Key points
- •
Reduction of scar burden and concealing of scars by placement in inconspicuous areas improves aesthetic outcomes in breast surgery.
- •
Periareolar incisions concealed in the breast skin–areola interface, while aesthetically advantageous, provide only limited access for breast reshaping or nipple repositioning. Correction of only mild ptosis and reductions <500 g are possible under the best of circumstances.
- •
Vertical scar breast techniques are well suited for reductions of <1500 g and correction of moderate breast ptosis.
- •
The extent to which pleasing aesthetic results can be achieved by periareolar and vertical scar breast techniques is heavily influenced by the quality of the breast gland and skin with more youthful breast and skin allowing for best results.
- •
Scar burden and visibility contribute only in part to overall aesthetic results in breast surgery. Breast shape, symmetry, and proportion to body habitus are equally important and efforts to limit scars may adversely affect the capacity to achieve other aesthetic goals.
Patient selection
Aesthetic results of periareolar or vertical scar breast techniques are heavily dependent on the quality of the breast gland and skin. Periareolar techniques are almost exclusively limited to younger patients with good skin thickness and elasticity. Firmer breasts with preserved integrity of Cooper’s ligaments are also desirable, especially if any amount of breast reshaping or reduction is to be performed. If significant atrophy of the breast gland is present an implant may be needed to fill the skin envelope before using a periareolar technique to reposition the nipple. Generally, correction of mild ptosis and reductions of up to 500 g of breast tissue are possible with a periareolar approach.
Vertical scar techniques are more versatile than periareolar techniques. Reductions of up 1500 g and correction of moderate ptosis are possible. These techniques allow for more extensive breast parenchymal rearrangement and hence even fatty breast can be supported by columns and pillars of repositioned breast gland. Youthful breast skin and gland is still desirable but not as limiting as in the periareolar approach. A firmer breast will hold shape better and hence give longer lasting results while more elastic skin will have a lessened tendency to form widened scars (which because of its location over the anterior breast is already prominent). As in the periareolar technique, an implant may be used if additional volume is required at the time of vertical scar mastopexy.
Periareolar operative techniques
Concentric mastopexy without parenchyma reshaping
In women with good skin thickness and elasticity, nipple ptosis is often mild. Unless there is an accompanying significant degree of glandular ptosis or breast atrophy, periareolar skin excision alone can effectively recentralize the areola over the breast mound. The nipple can be repositioned up to 3 cm without undue tension. In women with mild ptosis and glandular atrophy, placing an implant in the same setting fills the skin envelope providing additional lift.
Pre-operative preparation
In the standing position, the superior areola position is determined by measurement from the sternal notch 19–22 cm along the breast meridian. This point is marked for each breast and symmetry is confirmed by measurement from the sternum to the marked position. Differences in symmetry can be ‘split’ between the breasts with final adjustments of position based on the centering of the nipple over the breast mound.
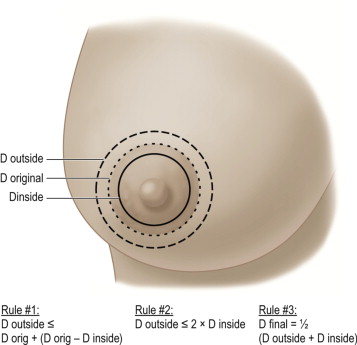
Based on the new areola position, a circular line of excision is marked. The diameter of the proposed line of excision (D outside ) based on the areolar diameter (D original ) and any amount of planned areolar reduction (D inside ) is constructed as defined by Spears ( Figure 12.1 ). The final diameter of the closure can be predicted ( Figure 12.1 Rule #3) for each breast and adjustments made to account for any asymmetry between the breasts.
Technique
Intraoperatively with the patient supine, the areola is distended and marked with an areolar sizer. The skin between the outer and inner circular marks is infiltrated using 0.5% lidocaine with 1 : 200 000 epinephrine and de-epithelialized. The caudal edge of exposed dermis is then incised at its outer border from 2 o’clock to 10 o’clock and elevated off the breast. This creates a dermal flap which reduces tension on the skin closure and may be folded underneath the areola to maintain projection.
