Fat grafting represents the most important new addition to surgical procedures to rejuvenate the orbit since the inception of the “blepharoplasty” technique. Traditional blepharoplasty procedures do not always address the changes that occur with age in the orbital area and can actually degrade the appearance of the eye. Fat grafting allows treatment of age-associated loss of periorbital volume not addressed by traditional blepharoplasty procedures. Fat grafting is an artistically powerful method to rejuvenate the periorbital orbital area that often provides a more healthy, fit, youthful, and sensual appearance than traditional blepharoplasty procedures.
Key points
- •
Traditional blepharoplasty procedures do not always address the changes that occur with age in the orbital area and can actually degrade the appearance of the eye.
- •
Fat grafting represents the most important new addition to surgical procedures to rejuvenate the orbit since the inception of the “blepharoplasty” technique.
- •
Fat grafting is an artistically powerful method to rejuvenate the periorbital orbital area that often provides a more healthy, fit, youthful, and sensual appearance than traditional blepharoplasty procedures.
- •
Periorbital fat grafting is easier and faster to perform than “septal reset” and eyelid fat transpositioning and provides the opportunity for comprehensive improvement of the entire orbital region, not just spot filling of the tear trough.
- •
Fat grafting is often more important to rejuvenating the periorbital areas of the secondary blepharoplasty patient than traditional eyelid surgery.
The aging orbit and the need for fat grafting
Why perform periorbital fat grafting? Why not just perform traditional blepharoplasty? The answer to these questions lies in the multifactorial origin of periorbital aging and the fact that fat is predictably lost from the periorbital area and the orbit and adjacent areas often become hollow as one ages. Acknowledging this, and recognizing the components of the aging change of the periorbital area and appreciating the underlying anatomic abnormalities, is essential to recommending appropriate treatment and the planning of proper surgical repair. Careful analysis will reveal that most patient problems seen in the aging periorbital area fall into the following categories ( Box 1 ).
- 1.
Forehead ptosis
- 2.
Eyelid skin excess
- 3.
Fatty accumulation and fat “herniation”
- 4.
Levator attenuation and dehiscence
- 5.
Canthal laxity
- 6.
Atrophy
Our traditional surgical procedures allow treatment of the first 5 changes. Fat grafting allows us to treat atrophy—an important new element in creating natural and attractive periocular appearance and something we could not do in the past.
