Abbreviations used
HS
hidradenitis suppurativa
IL
interleukin
Nd:YAG
neodymium-doped yttrium-aluminum-garnet laser
MetS
metabolic syndrome
IBD
inflammatory bowel disease
OR
odds ratio
SIR
standardized incidence ratios
QOL
quality of life
SD
standard deviation
SES
socioeconomic status
NAMCS
National Ambulatory Medical Care
NHAMCS
National Hospital Ambulatory Medical Care Survey
IPV
intimate partner violence
CD
Crohn’s disease
UC
ulcerative colitis
SCC
squamous cell carcinoma
US
United States
Prevalence of Hidradenitis Suppurativa in Skin of Color Individuals
While the overall US prevalence of hidradenitis suppurativa (HS), obtained through US claims data, has been reported to be 0.10% or 98 per 100,000 persons, HS disproportionally affects women (137 per 100,000), African Americans (296 per 100,000), and biracial (African American/Caucasian) (218 per 100,000) patient groups. In comparison, the rates of HS among white patients are closer to the overall reported US prevalence at 95 per 100,000 persons. Conversely, HS affects Asians, Pacific Islanders, Native Americans, Latin Americans, and Native Hawaiians at much lower rates, with a standard prevalence of 0.04%. However, these prevalence rates may be underestimations due to underdiagnosis and the inability to capture those who did not seek care in the healthcare systems included in the databases analyzed. Further, adult patients with HS may have symptoms for up to 7 years before diagnosis. Consequently, if the same is true among children with HS, then prevalence in younger age groups may also be underestimated.
Classical teachings have supported this claim that people of African descent have a higher incidence than those of European descent. However, the majority of previously published studies on HS report prevalence and incidence in a largely Caucasian cohort. Recently, additional retrospective studies have emerged supporting the classical teachings, demonstrating that African Americans appear to be more commonly affected and with higher severity of HS. The true prevalence of HS in the general US population may