Closure
A deep dermal permanent suture (4-0 gore-tex or mersilene) is placed in a running purse-string fashion along the breast skin edge and cinched to the final areolar diameter. Half-buried horizontal mattress 4-0 nylon sutures with the knot over the areolar skin are then placed tacking the areola to the breast skin. A running subcuticular 4-0 monocryl or PDS suture provides final skin closure.
Operative steps
- •
Infiltrate dermis between periareolar marks with local anesthetic containing epinephrine and de-epithelialize.
- •
Incise inferior border of de-epithelialized flap and tuck under areola.
- •
Cinch the breast skin down around the areola using a permanent suture run in the dermis as a purse-string cerclage.
- •
Approximate the areola and breast skin with half-buried mattress sutures and a running absorbable subcuticular suture.
The Benelli periareolar technique
The Benelli periareloar technique extends the periareolar approach to the breast to include a limited reduction of the breast gland. Removal of central and inferior glandular tissue followed by ‘reconization’ parenchymal rearrangement is accomplished through a periareolar incision. A decreased base diameter of the breast results and pushes the areola superiorly supported by breast parenchyma. This technique is limited to <500 g of glandular excision although a 1200 g excision has been reported with good results.
Pre-operative preparation
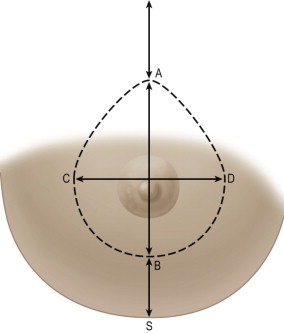
Pre-operative marks are made with the patient standing. The midline and the estimated meridian of the reshaped breast are marked. The estimated meridian intersects the clavicle 6 cm from the midline. The level of the inframammary fold is projected to the anterior breast with finger tips and the superior border of the new areolar position (point A) is marked 2 cm superior along the meridian. The future inferior border of the areola (point B) is marked with the patient supine 5–12 cm superior to the inframammary fold. The anticipated volume reduction and skin excision must be considered when identifying this point as a larger final volume of the breast will dictate a longer length. The medial and lateral limits of the proposed skin excision (points C and D respectively) are then placed equidistant from the meridian at a level between A and B with point C 8–12 cm lateral to the midline at the level of the sternum. Points A through D are then connected forming an ellipse. Point S is marked at the midpoint of the inframammary fold ( Figure 12.2 ). The opposite breast is marked in a similar fashion, insuring symmetry by the sternal notch to areola distance and distance from the midline along the sternum to areola. Simulation of the final closure from points A to B and points C to D is performed to ensure there is no excess tension.
Technique
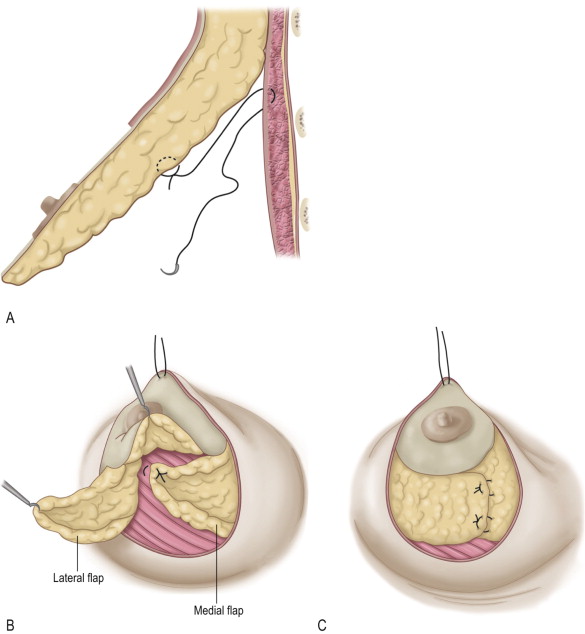
A wetting solution of 1000 mL saline mixed with 0.25 mg epinephrine and 20 mL of 2% lidocaine is infiltrated subcutaneously 3 cm outside the periareolar marks and into the prepectoral space. The areola is distended and marked under tension with a sizer. The skin between the sized areola and the marked ellipse is de-epithelialized. The de-epithelialized dermis is incised 1 cm from its outer border between the 2 o’clock and 10 o’clock positions. Subcutaneous dissection extending out from the incised ellipse follows over the upper outer, inferior, and medial breast being mindful to conserve adequate flap thickness to ensure blood supply ( Figure 12.3A ). Over the upper outer quadrant of the breast, dissection is more superficial to preserve extensions of the lateral thoracic artery.