Patients primarily concerned with surface aging of their periocular skin may not require blepharoplasty surgery and may achieve the improvement they desire through salon care and dermatologic surface treatments of their periorbital skin. These treatments include skin peels, intense pulsed light and broadband light treatments, laser skin resurfacing, and various cutaneous laser and other treatments designed to remove or reduce “age spots,” skin wrinkles, and other age-associated skin surface imperfections.
Patients primarily concerned with palpebral skin excess, fatty accumulation and fat “herniation,” relaxation and/or dehiscence of ligaments and musculoaponeurotic structures, and loss of youthful periocular contour achieve little, if any, improvement if surface treatments of the skin only are used. These patients require formal forehead lift and blepharoplasty procedures to reposition ptotic tissue, excise excess tissue, and surgically reinforce weakened ligamentous and musculoaponeurotic structures if these problems are to be properly treated and an attractive and natural appearing improvement is to be obtained. The misapplication of surface skin treatment to problems of forehead ptosis, eyelid skin excess, fatty accumulation, and weakening of ligamentous/musculoaponeurotic structures to eyes that have lost youthful shape and optimal function will produce smooth lid skin with no improvement in contour.
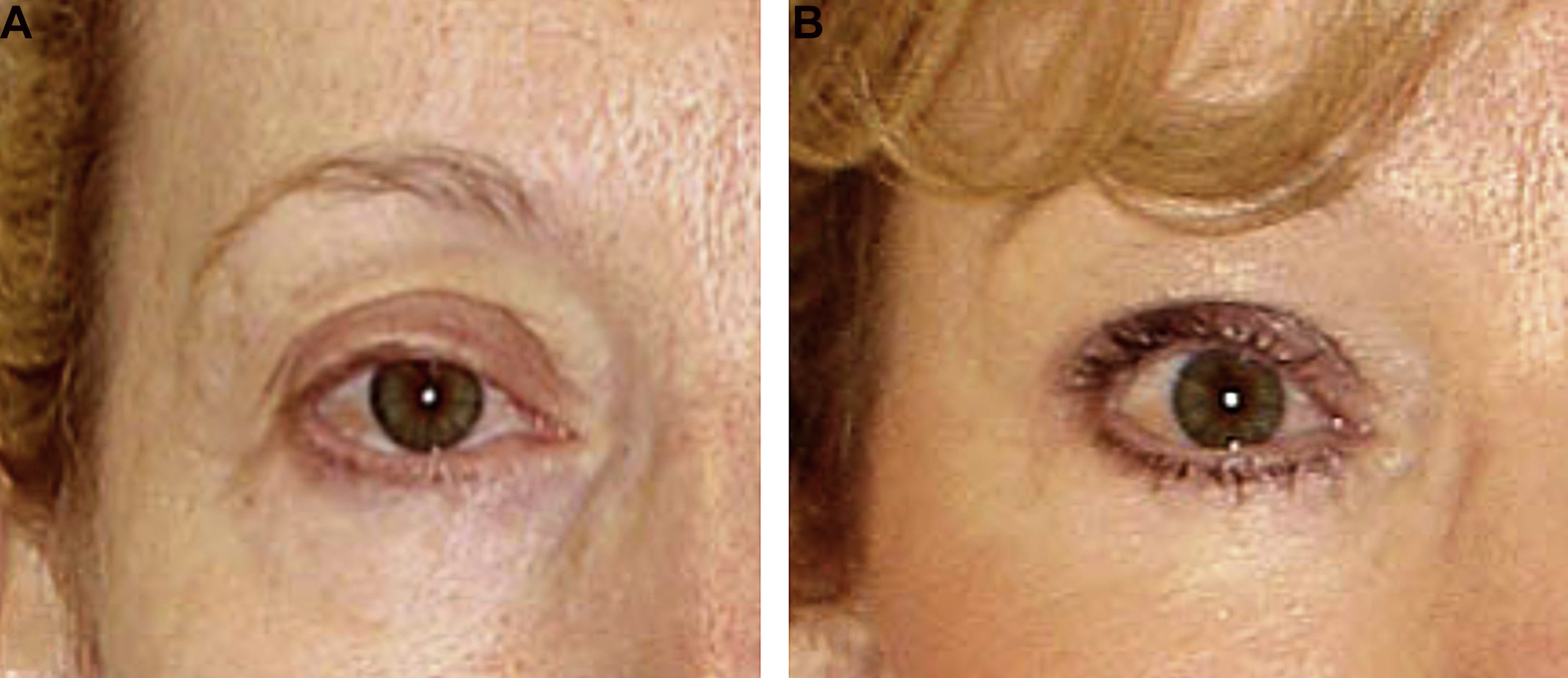
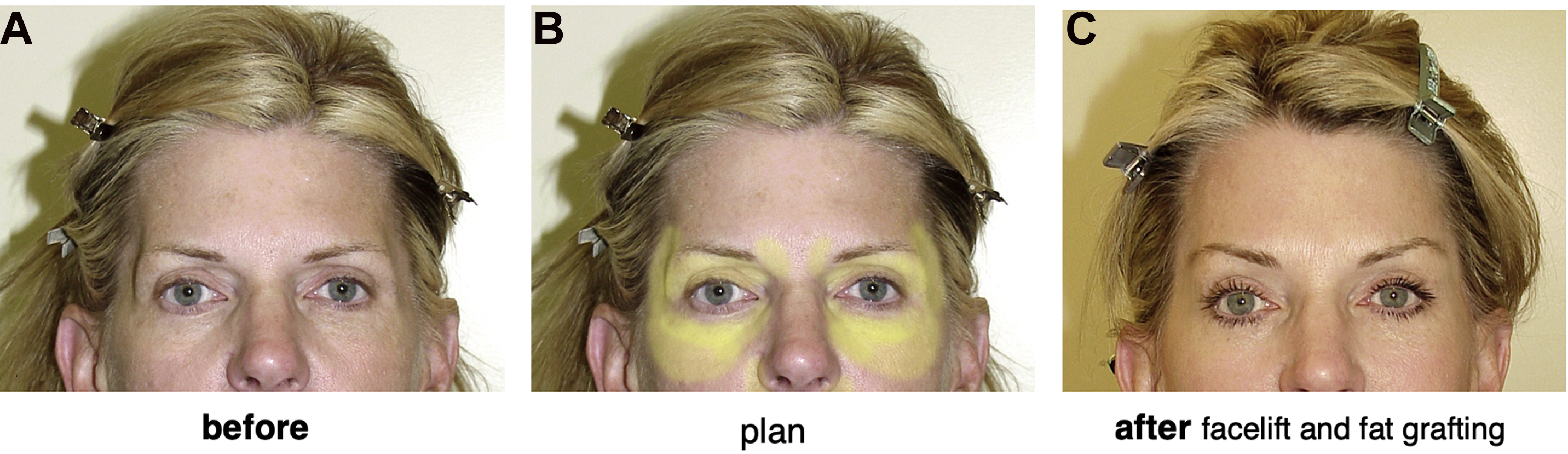
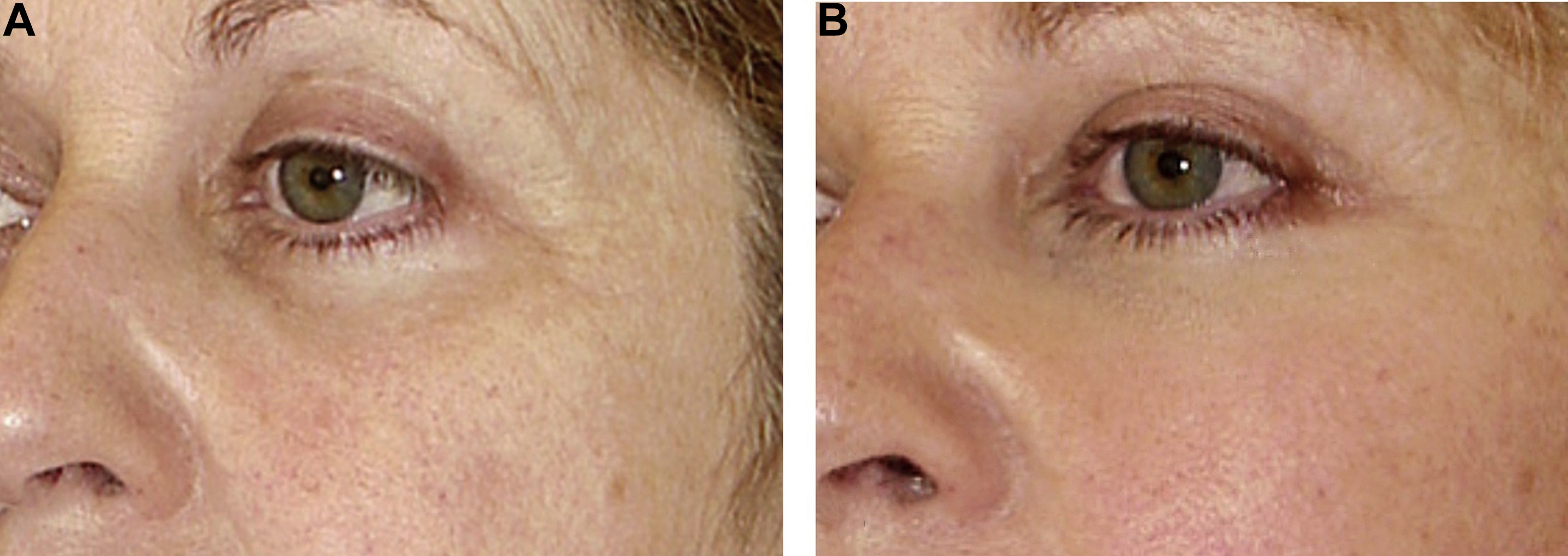
Patients with significant periorbital atrophy and age-associated hollowing and loss of periorbital volume will generally achieve suboptimal improvement from both surface treatments of periorbital skin and traditional blepharoplasty procedures. Smoothing skin will not hide an aged, gaunt, or ill appearance due to loss of periorbital fat, nor will removing tissue from already depleted orbital areas create natural and attractive periocular contours. Restoring lost periorbital volume by fat grafting is a powerful technique that is acknowledged by many surgeons engaged in treating the aging eyelid as the “missing link” in periorbital surgery and the most important advance in periorbital aesthetic surgery in several decades or more. Properly performed, the addition of fat to a periorbital region that has atrophied due to age or disease can produce a significant and sustained improvement in appearance unobtainable by traditional eyelid surgery ( Fig. 1 ).
What does the young eye really look like, what should our priorities be in rejuvenation of the periorbital area, and how can we best meet those aesthetic goals?
Simply stated, the young eye is clear, smooth skinned, neatly creased, elongated with a slight canthal tilt, and aesthetically framed by a well-positioned and appropriately shaped eyebrow. The hallmark of the young, attractive orbit is fullness , and we must ask ourselves “do our traditional blepharoplasty procedures produce results that look like these?” ( Fig. 2 ).