likely be higher due to limitations in diagnosis, underdiagnosis, misdiagnosis, and patient reluctance to seek treatment. This may be especially true in skin of color populations due to limited access to medical care, implicit biases, anatomical differences, genetics, and increased prevalence of lower socioeconomic status (SES) among these groups.
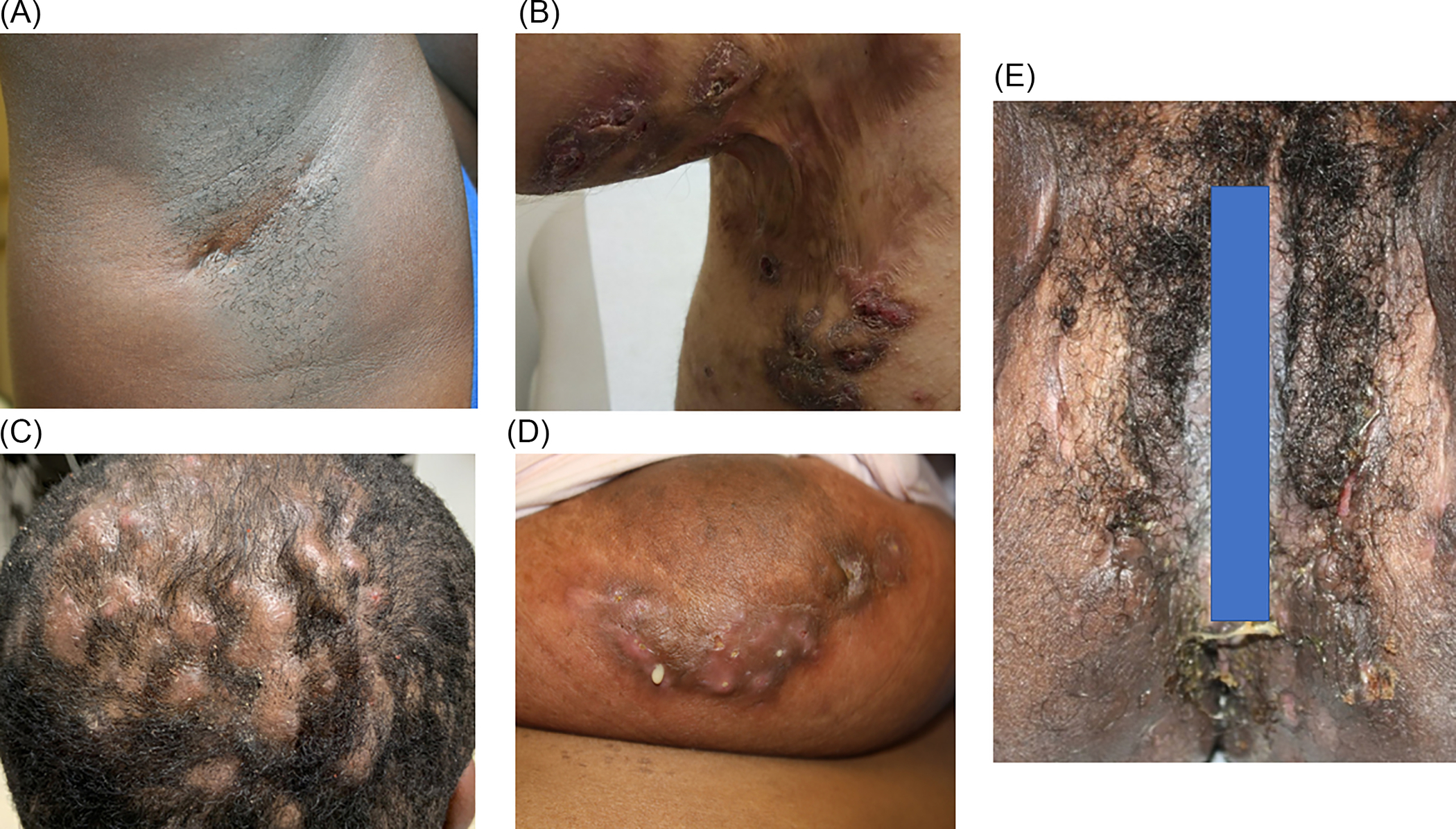
HS presents with painful, erythematous, and often malodorous abscesses, nodules, dermal tunnels, double- and multi-ended comedones, along with scar formation followed by hyperpigmentation in apocrine gland-bearing skin such as the axillae, inguinal, perianal, and perineal regions. Further, HS lesions in skin of color patients may be purplish in color, more hyperpigmented, and the erythema and tunnels may be more difficult to identify in comparison to Caucasian patients. Gentle palpation can be used to help identify them( Fig. 30.1 ).
Skin of Color Representation in Hidradenitis Suppurativa Clinical Trials
This discrepancy in reporting HS prevalence amongst skin of color patients also appears to extend to clinical trials. Using Clinicaltrials.gov and PubMed, Price et al. examined the race and ethnicity demographics in phase II and phase III HS treatment trials published from 2000 to August 2019. Fifteen trials were included in the analysis. Among these trials, 669 (68.0%) of the participants were Caucasian and 138 (14.0%) were of African descent. Asians, American Indian or Alaskan Natives, and Native Hawaiian or other Pacific Islanders comprised 29 (2.9%), 3 (0.3%), and 1 (0.1%) participants, respectively. Only 15 participants were reported as Hispanic, as only three trials reported ethnicity data. While these percentages may reflect the breakdown of the US population in terms of race/ethnicity, they do not reflect the disproportionate rates of HS in African Americans. The remaining 144 (14.6%) participants were recorded as “other/unspecified” (36 self-identified, 108 lacked race reporting). None of the trials included a sub-analysis of treatment efficacy based on race or ethnicity.
