• Photography is an essential tool to objectively document patient conditions, evaluate physical deformities, plan treatment approaches, and assess surgical outcomes.
• In plastic surgery, clinical photography accomplishes two goals primarily: first, documentation of preoperative conditions and postoperative surgical results, and second, recording of surgical procedures and techniques.
• It is always beneficial to understand the basic mechanics of a camera, in order to obtain high quality facial images that are accurate, representative, and consistent to permit reliable analysis.
• While the technology acquiring facial images is evolving and the contents of clinical photography are expanding, the basic concepts and principles remain the same.
• Contemporary clinical photography, for facial imaging particularly, extends from 2D photography to 2D videos, 3D surface images, and even emerging 4D images.
• Digital cameras, computers, and technological advancements in both hardware and software play a critical role in shaping contemporary clinical photography.
• Clinical needs in plastic and reconstructive surgery drive and accelerate further developments in the surface imaging technology.
Clinical photography in plastic surgery
Plastic surgery differs from most other fields of medicine in that it is a visual specialty. Plastic surgeons can and must see the changes in patients that they have surgically created. Photography, since its invention, has allowed plastic surgeons to capture preoperative, perioperative, and postoperative moments because such visual information can be challenging to accurately document with words, measurements, or even sketches. Embodying the saying “A picture is worth a thousand words,” photography serves as one of the fundamental objective means in clinical practices along with observation, examination, and measurements.
Clinical photography as a branch of medical photography emphasizes documentation of clinical presentations, in particular the facial appearances of patients, as seen in the clinic. In contrast to radiographic images such as computed tomography (CT) and magnetic resonance imaging (MRI), which acquire volumetric information, photography acquires surface images of patients. Being noninvasive and physically harmless to patients, photographs can be quickly obtained and archived for further analysis should a reexamination be needed without inconveniencing the patient to return.
Today clinical photography is an essential tool for surgeons and clinicians to document conditions, evaluate deformities, plan treatment approaches, and compare changes to assess treatment outcomes. Usually, plastic surgeons, nurses, or clinical photographers take pre- and postoperative photographs in a controlled office or studio setting following standardized protocols. The image quality is essential: photos and images have to be accurate, representative, detailed, consistent, and free of misleading information that may cause misinterpretation.
In plastic surgery, clinical photography also serves a role in documentation and demonstration of surgical procedures or techniques. Surgical images in forms of photos or videos are taken by surgeons in the setting of an operating theater to capture crucial moments of a procedure with interests in the operated region. It is important to strike a delicate balance between minimizing interference to the operative procedure and obtaining quality images or videos. Usually a quick, simple, flexible, and creative approach works better than a standardized protocol.
The progressive use of clinical photography in plastic surgery has been governed by the technologic advancements throughout history. From the first medical image produced in 1845 by Alfred François Donné using a daguerreotype, the technologic advancements of conventional clinical photography in plastic surgery have not only refined the methods available to the plastic surgeon, but have also invigorated the profession through technology. The advent of digital cameras and the subsequent digital video camcorders has transformed clinical photography by eliminating the chemical processing of negative and positive films in darkrooms, providing immediate results, and ensuring quality digital images with the abilities to archive, store, retrieve, and share.