Fig. 3 shows a group of patients who have previously undergone blepharoplasty procedures. Are these really good results? Do these eyes seem youthful? Healthy? Attractive? Rejuvenated? Surgeons seeking to rejuvenate the eyelids must ask themselves “should we be removing or adding fat to achieve the most aesthetic result?” Should a blepharoplasty be more than a traditional partial blepharectomy? Do we need to rethink our approach to our blepharoplasty procedures? Can fat grafting help us achieve better outcomes?

If lid fullness is good, why not just use filler?
Fillers have certain advantages and are a viable alternative to periorbital fat grafting. Fillers have helped patients and surgeons understand volume loss as part of the aging process. They are nonsurgical, have a quick recovery, are long-lasting in orbital area, easily adjustable, and reversible (hyaluronic acid gel [HAG] products). These advantages must be weighed against disadvantages including that they require ongoing maintenance and that the treatments are time-consuming for busy patients, uncomfortable or painful, expensive, can be uneven or unnatural, and can precipitate a Tyndall effect. Over time patients often get “filler face”—an overfilled, heavy, unfeminine, “old,” and unattractive appearance. Many patients will also develop “filler burn-out” and come in requesting something that produces a more long-lasting and natural appearance. Perhaps the biggest disadvantage and lost opportunity of filler is its lack of “stem cell” tissue effects.
Why not just transpose eyelid fat?
Why not just transpose eyelid fat or perform a “septal reset”? These procedures are technically difficult, time-consuming open surgeries that entail a long recovery and carry a significant potential for irregularities and serious problems and complications. More importantly, only limited fat is typically available and these procedures largely treat the “tear trough” only. No improvement is obtained in lateral orbit, cheek, midface, temple, and upper orbit.
Advantages of periorbital fat grafting
Fat grafting allows surgeons to treat atrophy and improve outcomes over traditional excisional procedures in which tissue is removed. It comprises a volumetric rejuvenation —a new dimension for surgeons seeking to rejuvenate the periorbital area. It is autologous and provides for comprehensive treatment of the entire orbital area—not just the eyelids. Unlike nonautologous fillers, fat produces long-lasting and sustained improvement with a stem cell regenerative effect.
Volumetric rejuvenation, tissue integration, and stem cell effect
Fat grafting provides previously unavailable advantages for the surgeon rejuvenating the periorbital area by providing a means to obtain volumetric rejuvenation—a new and different means to improve periocular and facial appearance and a new dimension for surgeons to work in. Before fat grafting, surgeons performing blepharoplasty procedures were largely engaged in exalted technical exercises focused on what they could remove. Fat grafting provides a means for us to look at surgical rejuvenation of the orbit more broadly and appropriately and at how we can best create a truly youthful, healthy, and attractive appearance.
Unlike injectable fillers, fat is autologous, integrates with facial tissues, and becomes a part of the face, promoting a more natural appearance during facial movement, avoiding a Tyndall effect, and producing a sustained and long-lasting improvement. In addition, mounting scientific evidence now supports the often-cited clinical observation that fat injections actually induce an improvement in facial tissue quality through a “stem cell” effect and when performed in the periorbital area may achieve rejuvenation in the true sense of the word.
Drawbacks of fat injections
Performing periorbital fat grafting in conjunction with blepharoplasty has disadvantages including the learning curve associated with any new procedure, the time spent and needed to harvest fat, increased postoperative edema, a longer period of recovery, uncertain graft take, and the potential for problems and complications such as asymmetries, lumps, and irregularities. In addition, patient and surgeon misconceptions must be overcome, including the misguided belief of some that injected fat can migrate or fall, that fat injections will make the face ‘‘look fat,’’ or that it does not last.
Identifying the patient who needs periorbital fat grafting
Areas in need of treatment vary from patient to patient, and planning fat grafting procedures requires looking at the face more as a “sculptor” and less as a “tailor” as we have done in the past. Any area that is treatable with nonautologous injectable fillers is potentially treatable with fat grafting, including, but not limited to, the temples, forehead, brow, glabella, radix, upper orbit (“upper eyelid”), lower orbit (“lower eyelid”), cheeks, midface, and “tear trough”, and experience with fillers is a useful point of reference for planning fat additions to the face. A key element in restoring a harmonious and youthful appearance is for the surgeon to look beyond spot rejuvenation of the eyelids and to consider the entire periorbital area (temples, forehead, cheeks. midface) as an aesthetically integrated whole.
Perhaps the best way to decide where fat is needed is for the surgeon to study their blepharoplasty outcomes and identify areas where the procedure has fallen short. Usually the biggest shortcoming for the experienced surgeon is the failure to replenish lost volume, and the areas in need of treatment will be obvious.
Examining nonsmiling photographs of patients when they were younger are very helpful and provide a way to gain an appreciation of volume loss in the periorbital area and its contribution to aging changes in the orbital area. Old photos are also very helpful in educating patients as to how their orbital area has changed with age and in explaining the need for fat grafting. In almost all cases old photos of prospective patients taken when they were younger show a full upper and lower orbit, full midface and cheek, and a palpebral skin fold that rests only a few millimeters from their lashes. After thoughtful review over time one gains a deeper appreciation of periorbital (and facial) atrophy and the desire to correct it ( Fig. 4 ).
Periorbital fat grafting applications
How can fat grafting help surgeons rejuvenate the periorbital area? What can the fat be used for and where should the fat be injected?
Some of the ways fat grafting is used to improve orbital appearance and blepharoplasty results are discussed in the following section.
Cheeks
Fat grafting the cheek enhances a patient’s facial shape, proportion, and cheek projection; corrects age-associated loss of cheek volume; and thus improves periorbital appearance ( Fig. 5 ). Often fat grafting can rival or even exceed the improvements obtained when Terino malar, Binder submalar, and combined malar–submalar shell style cheek implants are placed (see Figs. 1 , 5-7 , 13-17 see also patient examples 1–5). In many instances fat grafting results in a softer more natural appearing, integrated cheek than cheek implants provide and produces a softer and less harsh appearance.

