Perioral Dermatitis: Introduction
|
Perioral dermatitis is characterized by small, discrete papules and pustules in a periorificial distribution, predominantly around the mouth. Because this condition can involve areas other than the perioral region, the term periorificial dermatitis has been proposed for this disorder.1,2 The classic presentation is an eruption with overlapping features of an eczematous dermatitis and an acneiform eruption. Although initially described in young women of 15–25 years of age, perioral dermatitis is now recognized to occur in children as well.3 A subset of perioral dermatitis shows granulomas when lesional skin is examined histologically. Several names have been used to describe this granulomatous form of perioral dermatitis, including granulomatous perioral dermatitis, facial Afro-Caribbean childhood eruption, and granulomatous periorificial dermatitis.2,4,5
Historical Aspects
The first reports describing perioral dermatitis appeared in the 1950s; various names were given to the condition, however, there was a lack of defining clinical criteria. In 1957, Frumess and Lewis described a “light sensitive seborrheid” that is generally accepted as the first account of what was later termed perioral dermatitis by Mihan and Ayres in 1964.6,7 Later descriptions by Cochran and Thomson8 and Wilkinson, Kirton, and Wilkinson9 further defined this disorder, and more recently the term periorificial dermatitis has been proposed.2 The condition was first described in children in the late 1960s.
Epidemiology
Adult perioral dermatitis predominantly affects women. Pediatric perioral dermatitis may have a slight female preponderance and is seen equally among those of different races.1,10 The granulomatous form of perioral dermatitis has been reported mostly in children of prepubertal age.5 Perioral dermatitis can occur as early as 6 months.1 An increased prevalence in African-American children has been reported, but more recent reviews do not support this finding.2,11
Etiology and Pathogenesis
A relationship of perioral dermatitis to the misuse of topical corticosteroids (fluorinated or nonfluorinated) has been well established.12 Patients often reveal a history of an acute steroid-responsive eruption around the mouth, nose, and/or eyes that worsens when the topical corticosteroid is discontinued. Dependency on the use of the topical corticosteroid may develop as the patient repeatedly treats the recurrent eruption. In other cases, the condition may worsen with the application of topical corticosteroids, especially in the granulomatous variant of perioral dermatitis, which usually occurs in prepubertal children.2 Perioral dermatitis has been reported in patients using inhaled corticosteroids13 and with inadvertent facial exposure to topical corticosteroids.14 However, perioral dermatitis is not always linked to topical corticosteroids.9 The exact cause of perioral dermatitis in these other cases is unclear. Although isolated reports of affected siblings exist,2,15 no clear genetic predisposition has been noted, nor have specific environmental exposures been consistently implicated. Of note, the disease is predominant in young women, yet no link to hormonal causes has been found. The initial reports of photosensitivity by Frumess and Lewis6 were not further substantiated, nor were theories of microbiologic causes such as infection with Candida, fusiform bacteria, or Demodex folliculorum.16 Cases of allergic contact with fluorides or other components in toothpaste and dentifrices have also been reported, however, use of these agents after clearing of the perioral dermatitis without further eruption has also been described. Patch testing in a small series of patients led to few positive results, and these were not considered relevant.9
In the past, authors have considered the relationship of perioral dermatitis to acne rosacea, however, the clinical features are distinct (see Section “Differential Diagnosis”). In perioral dermatitis, the histopathologic findings are variable and are dependent on the form of perioral dermatitis. In a histopathologic review of 26 patients with the nongranulomatous form, follicular spongiosis and eczematous changes were prominent features, suggesting that perioral dermatitis is distinct from rosacea.17 A lymphohistiocytic infiltrate and occasional plasma cells were noted in a perifollicular and perivascular distribution in this series. In granulomatous perioral dermatitis, histopathology demonstrates follicular hyperkeratosis, edema and vasodilatation in the papillary dermis, perivascular and parafollicular infiltrates of lymphocytes, histiocytes, and polymorphonuclear leukocytes with occasional epithelioid granulomas and giant cells, similar to the histopathologic changes in acne rosacea.5,18
Clinical Findings
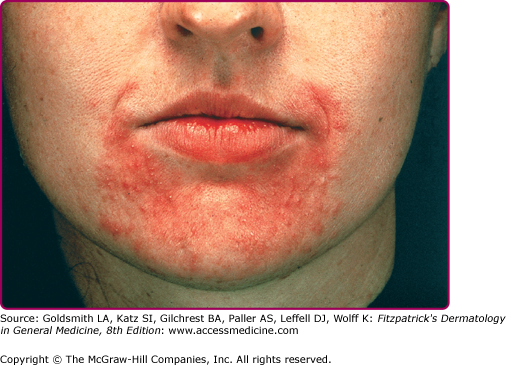
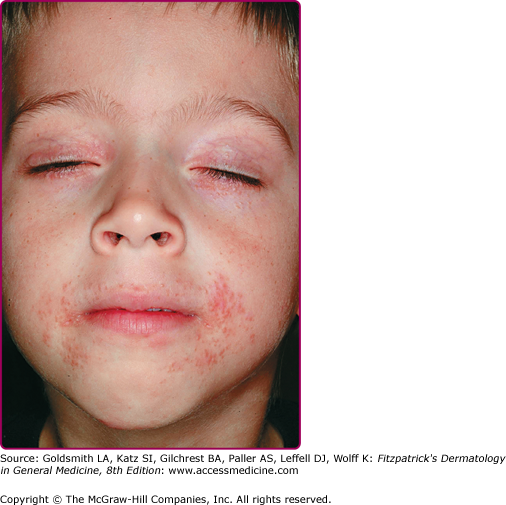
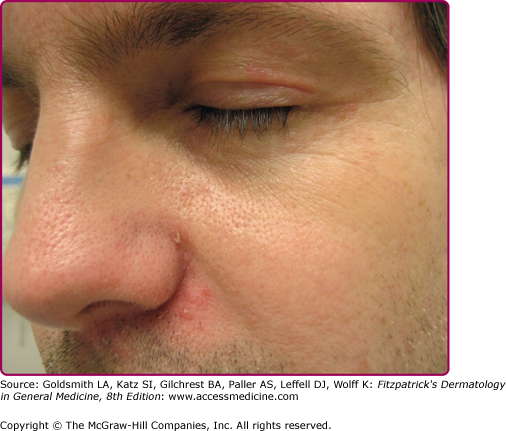
The primary lesions of perioral dermatitis are discrete and grouped erythematous papules, vesicles, and pustules (Figs. 82-1 and 82-2). The lesions are often symmetric but may be unilateral and appear in the perioral, perinasal, and/or periocular regions (Figs. 82-2 and 82-3 and eFigs. 82-3.1 and 82-3.2). In a retrospective review of 79 children with perioral dermatitis, isolated perioral involvement was present in only 39%, and in rare cases nonperioral regions were involved exclusively.1 Background erythema and/or scale may be present. A distinct 5-mm clear zone at the vermilion edge is well described (Fig. 82-2). The granulomatous variant of perioral dermatitis presents with small flesh-colored, erythematous, or yellow–brown papules, some with confluence, and shares the distribution of perioral dermatitis in adults (Fig. 82-3). In addition, lesions have been reported to appear on the ears, neck, scalp, trunk, labia majora, and extremities.1,11


Occasionally, an associated burning sensation or itching is reported, and intolerance to moisturizers and other topical products is described.1,9 In a few cases of granulomatous perioral dermatitis, an associated blepharitis or conjunctivitis has been reported.11 Systemic findings and regional lymphadenopathy are absent.