Adalimumab is the only currently approved systemic medication for the treatment of HS. However, clinical trials for adalimumab did not sufficiently examine the treatment response in patients with skin of color. One study was conducted solely in Caucasian and Romany individuals, while another study consisted of 80% to 85% Caucasians. Further, none of the trials reported the percentage of patients that were Hispanic/Latino or stratified the responses to adalimumab by race. The other systemic biologic agent trials for HS (e.g., etanercept, infliximab, anakinra, and ustekinumab) either did not report race or largely had a Caucasian population. Reduced enrollment in clinical trials by skin of color populations may be due to distance from clinical trial sites, lack of education regarding clinical trials, lack of awareness that clinical trials are available for the particular disorder, language barriers, and mistrust of researchers from historical experiences such as the Tuskegee Syphilis Study. Moreover, these results suggest that populations represented in clinical trials may not truly reflect the diverse patient populations affected by HS, and that these medications may only work in a subset of HS patients.
Light/Laser and Other Treatment Considerations
In HS treatment, there are differences in dosing for standard phototherapeutic options in patients with skin of color. In randomized controlled trials, typical settings used for the neodymium-doped yttrium-aluminum-garnet laser (Nd:YAG) were generally a 10-mm spot size with a 20-ms pulse duration and 40 to 50 J/cm 2 in patients with Fitzpatrick skin type I to III and a 35-ms pulse duration and 25 to 35 J/cm 2 in patients with skin types IV to VI. This treatment is discussed further in Chapter 25 . Carbon dioxide laser excision and marsupialization has also been shown to be an effective therapy for the management of Hurley Stage II or III disease. Notably, it has been our experience in clinical practice that the risk of keloid formation following the excision of HS lesions has rarely been seen. Due to this observation, the authors strongly suggest that this modality be offered to skin of color patients. Additional light-based treatment options for HS include photodynamic therapy (PDT) and intense pulsed light. However, these treatment modalities are not well-studied in skin of color HS patients and their general efficacy appears to be very limited.
Genetics and Anatomy
In a Dutch cohort of 846 HS patients, 283 (35.5%) were identified as having a family history of HS. Further, patients with a family history of HS were more often female, had a lower mean age of disease onset, and had longer disease duration. Familial HS proves to be autosomal dominant with mutations in genes ( NCSTN, PSENEN, PSEN1 ) that code for parts of γ-secretase, an enzyme that normally cleaves the Notch receptor involved in epidermal and follicular development and differentiation. Of note, these studies were conducted primarily in Chinese populations. Only one case report has been published identifying a mutation in the NCSTN gene in an African American family with HS. Further, a retrospective chart review of patients who underwent surgical treatment for HS was performed at the University of Illinois Medical Center. The results showed that 81.6% of patients who had surgery were African American, and African American women with axillary HS were more likely to have a recalcitrant disease with progressive symptomology over approximately nine years before surgical intervention.
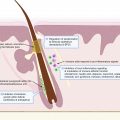
Older studies (pre-1965) found that patients of African American descent had larger, more numerous, and more productive apocrine glands than Caucasians. The scalp hair of African Americans has been examined, and cross-sections have shown that the hair shaft tends to be elliptical or flattened and spiraled or tightly curled in its tertiary structure. Moreover, the curled hair does not emanate from a straight follicle. Instead, the follicle where the hair is formed is just as curved as the hair itself. The hair shaft structure in Asian patients tends to be round in cross-section and relatively large in diameter. In comparison, Caucasian patients’ hair shaft structure appears to fall somewhere between those of Asian and African American patients. These results suggest that skin of color populations may have an anatomical predisposition for both HS and more severe forms of HS warranting further studies into genetic and anatomical variations and epigenetics in skin of color HS patients. Thus far, no ultrasound differences of hair follicles in skin of color patients versus Caucasian patients have been published.
Keloids
Individuals of African, Latino, or Asian descent appear to be at increased risk for keloids. In individuals prone to keloid formation, the chronic inflammatory lesions of HS may lead to keloid formation. It has been hypothesized that the same pathway underlying tissue destruction and scar formation in HS subsequently triggers keloid formation in these patients. HS has been associated with the upregulation of cytokines such as interleukin (IL)-1, similar to general keloids.