How Atrophy of the Cheek and Midface Affects the Appearance of the Lower Eyelid and Its Relevance in Procedures to Rejuvenate the Periorbital Area
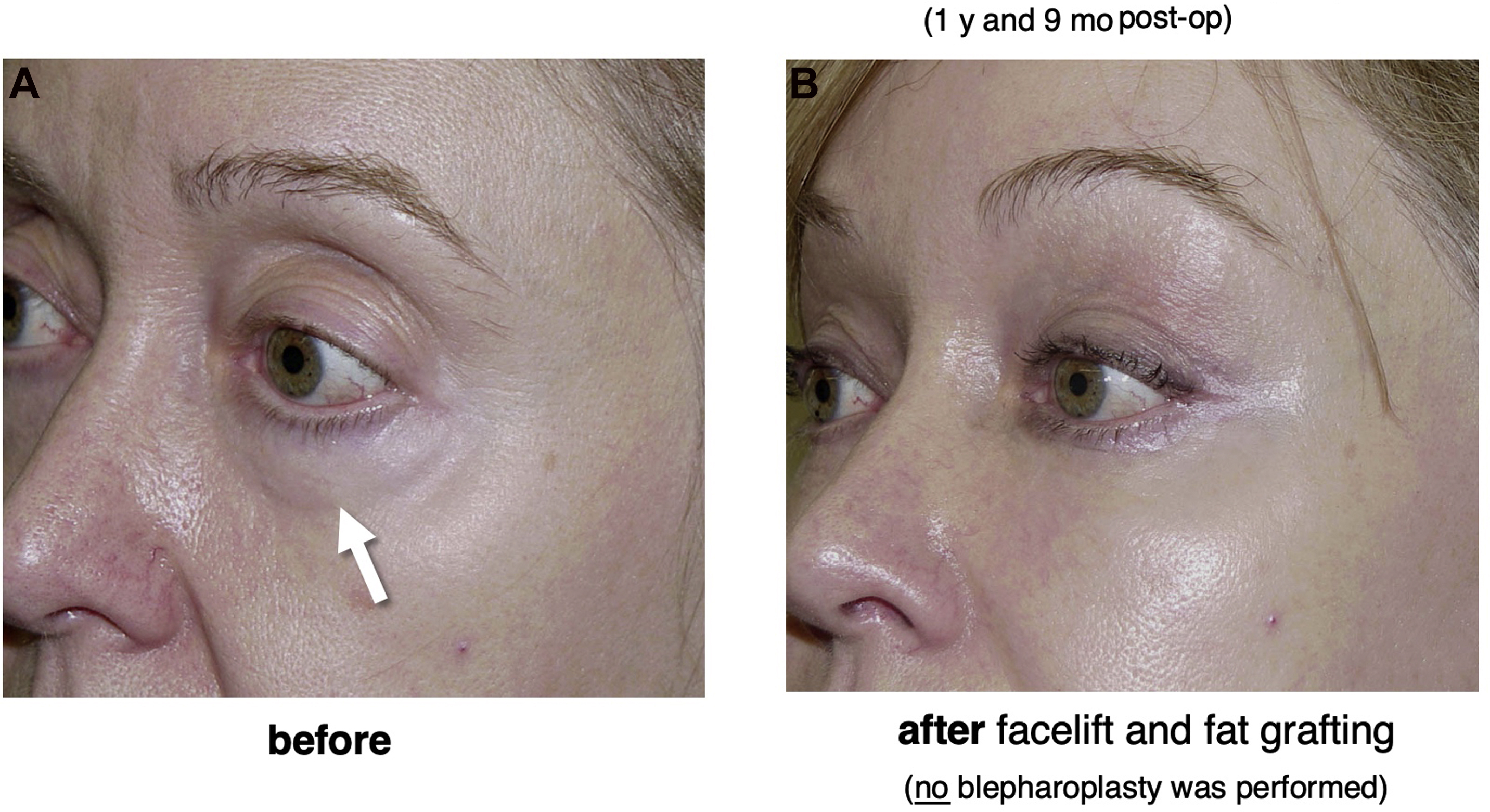
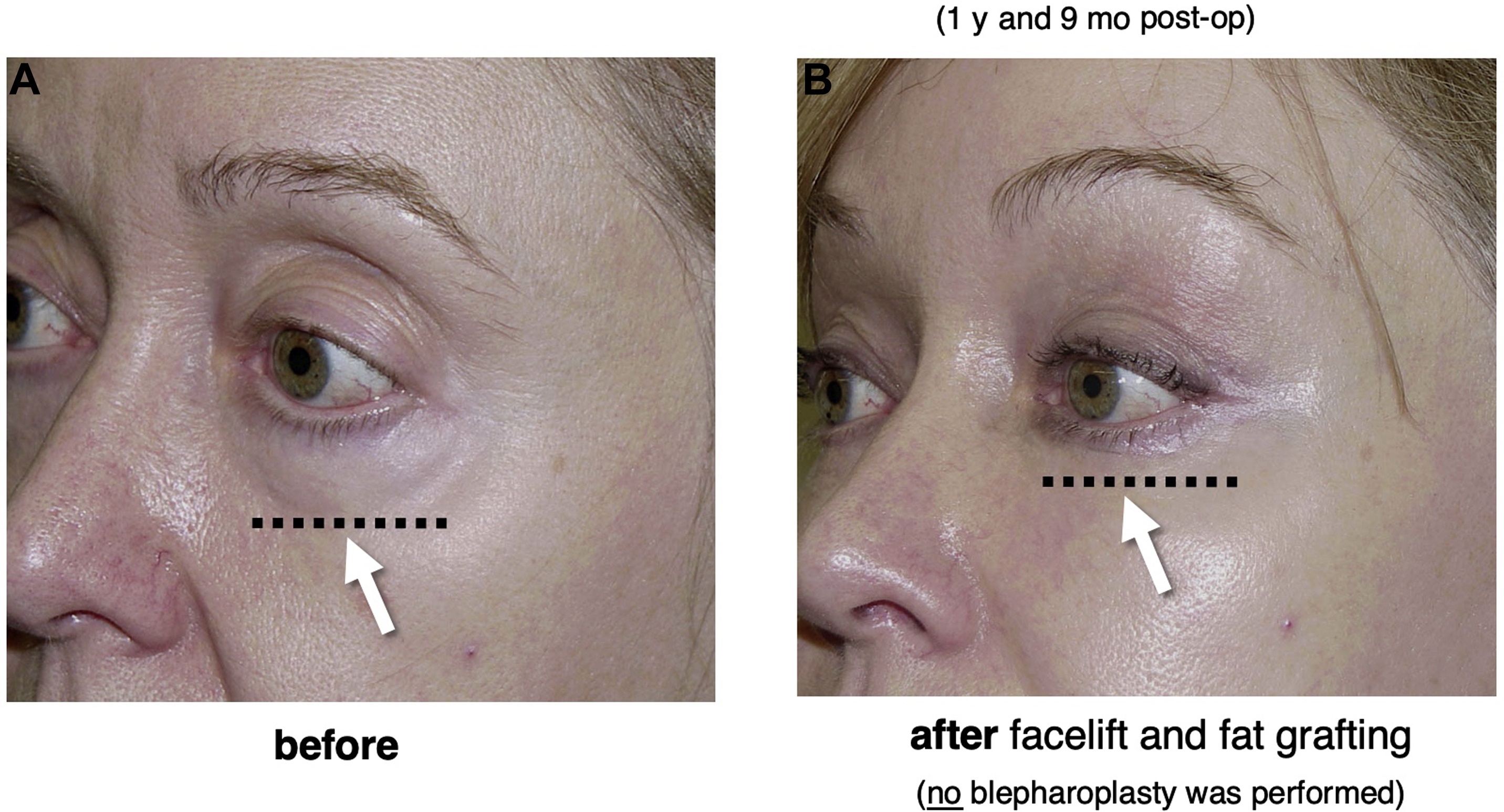
As the cheek atrophies, the lower eyelid orbital fat (“fat bags”) becomes more exposed and prominent in a process known as pseudoherniation . Removing lower eyelid fat in such circumstances as is often done in traditional blepharoplasty procedures, can create a hollow, elderly, and even ill “nursing home eye” appearance and a low-lying lid–cheek junction. A better strategy for many patients is to reconstitute the cheek with fat grafts and integrate the pseudoherniated fat with the cheek, rather than removing it, raising the lid–cheek junction to create a smooth and more youthful transition from the lower eyelid to the cheek ( Figs. 6 and 7 ).