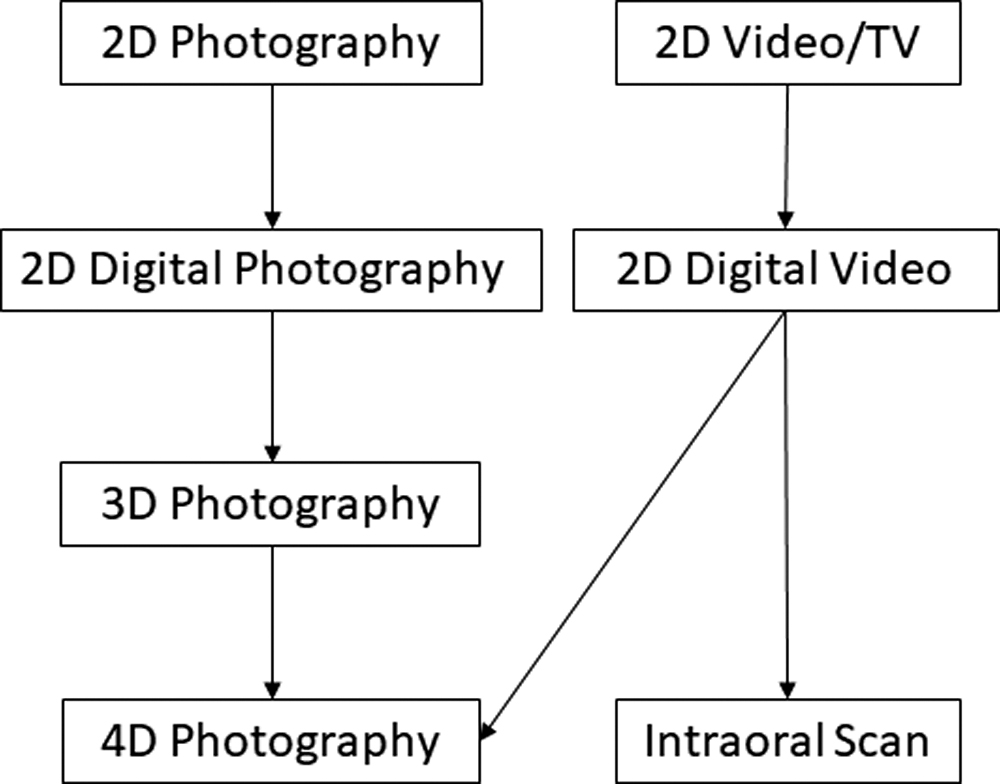
The emergence of three-dimensional (3D) surface image acquisition systems specifically designed for plastic surgery has permitted clinical photography to expand beyond the scope of traditional two-dimensional (2D) photography. From the image acquisition perspective, clinical photography can be accomplished through various modalities, which includes, but is not limited to, 2D photos, 2D videos, nasopharyngeal endoscopy, 3D surface images, intraoral scans (IOSs), and emerging 4D surface images, as shown in Fig. 8.1 . While most of current 3D surface imaging systems are large in dimension and require dedicated studio space, emerging devices tend to be more portable, and even smartphone compatible without additional equipment. Accompanied development is the integration of image acquisition, reconstruction, analysis, and surgical treatment simulation, shifting the paradigm of clinical photography in plastic surgery. As photographic technology evolves, it is imperative for plastic surgeons to not only become familiar with and incorporate new developments into one’s clinical practice but also continuously refine and provide guidance for facial imaging technology to further advance and develop to meet the clinical needs.
Along with the expansion of its means and contents, clinical photography today has a wide variety of applications, such as medicolegal documentation, patient counseling, treatment planning, and medical education, in addition to documentation, treatment outcome, and publication. It is also used for advertising in many practices via television, social media, and the Internet. Thus ethical and legal considerations arise especially for facial images. If the patient is recognizable as most are from facial images, the clinical photograph is considered protected health information (PHI) and is regulated by the Health Insurance Portability and Accountability Act (HIPAA). Mandated to protect the privacy and confidentiality of patients, plastic surgeons and clinicians must obtain patient permission and consent for use beyond the intended clinical purpose. Most patients are usually willing to have their pictures, including facial images, presented in professional conferences attended by health care providers or for publication in scientific journals for the medical science audience. The same patients may not be willing to have their photographs, especially of their face, advertised in magazines, newspapers, television, social media, or posters at the surgeons’ clinics. Standard practice is to obtain consent from the patient or surrogate before any specific use.
In the following sections, we will discuss the quality of clinical photography, review the history of medical photography, introduce basic concepts, discuss the development and clinical application of the major modalities in clinical photography, and conclude with a comparison of the major surface imaging modalities and a discussion on the technology development trends of clinical photography and their potential impact on clinical practice and patient care.
What accounts for a quality clinical photograph or image of a face?
Photographs reflect the care and attention to detail exhibited in the plastic surgery practice; thus, one should always strive for the highest quality attainable. What accounts for a quality clinical photograph or image of a face? The answer may lie in the simple example of pre- and postoperative photographs for comparison. To allow the surgeon and the patient to evaluate the surgical results, and possibly present those results to peers at medical conferences or in medical journals, “It is, therefore, essential that pre- and postoperative photographs be taken in exactly the same manner so that the only visible differences are the changes resulting from the surgery.” In this sense, high-quality clinical photographs have to be accurate, representative, consistent, and standardized.