Previously, one case report existed of HS keloids being successfully treated with adalimumab. However, in 2019, a North American case series was performed consisting of 10 patients with keloid formation in HS wounds. Patient ethnicities were African, Asian, Middle Eastern, and White. The most frequently affected sites were the chest (6 out of 10 cases) followed by axillae, and the severity of HS ranged from mild to severe disease. Some of the patients’ keloids were either treated with intralesional injections of triamcinolone or received no specific treatment. Three of the 10 patients received adalimumab for the treatment of HS with subsequent reduction in both keloidal size and pruritus.
Treating a patient with both HS and keloids within the same area can be complex. In the setting of no residual HS inflammation, the keloids formed from HS scars may respond to traditional therapies such as intralesional corticosteroid injections. However, keloids that occur in chronically inflamed HS lesions first require treating the underlying HS inflammation. Intralesional corticosteroid injections have been used for the management of localized flares in HS. In 3 of the 10 patients mentioned above, patients who received adalimumab for their HS also saw a subsequent reduction in both keloidal size and pruritis. However, it cannot be said for certain whether the effects of the biologics were due to directly acting on keloids or whether it was due to early control of inflammation. Optimal treatment of patients with HS and keloids in HS scars requires further investigation, and currently, prevalence rates of keloids in HS scars are unknown. However, our anecdotal experience is that the keloidal-type lesions in areas affected by HS are amenable to surgery.
Comorbidities
There are a number of comorbidities associated with HS. A higher cardiovascular risk is associated with HS due to several factors, including metabolic syndrome (MetS), diabetes mellitus type II, and smoking. Endocrine comorbidities include diabetes mellitus and polycystic ovarian syndrome. HS has also been linked to inflammatory bowel disease (IBD) and spondyloarthropathy. A recent population-based study of 22,468 patients with HS in the Republic of Korea demonstrated an increased risk of HS patients having cancer overall, specifically higher rates of Hodgkin lymphoma, oral cavity and pharyngeal cancer, central nervous system cancer, nonmelanoma skin cancer, prostate cancer, and colorectal cancer. Moreover, HS patients experience significant mental health disease burden, have an increased risk of completed suicide, and are vulnerable to substance use disorders.
Metabolic Syndrome
HS is known to be associated with MetS and shares several major risk factors, including non-Caucasian race (African Americans and Hispanics) and female gender. African Americans and Hispanics are less likely to engage in regular exercise compared to Caucasians. Further, HS disease severity has been correlated with morbid obesity more commonly in patients with high versus medium disease burden (37% vs. 22%). Non-obese HS patients report more frequent HS remission in comparison to obese patients (45 vs. 23%), and in younger patients, HS onset occurs earlier in patients with comorbid MetS. Taken together, these findings suggest that African American and Hispanic HS patients are at greater risk for MetS, chronic HS, and more severe forms.
Inflammatory Bowel Disease
In a retrospective study of a single US tertiary medical care center, the prevalence of HS in patients with IBD was 0.7%, while the prevalence of IBD in patients with HS was 3.6%. Among the 93 patients with both IBD and HS (IBD-HS), 75 (80%) had Crohn’s disease (CD). When compared to controls with only IBD, the IBD-HS population had more women, African Americans, and higher rates of smoking. Further, in another retrospective cohort study using the National Inpatient Sample (NIS) 2004 to 2014, a total of 3,079,332 admissions with IBD were recorded, of which 4,369 had a concurrent diagnosis of HS. From this IBD cohort, 1,962,733 (64%) patients had a diagnosis of CD, while 1,116,599 (36%) of patients were diagnosed with ulcerative colitis (UC). IBD-HS patients were associated with 3732 cases (85%) of CD and 637 cases (15%) of UC. Compared to IBD-only patients, IBD-HS patients were significantly younger (mean age 39 [IQR: 28 to 49] vs. 51 [IQR: 34 to 66]; P < .001), more likely to be female (61.6% vs. 57.2%; P = .008), and African American (46.8% vs. 10.0%; P < .001); they were also more likely to be smokers, obese, and have diabetes mellitus, depression, and anemia. Overall, these two studies show that patients with IBD and HS are more likely to be African American than IBD patients without HS.