Temples
Temporal hollowing is a consistent marker of one entering their 40s that is readily improved with fat grafting ( Fig. 8 ). Even skillfully performed eyelid surgery results in marginal improvement in overall orbital and upper facial appearance if the outcome of blepharoplasties is viewed against the background of a hollow, elderly and hard-appearing, bony, atrophic, empty temple. Restoring lost volume in the temples is arguably an important and essential part of contemporary “blepharoplasty” procedures performed by surgeons willing to look beyond the eyelids.
Fat grafting the temples is important to facial shaping and is typically sought by surgeons with a sharp aesthetic eye for detail in their facelift procedures. The ideal youthful, attractive female face has an inverted oval shape that with aging typically changes to be more rectangular and bottom-heavy one as the lower face, jowl, and jawline sags. Temporal atrophy and hollowing contributes to facial rectangularization, and when advanced a “peanut” facial shape results. Although a well-performed facelift corrects the lower facial squareness, temporal filling by fat grafting provides a wider intertemporal distance producing an inverted oval shape. Seen from this perspective, temporal filling comprises much more than simple filling of the temporal hollow or even more than a comprehensive rejuvenation of the eyelids and orbital area, it provides a more youthful, feminine, and beautiful appearing facial shape.
Upper orbit/“upper eyelid” area
Whether the result of illness, aging, or an overzealous previous surgical procedure, filling the hollow upper orbit can produce a remarkable rejuvenation of the upper eyelid and eliminate an unnaturally hollow and elderly appearance sometimes referred to by patients as “nursing home” or “owl eyes” ( Figs. 9 and 10 ).
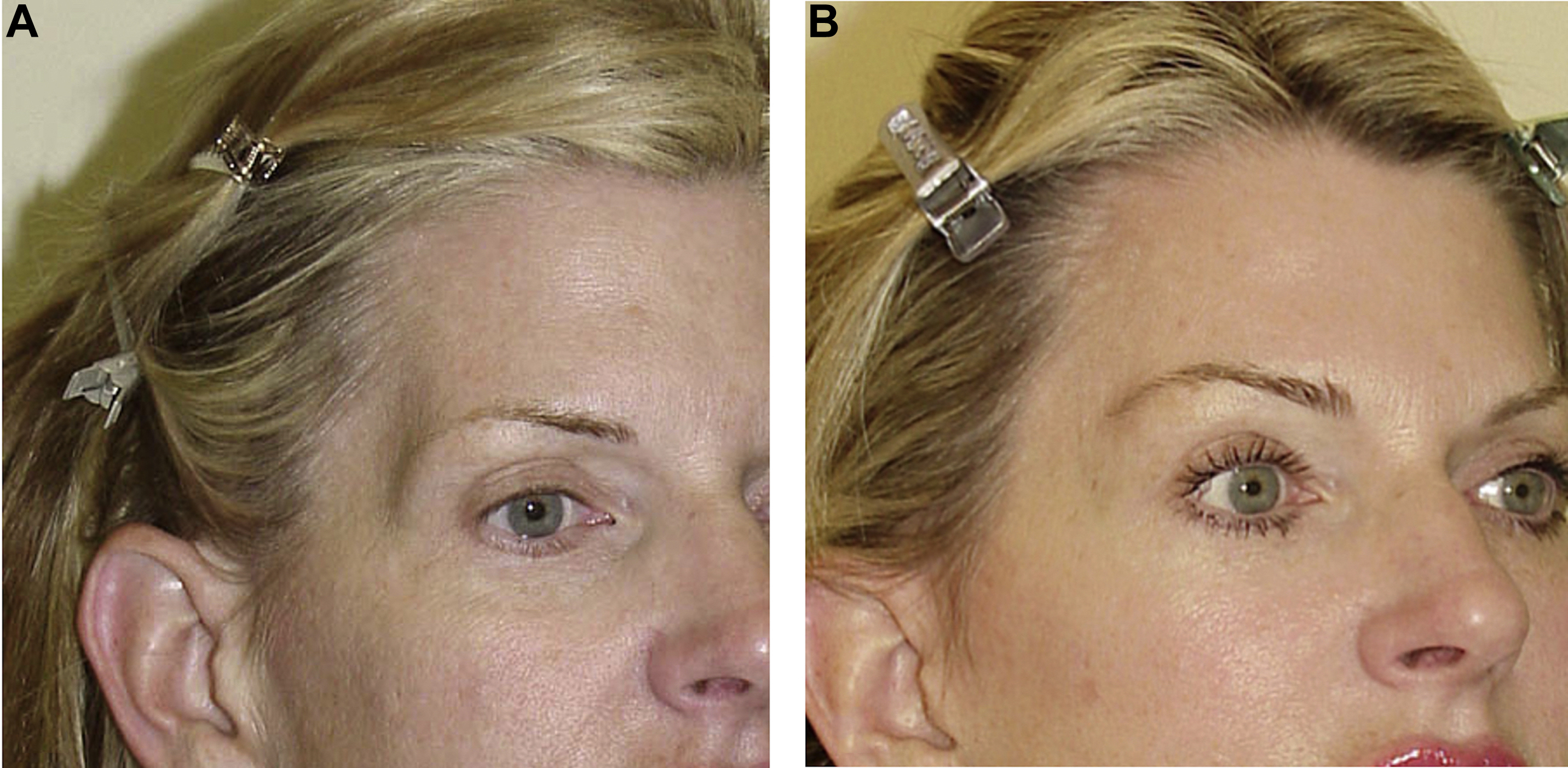
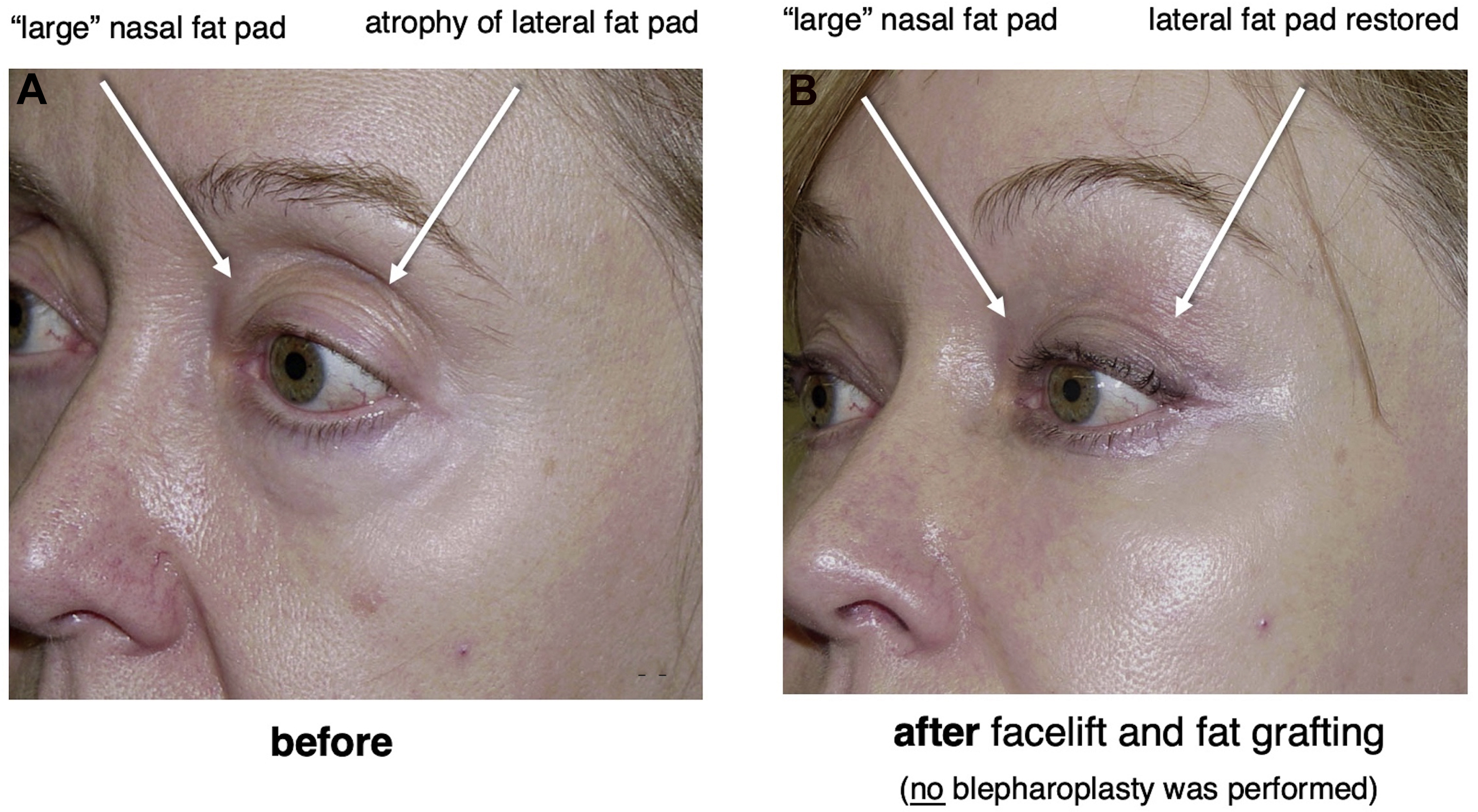
Pseudoherniation of the upper eyelid nasal fat pad
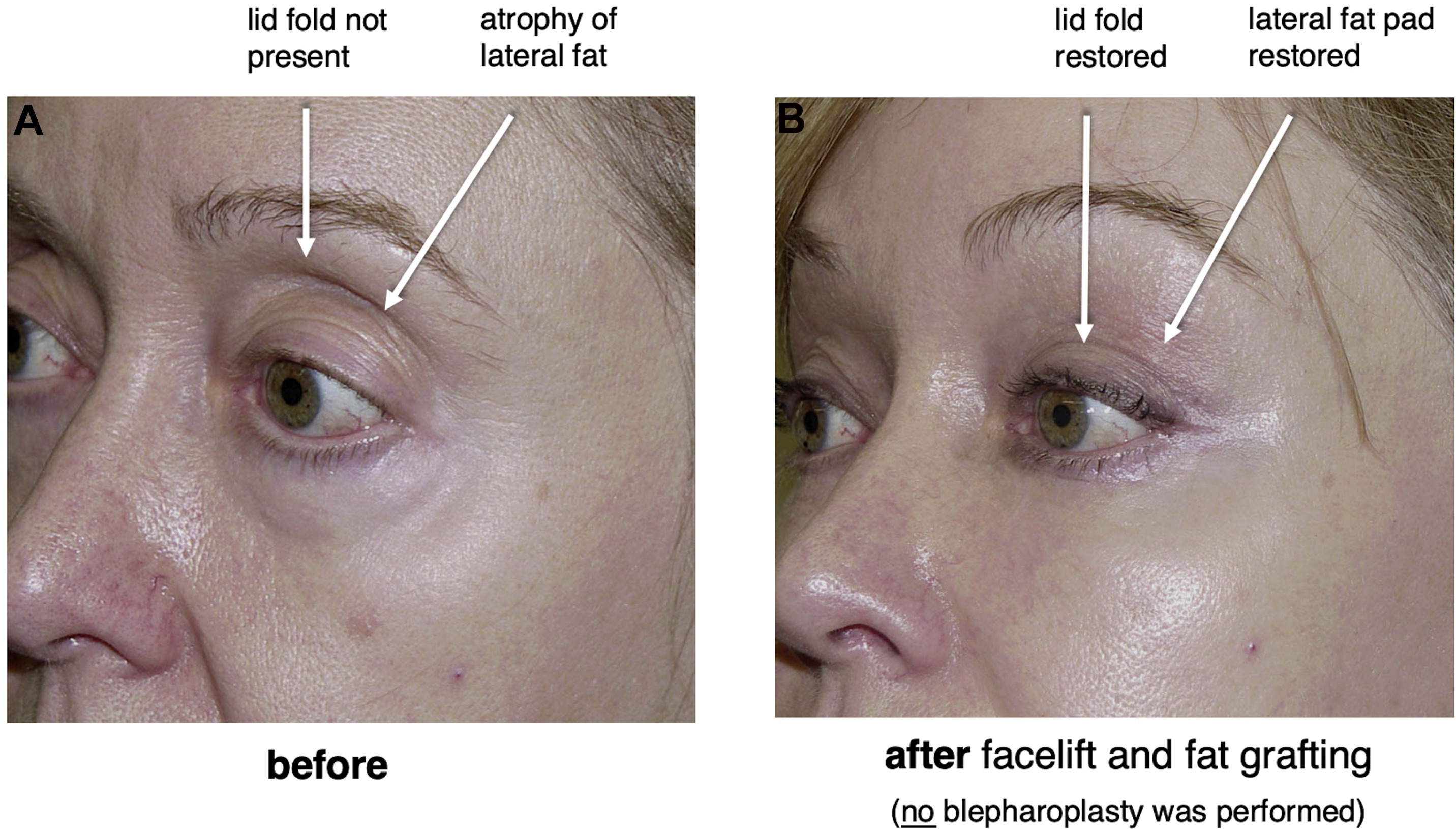
As the temporal fat pad of the upper eyelid atrophies, the nasal fat pad becomes more exposed and prominent—a sequence of events known as pseudoherniation . Removing fat from the nasal compartment in such circumstances as is traditionally taught usually creates a hollow, elderly, and unhealthy appearance or exacerbates such an appearance if already present. A more appropriate and attractive rejuvenation of the upper orbit is obtained under these circumstances when the atrophic lateral fat compartment is refilled and restored by fat grafting ( Fig. 11 ). In most cases the problem is not that the nasal fat pad has grown. It is that the temporal fat pad has atrophied.