Accurate
Accurate photographs are essential in plastic and reconstructive surgery practice. It is imperative that clinical photographs clearly show every detail, wrinkle, and minor deformity that the surgeon desires to correct. “In this respect, clinical photography differs from portrait photography. The purpose of portrait photography is to present the subject in the most favorable way, whereas the purpose of clinical photography is to portray the subject in the most accurate way. Most of studio photographer’s techniques may be counterproductive at best and deliberately deceptive at worst.” Cover-up, such as makeup, should be avoided, and distractive objects such as jewelry should be removed or kept to a minimum.
Representative
Representative photos convey the message efficiently. Specifically, they should focus on the region of interest (ROI) and the moment of interest (MOI) that are pertinent to the deformity that needs to be corrected. For example, intraoral photos are essential for patients who undergo orthodontic treatment or orthognathic surgery but may not be necessary for patients who undergo rhinoplasty. However, one should always take the entirety of the face and the head into consideration and include necessary background information in the clinical photography. For instance, it is useful to include the natural head position in facial images for patients with craniofacial malformations. As a compromise among different requirements, it is generally better to err on the side of caution and capture more information than less because loss of time-sensitive, critical information may not be easily acquired again. After obtaining medical photographs and images, it is imperative to properly format the images to attain the highest-quality products. Images should be oriented in the same direction that a surgeon would view them, cropped to only the essential aspects of the photograph, and organized in a way that is easy to archive, share, and retrieve.
Consistent
Consistent clinical photographs are critical for comparison of the pre- and postoperative conditions. The acquisition process should be consistent to ensure uniformity among the photos. Clinical photographers, nurses, or assistants must take every photograph the same way every time. These details include, but are not limited to, lighting, background, magnification, distance between the camera and the patient, clothing, and posing of the patient, as well as the format, orientation, and cropping of the image after its acquisition.
Standardized
While consistency suffices for comparison of the same patient at different times, standardization of the clinical photographs is essential for meaningful comparisons among individuals with similar craniofacial conditions that may be documented in different institutions and clinics. A set of standardized clinical photographs for specific craniofacial conditions is necessary for communication among health care providers from different institutions and clinics and in educational materials, presentations, and journal publications. This can be achieved through standardization of the cameras, settings, environments, and step-by-step guidelines, as seen in multicenter studies.
Two-dimensional photography
2D photography, or photography, as it is usually called, is described as the projection or reflection of a 3D object onto a 2D plane or the projection of a 3D surface image of the 3D object without the perception of depth.
Historical review
In 1839, Louis Daguerre invented the process of creating images on silver-plated copper called daguerreotype, and William Henry Fox Talbot developed a process of creating permanent negative images called calotype in 1840. Using a daguerreotype, Alfred François Donné produced the first medical image in 1845. Such negative–positive film technique was later refined by George Eastman, the founder of Eastman-Kodak company, who replaced the photographic plate with paper and film in 1884. , Earlier in the mid-1900s, fadeless color photo documentation was introduced to plastic surgery by Percy Hennell, a clinical photographer who worked alongside two of the most influential plastic surgeons of the century, Harold Gillies and Archibald McIndoe. Hennell contributed over 500 photographs of burn reconstruction patients to The Principles and Art of Plastic Surgery by Gillies and Millard in 1957. In 1955, Sir Harold Gillies stated that the greatest advancement in plastic surgery to date was the use of photography in medical applications. Advances in technology and digital photography led to higher resolution, greater memory capacity, smaller cameras, and lower costs. Around the year 2000, digital single-lens-reflex (DSLR) cameras replaced the conventional 35-mm film cameras in most medical photography. The digital camera not only eliminates the chemical process to develop negatives and print in a darkroom, but also allows for immediate viewing and evaluation of the images, which enables one to examine the image quality, perfect their techniques, eliminate unsatisfactory pictures, and retake while the patient is still present without additional cost. The ability to transfer the image directly from the digital camera to the computer allows one to archive, retrieve, and share images rapidly with ease. Furthermore, the digital camera technology opens the door for consolidating 2D photography and 2D videography onto developing multicamera systems, such as 3D and 4D surface imaging systems, in the era of powerful personal computers and accessible Internet. The digital camera is thus one of the corner stones of contemporary digital technology.