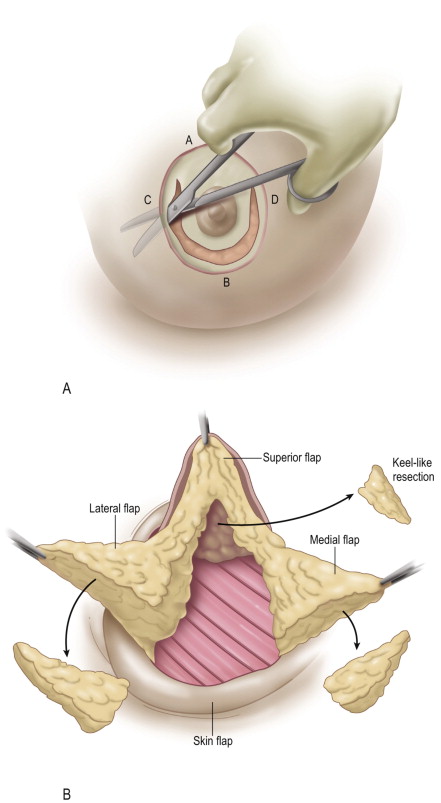
Glandular resection follows, beginning with a semicircular incision through the gland some 3 cm from the inferior areolar edge. The incision is carried deep to the level of the prepectoral space. The inferior gland is incised vertically beyond the breast meridian to the level of the fascia creating four flaps: (1) a superior dermatoglandular flap carrying the areola; (2) a glandular medial flap; (3) a glandular lateral flap; and (4) a detached skin flap ( Figure 12.3B ). The glandular flaps are trimmed being cautious of reduction along the distal ends of the flaps which will reduce their length. If the breast requires no reduction or parenchymal rearrangement, no trimming is performed.
Closure
The breast is reassembled beginning with suture elevation of the superior dermatoglandular flap high on the chest wall to the pectoralis fascia ( Figure 12.4A ). Trimmed medial and lateral flaps are then folded over one another with the medial flap rotated first and sutured to the pectoralis fascia. The lateral flap is folded over the medial flap and sutured in place forming a ‘cone’ of glandular tissue ( Figure 12.4B,C ). If no trimming of the medial and lateral flaps was performed, the edges of the flaps can be simply plicated and invaginated to cone the breast shape.