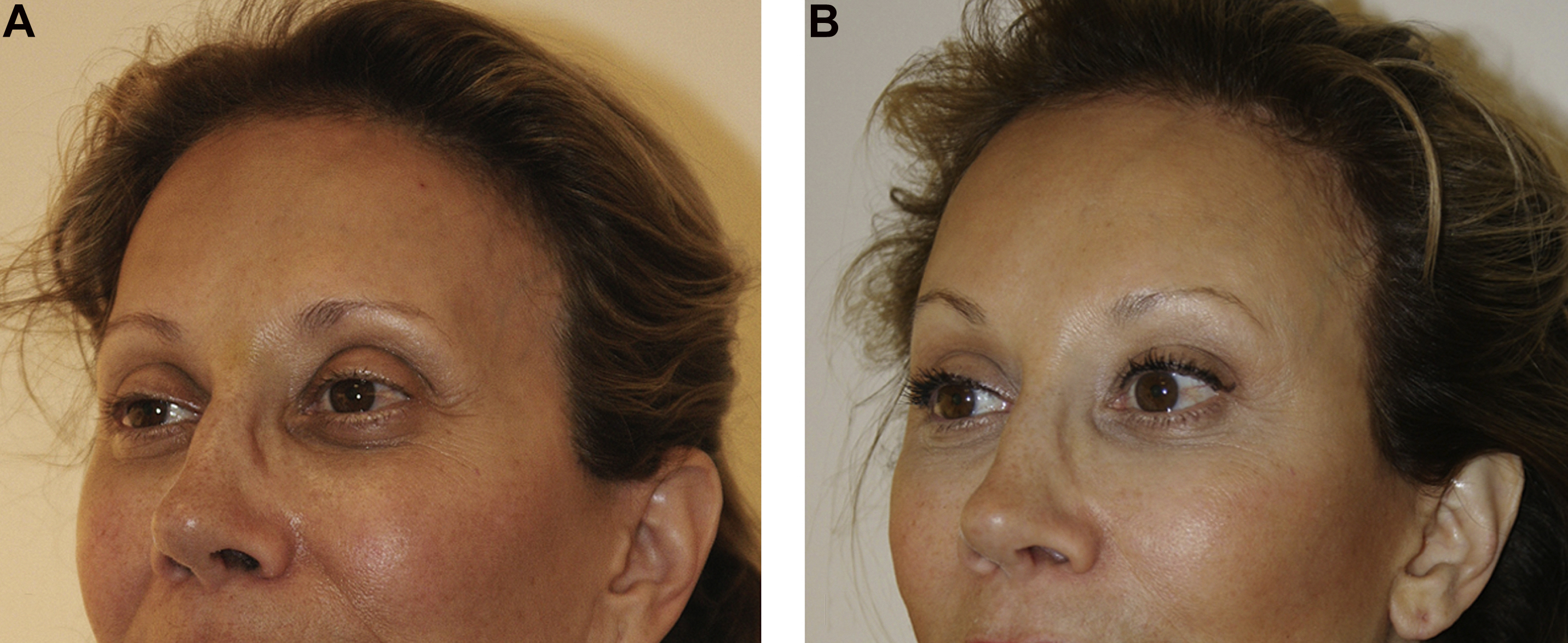
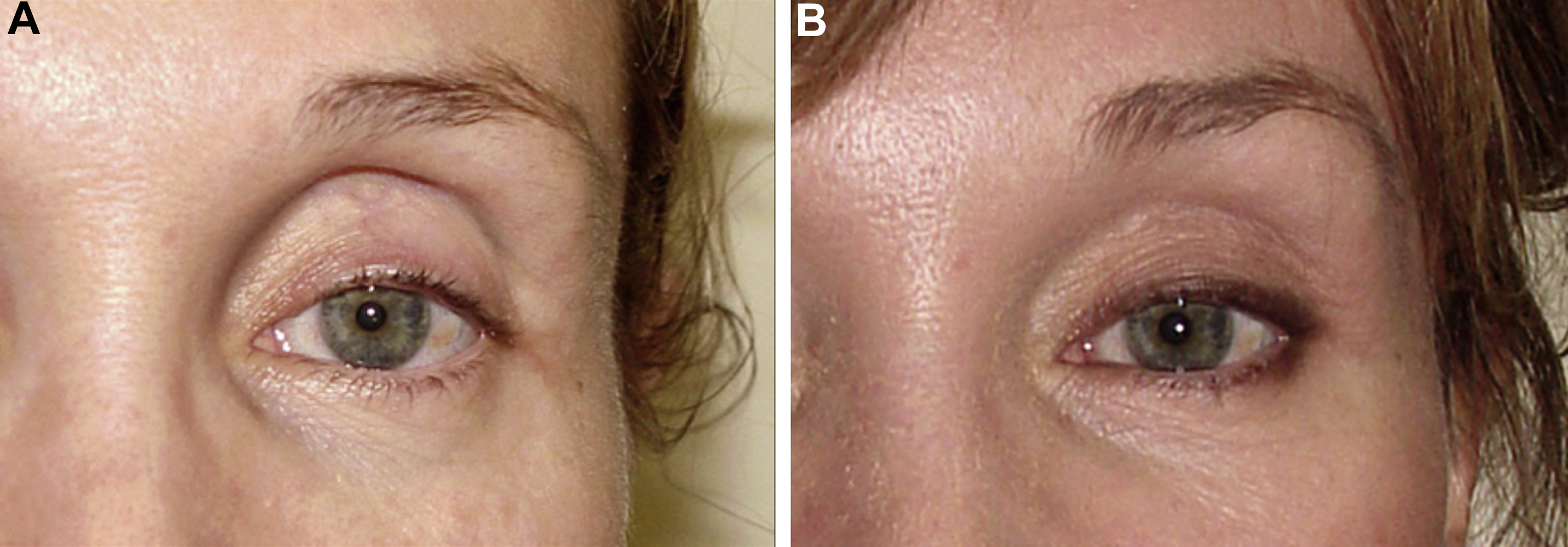
Restoration of the upper eyelid palpebral skin fold
As the temporal fat pad of the upper eyelid atrophies, lid skin is retracted into the upper orbit obliterating the normal palpebral skin fold. Removing fat from the nasal compartment as is traditionally taught accentuates a hollow, elderly, and unhealthy appearance and does nothing to restore the normal palpebral lid skin fold, essential to a youthful, healthy, and attractive appearance. A more appropriate and attractive rejuvenation of the upper orbit is obtained when the atrophic lateral fat compartment is reconstituted by fat grafting. When the upper orbital volume is restored, upper eyelid skin retracted up into the upper orbit preoperatively descends to form a youthful and natural appearing palpebral lid skin fold ( Fig. 12 ).
Lower orbit/“lower eyelid” area
Fat grafting the infraorbital (“lower eyelid”) area is in some ways analogous to augmenting the upper orbit, and the artistic payoff is very high if the procedure is carried out correctly ( Fig. 13 ).
Fat grafting the infraorbital area allows correction of age-associated atrophy and hollowness that lends the face an ill or haggard appearance; “shortens” the apparent length of the lower eyelid; and produces a youthful, attractive, and highly desirable smooth transition from the lower eyelid to the cheek that is generally unobtainable by traditional lower eyelid surgery, fat transpositions, “septal resets,” midface lifts, free fat grafts, and other procedures.
“Tear trough”
Where the infraorbital area ends and the nasojugal “tear trough”, midface, and cheek areas begin is hard to define and in practice the treatment of the infraorbital, cheek, and nasojugal areas must be undertaken concurrently, and in most situations the treated areas will overlap each other to a certain extent. In addition, it must be remembered that the ultimate goal of the procedure is creating youthful and attractive contour , not simply filling a specific area, and doing so requires treating multiple areas.
Fat grafting the tear trough ( Fig. 14 ) is simpler and faster to perform than fat transposition and septal reset, and we have largely abandoned these blepharoplasty procedures as have Little, Tonnard and Verpale, and others. And unlike when septal reset and fat transpositioning are performed, fat grafting allows one to fill not only the tear trough but also the infraorbital region, the cheek and midface, the upper orbit, the temple, forehead, and the radix and glabella and comprehensively rejuvenate the entire periorbital region . Fat grafting is aesthetically far more powerful and superior to a limited correction of the tear trough only.
Midface
