppressive or biologic medications. Close contact and collaboration between specialties to come up with individualized treatment regimens are key to optimizing patient outcomes.
Antibiotic Management
Infectious disease is also an important referral specialty for those with HS. Oral antibiotics are an important component of the HS treatment armamentarium. Administration of some intravenous antibiotics, including ertapenem, require consultation with infectious disease colleagues to develop a collaborative management plan as well as to coordinate placement of vascular access lines for prolonged use. Concern for antibiotic resistance means that this treatment is typically reserved for more severe cases that have failed first-line treatments.
Obstetrics and Gynecology
Hormones affect HS; thus, many pregnant women with HS can experience improvement, no change, or worsening of the disease during pregnancy or in the post-partum period. A recent single-institution study of 202 pregnancies revealed that 34.7% of pregnancies ( n = 70) had worsened the severity of HS during pregnancy, 16.8% ( n = 34) had no change, 4.5% ( n = 9) had improvement, and 42.6% ( n = 86) were unknown. In addition, post-partum HS exacerbation was reported in 40.1% ( n = 81) pregnancies. Treatment of HS during pregnancy also requires special attention to avoid the negative effects of some medications on the fetus that could cause birth defects. For instance, tetracyclines and retinoids are contraindicated during pregnancy due to the risk for teeth discoloration and fetal anomalies, respectively. Thus, close collaboration between dermatology and obstetrics and gynecology (OB-GYN) is needed throughout pregnancy and in the post-partum period. In addition, OB-GYN physicians can aid in the early diagnosis of HS as well as the management of comorbid PCOS.
Pediatrics
HS can also be present in the pediatric population, and it has been suggested that HS in the pediatric population may be more severe than in the adult population. Thus, early intervention and close collaboration between dermatology and pediatrics to avoid progression and scarring are warranted.
Pain Management
Pain is a major factor that negatively affects patient quality of life in those with HS. Management of acute and chronic pain are both important considerations, and collaboration with pain specialists is often necessary. One or a combination of topical and/or oral analgesics, anti-inflammatories, opiates, and anticonvulsants can be used. There are no HS-specific pain studies or recommendations, and treatment is based on pain guidelines, expert opinion, and patient preference. Pain management is discussed further in Chapter 19 .
Mental Health
Lastly, and perhaps most importantly, mental health in patients with HS should always be evaluated. HS is a chronic, painful, and often debilitating and disfiguring disease, and as such has a huge effect on patient quality of life and mental health. HS is associated with depression and anxiety, and patients with HS also have a higher chance of committing suicide than those without HS. Patients should be screened and be referred for psychology/psychiatry services to treat any depression, anxiety, and suicidal thoughts/behaviors. Psychosexual health should also be considered as those with HS are at a higher risk for sexual dysfunction when compared to those without HS. Referral to a sex therapist who has experience treating patients with HS could be extremely helpful in select patients. Access to HS support groups such as Hope for HS ( https://hopeforhs.org ) or other chronic disease support groups also allows for a sense of community and the opportunity to express shared experiences and promote mental health. In fact, those participating in support groups have been reported to have lower levels of depression and anxiety as well as increased quality of life. These support groups can also provide resources and recommendations for therapists and mental health experts for patients.
Conclusion
In conclusion, establishing a successful multidisciplinary clinic for the treatment of patients with HS is a multifaceted endeavor. A basic treatment algorithm can guide an initial treatment approach. Customizing the clinic to meet the needs of the patient is central. Quality improvement projects to help enhance the clinic should always be considered. And finally, close collaboration with colleagues in other specialties is crucial.
References
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