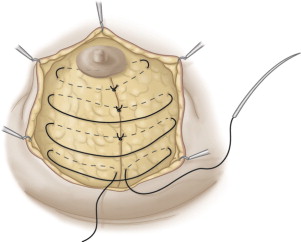
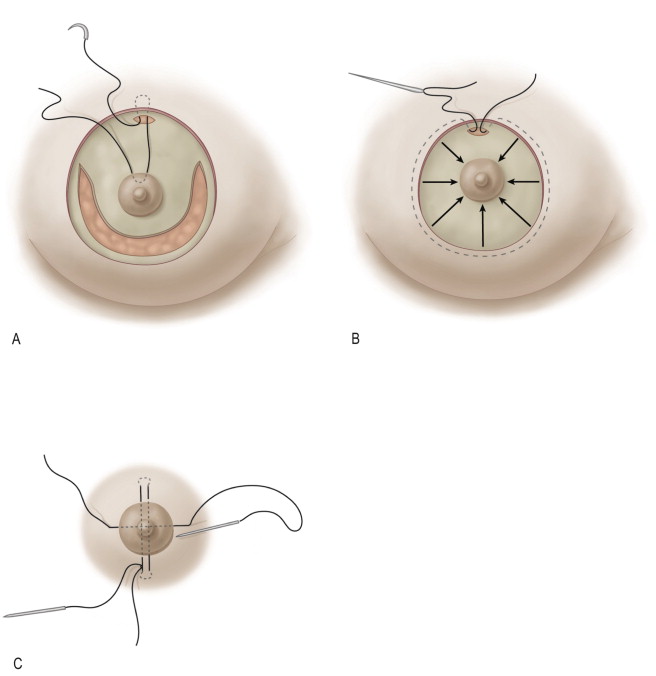
Additional coning of the breast is accomplished with ‘full-breast lacing’. Large-bite inverted sutures of braided 2-0 polyester are placed across the inferior gland as retention sutures. The sutures are tied under minimal tension and help maintain shape, particularly when the gland is fatty and less firm ( Figure 12.5 ). The deep dermal areolar undersurface is then suspended from the dermis of the superior border of the de-epithelialized ellipse with a suture passed through a small incision made at the 12 o’clock position ( Figure 12.6A ). The incision allows for the knot to be buried as the suture supports the areola without tension on the skin. A running intradermal permanent suture on a straight needle is then passed along the outer perimeter of the de-epithelialized ellipse through the 12 o’clock dermal incision. The suture is cinched down to the diameter of the areolar template and tied ( Figure 12.6B ). Diametrical transareolar U-stitches are then placed, anchored into the dermis of the breast skin edges, to help prevent areolar protrusion and better define the circular shape of the areola ( Figure 12.6C ). A 4-0 vicryl intradermal suture is run around the areola for final skin closure.
Operative steps
- •
Infiltrate subcutaneous and prepectoral spaces with dilute local anesthetic containing epinephrine 3 cm outside the planned area of excision.
- •
De-epithelialize periareolar skin between marks and then incise the de-epithelialized flap 1 cm from its outer edge between 2 and 10 o’clock.
- •
Undermine the skin over the upper outer, inferior and medial breast and then incise the inferior breast gland horizontally then vertically down to chest wall fascia to create four flaps.
- •
Suture the superior flap carrying the areola high on the chest wall to fascia.
- •
Trim excess gland tissue from medial and lateral gland flaps if needed and then secure the flaps over one another in a ‘criss-cross’ fashion giving addition support with placement of retention sutures.
- •
Cinch the periareolar breast skin down around the areola with a purse-string suture cerclage placed intradermally with the knot buried. Place additional transareolar ‘U’ stitches to support the areola and close skin with running subcuticular suture.
Góes periareolar technique with mesh support
The Góes periareolar technique supports the areola on a central dermatoglandular column created by excision of parenchyma superiorly and inferiorly. A mixed vicryl and polypropylene (Vipro II™) mesh is also placed which acts as an ‘internal brassiere’ providing long-term shape to the breast. Initially the mesh is palpable but softens over time as it is incorporated. The mesh does not interfere with mammography. Again, the degree of gland reduction is generally limited to <500 g and is best suited for younger patients with good skin quality.
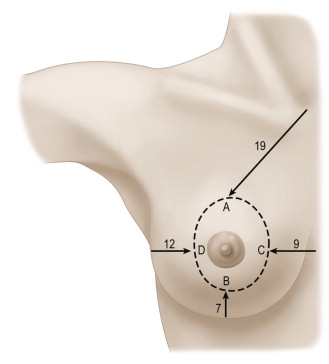
Pre-operative preparations
Four cardinal points are marked with the patient standing: the superior border of the new areola (point A) is marked 19–22 cm from the sternal notch; the new inferior border of the areola (point B) is marked 5–12 cm from the inframammary fold; the medial margin of excision (point C) lies 9 cm lateral of midline; and the lateral margin of resection (point D) lies 12 cm medial to the anterior axillary line. The four points are joined as an ellipse defining the limits of skin de-epithelialization ( Figure 12.7 ).