The midface is a loosely defined triangular area bound by the infraorbital rim superiorly, the nasolabial fold medially, and the zygomaticus major muscle laterally. For several decades the aging change in this area has been mischaracterized as one of descent and mistakenly referred to as “midface ptosis” and as a result a variety of failed and/or largely abandoned procedures were conceived over the course of that time to “lift” what was mistakenly thought of as a “fallen” area. Often the early outcomes of these procedures looked satisfactory due to swelling but surgeons and patients were typically disappointed that once healing was complete and swelling had subsided a discernible improvement was not seen.
As experience with midface lifts accumulated, surgeons realized that the aging change in the midface consisted largely of deflation, and not descent , and a rethinking of how the midface is best treated occurred. It is now more widely recognized that one cannot lift an empty space, but instead must fill it, and fat grafting has taken a preeminent role in treatment of this aesthetically important area. Indeed, Tonnard and Verpale, Little, and others who all once advocated “lifting” the midface have abandoned it and acknowledged that the midface is best rejuvenated by fat grafting alone ( Fig. 15 ).
Practically speaking, the midface overlaps the infraorbital region, the tear trough, and the cheek (see Fig. 22 ), and when these adjacent areas are treated separate filling of the midface may not be needed. Fat grafting the midface when indicated corrects a hollow, ill, and unaesthetic orbital appearance that occurs with age by filling and strengthening it in ways that a midface lift cannot.
Special Circumstances that Demand Periorbital Fat Grafting
Proptotic ocular globe
The proptotic ocular globe or “negative vector” eye has presented a challenge to surgeons performing blepharoplasty since the inception of the procedure. Traditional upper blepharoplasty in which skin and fat is removed from the upper eyelid often results in a hollow upper orbit, overly high palpebral skin fold, and a distinctive “bug eye” stare or “frog eye” appearance. Traditional lower blepharoplasty in which fat was removed from the lower eyelid often compounds these appearances and precipitates lower lid retraction and scleral show and a “polar bear” look. In addition, canthopexy is generally ineffective in these patients. Periorbital fat grafting is often a better way to improve these patients’ ocular appearance and can disguise this problem and create a “neutral” vector oculomalar relationship ( Fig. 16 ). Treating the proptotic globe calls on the surgeon’s ability to recognize and treat multiple areas and not just spot treat one site.
Related posts:
 Treatment Options for Lower Eyelid Festoons
Treatment Options for Lower Eyelid Festoons
 Anatomic Trends and Directions in Periorbital Aesthetic Surgery
Anatomic Trends and Directions in Periorbital Aesthetic Surgery
 Complications of Periocular Dermal Fillers
Complications of Periocular Dermal Fillers
 The Treatment of Post-blepharoplasty Lower Eyelid Retraction
The Treatment of Post-blepharoplasty Lower Eyelid Retraction
 Eyelid and Periorbital Dermal Fillers
Eyelid and Periorbital Dermal Fillers
 Transcutaneous Blepharoplasty with Volume Preservation
Transcutaneous Blepharoplasty with Volume Preservation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