Basic photographic concepts
Regardless if one uses digital cameras or classic film cameras, the basic photographic concept remains the same. It is always beneficial to become familiar with the mechanics, concepts, and terminologies of a camera. All cameras rely on reflected light from the subject, which travels through the lens and creates an image on a medium, either film in a traditional camera or electronic chip or charge-coupled device (CCD) in a digital camera.
The medium’s sensitivity to light is quantified by the ISO speeds. Films with different ISO speeds are available. One may need different films for different lighting conditions when taking a photo. The digital camera simplifies this as its CCD can function at the equivalent of several ISO speeds often from ISO 100 to ISO 1600, allowing photographs to be taken in a variety of conditions. In most digital cameras, this change in ISO setting is automatic, whereas more sophisticated cameras allow the photographer to specify the ISO setting manually.
The amount of light striking the medium is referred to as exposure, which depends on two parameters. The first parameter is the size of the hole in the lens, called the aperture of the lens, and is expressed as a number called the f-stop . The f-stop number is inversely proportional to the size of the lens opening; that is, f/2.8 is a much larger opening than f/16 and therefore lets more light travel through during a given time. The second parameter is the length of time that the light shines on the medium, which is determined by how long the shutter stays open. This is called the shutter speed and is expressed in seconds. Most shutter speeds are between 1/30th and 1/1000th of a second. The faster the shutter speed, the less light reaches the medium. Thus, a photograph taken with a shutter speed of 1/500th of a second will be darker than one taken at 1/60th of a second, with all other settings being identical.
The lens, a key component of a camera, converts the reflected light from an object or a scene to a small region, a point, in theory, where the medium is located. The focal length of the lens is defined as the distance between the lens and the medium, and the distance between the lens and the object is set to be infinite. Adjustment of the distance between the lens and the medium can be either manual or automatic. In clinical photography, the lens, and thus the camera is optimized and preselected.
A combination of parameters, mainly the f-stop number, shutter speed, and ISO number, comprises of the settings of a camera. The selection of such settings depends on the desired effects and environment as well as personal preference. The primary effect is the depth of field which describes how much distance, from front to back is in focus given the lens has been adjusted properly for clear images to be created on the medium. For clinical photography, a large depth of field is preferred so that the entire subject is in focus. The higher the f-stop number, the larger is the depth of field the camera will provide. Clinical photographers generally prefer to use a high f-stop of f/8 or greater for facial images.
Camera settings have been automated as different modes in digital cameras, which are predefined for certain desired effects and environment. Some examples are sport, portrait, landscape, snow scene, and macro. While such predefined settings are easy to use and suitable for certain applications, surgeons usually prefer some degree of control. For example, surgeons may prefer the aperture priority mode which allows the user to choose a specific aperture value while the camera selects a shutter speed to match. This mode can easily provide a consistent depth of field, an important consideration when taking medical photographs. Aperture priority mode with the “Macro” setting on can be helpful for intraoperative photography when the camera is positioned close to the subject.
A digital image, either acquired via a digital camera or digitized from a traditional 2D photo via a device, such as a scanner, is a numeric representation of a 2D image. It has a finite set of digital values called picture elements or pixels, which is the smallest element in an image. The digital image contains a fixed number of rows and columns of pixels. Camera resolution is measured in megapixels or millions of pixels; both image file resolution and monitor resolution are measured in either pixels per inch (PPI) or pixel dimensions such as 1024 by 768 pixels, whereas printer resolution is measured in dots per inch (DPI). Monitor resolution is determined by the number of pixels the monitor can display, and its optimal resolution is the actual number of physical light-emitting pixels on the display.
Applications of two-dimensional photography
Two-dimensional photographs of the face
A typical set of photographs includes six images, which are frontal view, left oblique or quarter (1/4) view, right oblique or quarter (1/4) view, left view, and right view, as shown in Fig. 8.2 . The patient is seated and relaxed with a neutral facial expression as well as a smiling expression.