Squamous Cell Carcinoma
Lapins et al. found that statistically significant risk elevations were observed for nonmelanoma skin cancer in HS patients (5 cases; SIR, 4.6; 95% confidence interval, 1.5 to 10.7). As mentioned previously, a Korean cohort demonstrated an increased risk of HS patients having nonmelanoma skin cancer. The transformation of chronic HS to squamous cell carcinoma (SCC) is considered the most severe complication of HS but is an extremely rare phenomenon. The most important risk factor for the development of SCC in African Americans is chronic scarring processes and areas of chronic inflammation. Moreover, chronic scarring processes including ulcers, discoid lupus erythematosus, lupus vulgaris, granuloma annulare, osteomyelitis, and HS have been noted in 20% to 40% of cases of SCC in African American people. Therefore, any nonhealing ulcers or nodules adjacent to an area of chronic scarring or inflammation should be biopsied to exclude malignancy. In general, African Americans with SCC have a higher mortality rate than Caucasians. Currently, there are no studies that examine whether there are higher rates of SCC in African American patients vs Caucasian patients with HS.
Psychiatric Comorbidity
HS patients have higher quality-of-life (QOL) impairment than patients with psoriasis, acne, neoplasms, strokes, and heart transplant candidates, and HS has been shown to be associated with increased odds of depression, antidepressant use, anxiety, anxiolytic use, and suicidality. Further, depression was found to be more prevalent in those with higher disease burden than those with medium disease burden (52% vs. 35%). This has serious implications for African Americans and Latinos compared to Caucasians because they are already at risk for a wide range of psychosocial stressors. A study that oversampled African Americans and Hispanics/Latinos in relation to Caucasians found that major depression was most prevalent amongst Latinos (11%), followed by African Americans (8%), and then Caucasians (8%). The differences in depression rates are thought to be due to functional limitations, lack of health insurance, and lifestyle factors such as smoking and exercise, which varied amongst the racial groups. Rates of chronic major depressive disorder are higher in African Americans than Caucasians (57% vs. 39%), and African Americans were more likely to rate their depression as severe/very severe and more disabling. Given these findings, African American and Latino patients with HS may be at higher risk for developing depression and more severe forms of depression in comparison to the overall HS population.
In addition, there is increased mental health stigma in African American and Latino communities. Thus, if there is an underlying medical condition that is causing or exacerbating an individual’s mental health, treatment of that underlying medical condition is imperative since the patient may not seek treatment for their mental health. Further, in a study conducted to determine the incidence of long-term opioid use in previously opioid-naïve patients with HS, there was a 53% higher risk of long-term opioid use among patients with HS (OR 1.53, 95% CI 1.20 to 1.95; P < .001). Among patients with HS, a history of depression (OR, 1.97; 95% CI, 1.21 to 3.19, P = .006) was associated with higher odds of long-term opioid use. However, no association was found between race/ethnicity and increased risk of long-term opioid use among the HS patients. These finding should still be seriously considered in skin of color HS patients as well as other racial and ethnic groups who also suffer from depression.
Access to Adequate and Empathetic Care
Studies have shown that HS is associated with low SES, potentially because low SES is also associated with lifestyle factors such as smoking and obesity. Moreover, low SES is more prevalent in African and Latino populations, especially in the US. A recent retrospective analysis examined HS patients presenting to Montefiore Medical Center HS Treatment Center between January 2015 and November 2017. Patient SES was based on factor analysis from census block groups and a z -score reflecting SES deviation from the New York State mean. Demographics of 375 HS patients were analyzed. Females with low SES ( z -score ≤-1.00) were more likely to present with Hurley stage II/III disease (OR, 1.72; P = .049), and there were more African American patients in stage III than non-African Americans (50% vs. 28%, P < .001). African American patients were more likely to have stage II/III than others (OR 2.46, P = .0003). The median SES of HS patients was -2.3 standard deviations (SD). African American patients with HS demonstrated a median SES of -2.3 SD, while non-African American patients had a median SES of -1.6 SD ( P = .001). In summary, approximately one-third of HS patients were African American and had more severe disease and significantly lower SES.
Patients with low SES may have HS and more severe HS due to healthcare barriers. Conversely, patients with HS may have low SES due to pain, drainage, and medical comorbidities leading to lost employment and educational opportunities. Low SES makes it difficult for families to buy fresh produce, and their neighborhoods may prevent them from exercising outside for safety reasons, thereby contributing to obesity and metabolic syndrome. In addition, an important barrier to optimal HS treatment is proper wound care management. The cost of the dressings can be mitigated by insurance coverage, but some insurance plans do not cover the expense of wound dressings.
In 2016, data from the 2005 to 2011 National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) were analyzed to assess factors that were predictive of outpatient visits for HS. Non-Hispanic, non-Latino patients were more likely to experience clinic visits for HS than Hispanic/Latino patients (OR 5.49, P = .002). The difference in patient visits for HS observed in Latinos and Hispanics may not represent a true difference in disease burden within this population but may reflect decreased access to healthcare resources.
A recent study examined the demographic patterns and geographic patterns of inpatient hospitalizations for HS in the United States. African American patients accounted for almost half (47%) of HS patients discharged. Patients from zip codes with the lowest quartile for income accounted for 41% of HS hospitalizations. Nearly one-third (29%) of HS discharges from 2012 through 2014 were from the South Atlantic census division (Delaware, Maryland, Virginia, West Virginia, North Carolina, South Carolina, Georgia, Florida, and the District of Columbia). In contrast, the New England division and the Mountain division each accounted for only 3% of HS discharges. The study suggested there may be a significant link between the geographic distribution of HS discharges, the racial distribution of African Americans, and the prevalence of adult obesity across the US. Further, a recent study demonstrated that urban zip codes with higher percentages of African Americans tended to have fewer dermatologists, while urban zip codes with lower percentages of African Americans tended to have more dermatologists. In the areas with a higher representation of African Americans, dermatologists were responsible for more people per provider than recommended (> 25,000 people/dermatologist). Hence, limited access to care and a higher number of comorbidities may contribute to more severe disease, necessitating higher hospitalization rates amongst African Americans.
Sisic et al. found that individuals with HS were significantly more likely to report being victimized by intimate partner violence (IPV). Moreover, ethnic minority women (i.e., Black/African American, Hispanic/Latina, Native American/Alaska Native, Asian American) are disproportionately affected by IPV. According to the 2010 National Intimate Partner and Sexual Violence Survey, non-Hispanic Black and Native American/Alaska Native women reported higher prevalence rates of lifetime IPV (43.7% and 46%, respectively) compared to non-Hispanic White women (34.6%); the rate for Hispanic women was slightly higher (37.1%). These disproportionate rates have also been consistently documented in multiple US studies. Screening for IPV should be incorporated into the care of HS patients, especially those with skin of color.
Conclusion
Despite a growing database of literature demonstrating a higher prevalence of HS in skin of color patients, especially in African Americans, few large-scale studies exist focusing on HS in skin of color. Significant differences may exist in treatment response for different racial/ethnic groups; however, clinical studies have primarily been performed in the Caucasian population. Greater representation of skin of color patients is needed in HS clinical trials. Skin of color populations may have forms of HS that are more severe and less responsive to treatment due to genetic variations, warranting further studies into genetic and anatomic variations and epigenetics in skin of color patients. Further, African American and Latino patients are at greater risk for MetS and more chronic and severe forms of HS. They may also be at higher risk for other comorbidities of HS, including IBD, SCC, and depression exacerbated by lower SES and higher rates of IPV. There is a crucial need for improved access to effective and culturally appropriate care for skin of color patients with HS and future research focusing on skin of color patients is needed to fully elucidate HS and its burden in these patient populations.
Note: In writing this chapter, we used the terminology presented by the National Institutes of Health regarding racial and ethnic categories. However, we would like to bring awareness that these terms, while acceptable in scientific literature, may not always be the preferred terms of these communities. For example, Latino and Latina are gender specific, so Latinx may actually be the preferred term to include individuals of the LGBTQIA (Lesbian, Gay, Bisexual, Transsexual, Queer, Intersex, Asexual) community. In all permissible instances, we have tried to be respectful and thoughtful of these considerations.
References
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


